
Abstract
Objective
To compare the radiological and functional outcomes of the newly proposed lateral articular line approach with those of the traditional extended anterolateral approach in the management of Schatzker type II–III tibial plateau fractures involving the posterolateral quadrant.
Methods
This single-center retrospective cohort study included 90 patients who underwent open reduction and internal fixation using either lateral articular line approach (n = 45) or extended anterolateral approach (n = 45). Perioperative data (operative time, blood loss, and incision length), radiological outcomes (articular depression and posterior tibial slope), and functional recovery (Rasmussen knee scores and range of motion) were evaluated up to 12 months postoperatively.
Results
Compared with the extended anterolateral approach, the lateral articular line approach significantly reduced operative time (72.47 vs. 87.73 min, p < 0.001), blood loss (80.11 vs. 133.33 mL, p < 0.001), and incision length (6.0 vs. 15.0 cm, p < 0.001). The lateral articular line approach also achieved better reduction quality with smaller final articular depression (0.55 vs. 1.55 mm, p < 0.001) and yielded higher Rasmussen knee scores and greater range of motion at all follow-up assessments (all p < 0.05). Complication rates were comparable between the two groups.
Conclusion
The lateral articular line approach offers a minimally invasive and reliable alternative to the extended anterolateral approach for Schatzker type II–III tibial plateau fractures with posterolateral involvement, providing superior reduction quality, faster recovery, and less surgical trauma.
Keywords
Introduction
Tibial plateau fractures are one of the common complex fractures of the knee joint, accounting for approximately 1% of all fractures in the body.1,2 According to the Schatzker classification, type II fractures involve a split-depression of the lateral plateau, while type III fractures are pure depression fractures.3,4 In recent years, the increasing prevalence of high-energy trauma has led to a rising incidence of Schatzker type II and III fractures combined with posterolateral tibial plateau involvement. These fractures are more difficult to treat and pose greater challenges for prognosis.5,6 Due to the unique anatomical structure of the posterolateral plateau, conventional surgical approaches (such as the anterolateral approach) often fail to adequately expose the fracture fragments, which can easily lead to issues such as poor reduction of the articular surface, insufficient stability of internal fixation, and postoperative joint dysfunction.7–9
Currently, the optimal surgical management of Schatzker type II and III fractures with concomitant posterolateral plateau fractures remains controversial, and standardized criteria, particularly regarding the choice of surgical approach, are lacking. The extended anterolateral approach (EALA) is currently the most widely used technique, which provides good exposure of the lateral plateau. However, it offers limited visualization of the posterolateral area. This approach is also associated with significant trauma, involving extensive soft tissue dissection, which may compromise reduction quality and subsequent healing.10,11 To optimize exposure of the posterolateral plateau and reduce surgical invasiveness, our research team has proposed an innovative technique—lateral articular line approach (LALA)—designed to provide more direct and safer access to the posterolateral quadrant. 12 Preliminary studies indicate that this approach provides direct and adequate exposure of the posterolateral fracture region, thereby facilitating articular surface elevation and structural support reconstruction. However, high-quality evidence comparing its efficacy and safety with those of the traditional EALA remains limited.
Therefore, this study aimed to conduct a retrospective controlled analysis comparing LALA with EALA in the management of Schatzker type II and III fractures with concomitant posterolateral plateau involvement. This comparative analysis will focus on the quality of radiographic reduction, clinical outcomes, and perioperative safety. The study seeks to provide evidence-based support for the rational selection of surgical approaches and to guide clinical decision-making.
Methods
Study design
This is a single-center retrospective cohort study conducted in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines. Eligible patients with Schatzker type II or III tibial plateau fractures involving the posterolateral plateau were enrolled and divided into two groups based on the surgical approach they previously received: LALA and EALA groups. The study protocol was approved by our institution’s Ethics Committee (Approval No. 202307818). Given the retrospective design, the requirement for additional research-specific consent was waived, as all patients had already provided standard surgical consent prior to treatment.
Study participants
Inclusion criteria
We included patients who met the following criteria:
Radiologically confirmed (X-ray/computed tomography (CT)) diagnosis of Schatzker type II or III fracture involving the posterolateral plateau; Underwent primary open reduction and internal fixation using either LALA or EALA; Had complete preoperative and postoperative follow-up data with evaluable imaging studies; Completed a postoperative follow-up period of ≥12 months.
Exclusion criteria
We excluded patients who met any of the following criteria:
Presented with other ipsilateral lower limb fractures requiring surgical intervention or sustained multiple traumatic injuries; Had a history of surgery on the ipsilateral knee; Had significant comorbidities or neuromuscular diseases that could impact rehabilitation; Were lost to follow-up before the 12-month follow-up visit or had missing critical information.
Surgical groups and procedure overview
All surgeries were performed by the same senior orthopedic trauma surgeon. In the LALA group, the posterolateral quadrant was directly exposed using LALA. Depressed fracture fragments were elevated, with bone grafting performed when necessary, and then stabilized with a lateral locking plate (Figure 1).12,13 In the EALA group, patients underwent analogous reduction and fixation procedures using EALA (Figure 2). 13

(a) Incision for the lateral articular line approach; (b) photograph following reduction and internal fixation placement and (c) postoperative appearance of the incision.

(a) Incision for the extended anterolateral approach; (b) photograph following reduction and internal fixation placement and (c) postoperative appearance of the incision.
Outcome measures
The outcome measures of this study included perioperative parameters, radiographic outcomes, functional outcomes, and complications.
Perioperative parameters
Operative time (measured from skin incision to wound closure), estimated intraoperative blood loss (based on anesthesia records), and incision length (as documented in the surgical notes) were recorded.
Radiographic assessment
Knee CT was performed within 72 h postoperatively to assess the quality of initial reduction. Bilateral weight-bearing anteroposterior and lateral knee radiographs were obtained at the final follow-up (12 months ± 8 weeks) to evaluate the maintenance of reduction. The following parameters were measured by two assessors blinded to both patient group and assessment time point: (a) articular surface depression depth (mm) and (b) lateral posterior tibial slope (PTS, °). To evaluate measurement reliability, imaging data from 30 randomly selected patients were measured by both assessors to determine interobserver reliability. One assessor repeated the measurements on the same dataset after an interval of at least 2 weeks to calculate intraobserver reliability. The intraclass correlation coefficient (ICC(2,1)) model was used to calculate reliability coefficients and their 95% confidence intervals (CI). If reliability was good (ICC > 0.75), the average of the first measurements from both assessors was used for subsequent analyses. If the initial measurements for a given parameter differed beyond the predefined tolerance (>1 mm for depression depth and >2° for PTS), a third senior expert would arbitrate, and the arbitrated result would be used.
Functional assessment
By reviewing the electronic medical record system, the Rasmussen knee functional score and active range of motion (ROM, °) were collected preoperatively and at 1, 3, 6, and 12 months postoperatively. To account for variability in retrospective data collection, the following tolerance windows were defined: 1 month (±2 weeks), 3/6 months (±4 weeks), and 12 months (±8 weeks).
Complications
Recorded complications included surgical site infection, symptomatic deep vein thrombosis (DVT), implant failure, loss of reduction (defined as step-off or depression >2 mm), and reoperation.
Statistical analysis
Data analysis was performed using SPSS software (version 27.0). The normality of continuous variables was assessed using the Shapiro–Wilk test. Normally distributed data were presented as mean ± standard deviation and were compared using the independent-samples t-test. Non-normally distributed data were presented as median (interquartile range) and compared using the Mann–Whitney U test. Categorical variables were presented as frequency (percentage) and compared using the chi-square test or Fisher’s exact test, as appropriate. All statistical tests were two-sided, and a p-value of <0.05 was considered statistically significant.
Power analysis
A post-hoc power analysis was conducted based on the primary functional outcome (Rasmussen knee score at 12 months). Using the observed effect size (Cohen’s d = 1.42), a total sample size of 90 patients achieved a statistical power >99% at a two-sided α-level of 0.05. Power analyses were performed using G*Power (version 3.1).
Linear mixed-effects model
To account for repeated measurements and baseline variability, longitudinal functional outcomes were further analyzed using linear mixed-effects models. Patient ID was included as a random effect, while surgical approach, time, and their interaction were treated as fixed effects. Preoperative functional score, age, sex, and body mass index were included as covariates.
Results
Baseline characteristics and comparability
A total of 90 patients were ultimately included in this study, with 45 patients each in the LALA and EALA groups. The two groups showed no significant differences in preoperative baseline characteristics, including age, sex, injured side, Schatzker classification, and PTS of the uninjured side (all p > 0.05), confirming their baseline comparability (Table 1).
Comparison of baseline characteristics between the LALA and EALA groups.

Data are shown as mean ± SD or n (%). Independent-samples t-test was used for continuous variables and χ2 test for categorical variables. p < 0.05 was considered statistically significant.
EALA: extended anterolateral approach; LALA: lateral articular line approach; PTS: posterolateral tibial slope.
Comparison of perioperative parameters
The LALA group demonstrated statistically significant superiority over the EALA group across all perioperative parameters (Table 2). Specifically, the LALA group had a significantly shorter operative time (72.47 ± 6.37 vs. 87.73 ± 10.59 min, p < 0.001), significantly less intraoperative blood loss (80.11 ±9.14 vs. 133.33 ± 15.74 mL, p < 0.001), and a significantly shorter incision length (median: 6.0 cm (interquartile range (IQR): 5.5, 7.0) vs. 15.0 cm (IQR: 14.0, 16.0), p < 0.001).
Comparison of perioperative outcomes between the LALA and EALA groups.

Normally distributed variables are presented as mean ± SD and compared using independent-samples t-test. Non-normally distributed variables are presented as median (IQR) and compared using Mann–Whitney U test.
EALA: extended anterolateral approach; LALA: lateral articular line approach; IQR: interquartile range.
Comparison of postoperative functional recovery
Postoperative functional assessment outcomes revealed that the LALA group demonstrated significant advantages in knee joint functional recovery compared with the EALA group (Table 3). No significant difference in knee functional scores was observed between the two groups preoperatively (p = 0.490). However, as early as 1 month postoperatively, the LALA group exhibited significantly higher scores than the EALA group (16.04 ± 1.38 vs. 15.09 ± 1.41, p = 0.002). This advantage was maintained at the 3-, 6-, and 12-month final follow-up assessments (all p < 0.001). For the active ROM, the preoperative values were comparable between the two groups (p = 0.668). In the early postoperative phases (1 and 3 months), the LALA group achieved a significantly faster ROM recovery (e.g. at 3 months: 125° (IQR: 120, 130) vs. 90° (IQR: 85, 95), p < 0.001). Although the EALA group showed substantial improvement at 6 and 12 months, the LALA group maintained a statistically superior ROM at the final follow-up (125° (IQR: 120, 130) vs. 120° (IQR: 115, 125), p < 0.001).
Functional outcomes between the LALA and EALA groups.

Continuous data are presented as mean ± SD or median (IQR), according to distribution. Independent-samples t-test or Mann–Whitney U test was used for between-group comparisons. p < 0.05 indicates statistical significance.
EALA: extended anterolateral approach; LALA: lateral articular line approach; postop: postoperatively; IQR: interquartile range.
Radiographic outcomes
Radiographic assessment revealed differences in the quality and maintenance of reduction between the two surgical approaches (Table 4). Regarding the immediate postoperative PTS, no significant difference was found between the two groups (p > 0.05). However, at the final follow-up, the PTS in the EALA group was significantly greater than that in the LALA group (9.74° ± 1.10° vs. 9.22° ± 0.89°, p = 0.015), suggesting a more pronounced loss of reduction in the EALA group. Even in the immediate postoperative period, the articular surface depression depth was significantly greater in the EALA group than in the LALA group (0.70 mm (IQR: 0.50, 0.90) vs. 0.25 mm (IQR: 0.20, 0.40), p < 0.001). By the final follow-up, the depression depth had increased slightly in both groups but remained significantly greater in the EALA group (1.55 mm (IQR: 1.30, 1.80) vs. 0.55 mm (IQR: 0.40, 0.70), p < 0.001).
Radiographic outcomes between the LALA and EALA groups.

PTS values are expressed as mean ± SD and compared using independent-samples t-test. Depression depth is expressed as median (IQR) and compared using Mann–Whitney U test.
EALA: extended anterolateral approach; LALA: lateral articular line approach; postop: postoperative; IQR: interquartile range.
Measurement reliability
All radiographic measurements demonstrated excellent reliability (Table 5). Both intra- and interobserver reliability, assessed using ICC, were above 0.90 (indicating excellent reliability), with all p values <0.001, confirming that the measurements were highly consistent and reliable.
ICC for the reliability of radiographic measurements.

ICCs were calculated using a two-way random-effects model for absolute agreement: ICC(2,1) for single measures and ICC(2,k) for the mean of k = 2 raters. Analyses were based on 30 randomly selected images. Interpretation: <0.50 = poor, 0.50–0.75 = moderate, 0.75–0.90 = good, and >0.90 = excellent.
ICC: intraclass correlation coefficient; CI: confidence interval; PTS: posterolateral tibial slope.
Linear mixed-effects model analysis
After adjustment for baseline functional status and demographic covariates, linear mixed-effects modeling demonstrated that surgical approach remained an independent predictor of both Rasmussen knee score and ROM over time. The LALA was associated with significantly higher Rasmussen scores (β = 1.21, 95% CI: 0.86–1.56, p < 0.001) and greater ROM (β = 12.6°, 95% CI: 9.1–16.1, p < 0.001). A significant interaction between surgical approach and time indicated faster and more sustained functional recovery in the LALA group (Table 6).
Linear mixed-effects model analysis of Rasmussen knee score and ROM.
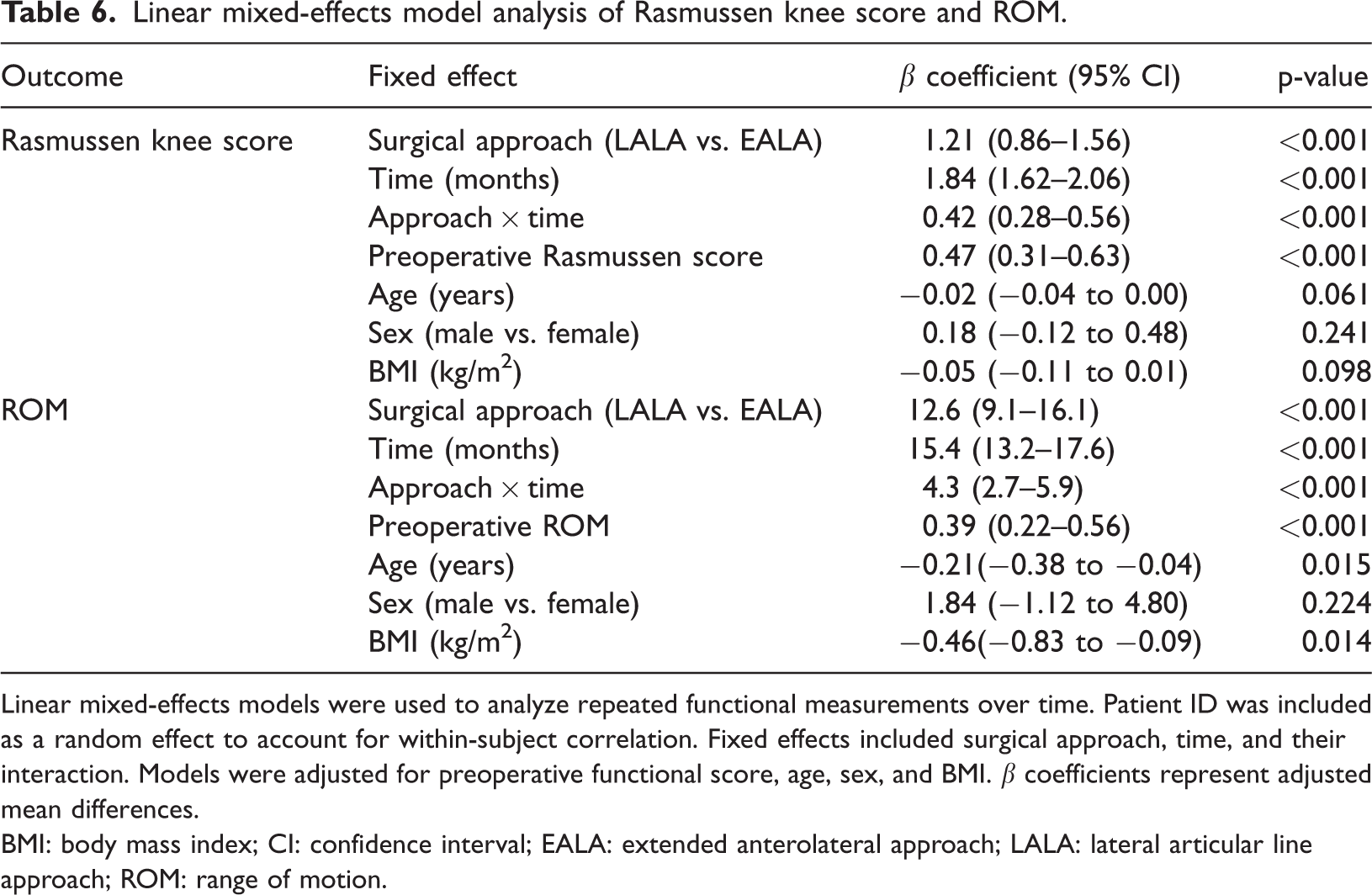
Linear mixed-effects models were used to analyze repeated functional measurements over time. Patient ID was included as a random effect to account for within-subject correlation. Fixed effects included surgical approach, time, and their interaction. Models were adjusted for preoperative functional score, age, sex, and BMI. β coefficients represent adjusted mean differences.
BMI: body mass index; CI: confidence interval; EALA: extended anterolateral approach; LALA: lateral articular line approach; ROM: range of motion.
Complications
During the postoperative follow-up period, neither group recorded any cases of deep surgical site infection, symptomatic DVT, implant failure, loss of reduction (defined as >2 mm), or the need for reoperation due to complications.
Discussion
The principal finding is that in Schatzker type II–III tibial plateau fractures with posterolateral involvement, LALA achieved superior outcomes compared with EALA. Specifically, LALA was associated with higher-quality radiographic reduction, improved midterm knee functional recovery, and significantly reduced surgical trauma, without increasing the risk of complications. These findings provide a novel and effective solution for managing this clinically challenging fracture pattern.
Schatzker type II and III tibial plateau fractures with concomitant posterolateral involvement often present as complex intra-articular injuries. 14 A study by Xiang et al. 15 indicated that approximately 20% of tibial plateau fractures involve the posterolateral quadrant, with approximately 7% being isolated posterolateral plateau fractures. These fractures frequently occur when force is applied to the knee in a flexed position. The typical injury mechanism involves impaction of the lateral femoral condyle against the posterolateral tibial plateau, resulting in a split or depression of the articular surface.16,17 Consequently, fracture fragments often assume a pyramidal configuration, characterized by a narrow articular surface, short and deep fracture lines, and varying degrees of depression, substantially increasing the difficulty of reduction and fixation and making it a major therapeutic challenge. The posterolateral tibial plateau, located in the posterolateral quadrant of the proximal articular surface, is surrounded by complex anatomical structures with critical soft tissue attachments, which further complicate intraoperative exposure and manipulation. Laterally, the prominent fibular head serves as the attachment point for the lateral collateral ligament and the biceps femoris tendon, both of which transverse the posterolateral plateau and create a natural anatomical barrier. 18 Moreover, the posterolateral plateau is covered by structures such as the popliteus tendon, popliteofibular ligament, and the posterolateral corner complex of the joint capsule.19,20 In addition, the close proximity of the popliteal artery, popliteal vein, and common peroneal nerve to the posterior tibia and fibular neck further increases the complexity and risk associated with surgical exposure.21,22
The anterolateral approach, characterized by familiar anatomy and technical simplicity, is a classic surgical method for Schatzker type I–III tibial plateau fractures and has been widely adopted in clinical practice. This approach avoids the major neurovascular structures within the popliteal fossa, thereby reducing the risk of iatrogenic injury. However, visualization of the posterolateral plateau is inherently limited because of obstruction by the fibular head and surrounding soft tissues. Even with soft tissue retraction, this region frequently remains a blind spot in the surgical field, thereby increasing the difficulty of achieving reduction and internal fixation.22–25 To overcome this limitation, Chen et al. 26 proposed an extended anterolateral incision designed to enlarge the surgical field, which partially improves exposure of the posterolateral plateau. Nevertheless, despite this modification, direct visualization and fixation of the posterolateral plateau remain suboptimal.27,28
To address the aforementioned challenges, our research team proposed LALA as an innovative surgical technique. This approach is designed to optimize surgical field exposure, enhance reduction accuracy, and minimize soft tissue disruption while preserving the critical stabilizing structures of the knee joint, thereby facilitating postoperative functional recovery. Through a retrospective controlled study, this research compared the clinical efficacy and safety of LALA with those of the traditional anterolateral approach for the treatment of Schatzker type II and III tibial plateau fractures with concomitant posterolateral plateau involvement. The study optimized the strategy for selecting surgical approaches and provided evidence-based support for clinical decision-making.
Importantly, the functional outcomes observed in this study were not only statistically significant but also clinically meaningful. Previous studies have suggested that a change of ≥3 points in the Rasmussen knee score and an increase of ≥10° in knee ROM represent the minimal clinically important difference (MCID) for patients with tibial plateau fractures.29,30 In our cohort, the LALA group consistently exceeded these thresholds compared with the EALA group at all follow-up intervals. At the 12-month follow-up, for example, the mean difference in Rasmussen score was approximately 3.5 points, while the ROM advantage was approximately 15°, both surpassing the established MCID criteria. These findings suggest that the observed differences are not only statistically significant but also clinically meaningful, translating into tangible functional benefits in daily activities and rehabilitation.
The results of this study indicate that compared with EALA, LALA demonstrates superior outcomes in terms of radiographic reduction quality and postoperative functional recovery (p < 0.05). In addition to achieving higher Rasmussen scores and greater ROM, LALA was associated with significantly shorter operative time, reduced intraoperative blood loss, and a smaller surgical incision, without increasing the complication rate (p < 0.05). These findings are consistent with those reported by Li et al., 31 who also identified insufficient exposure of the posterolateral region when using EALA. Importantly, this study is the first controlled comparative analysis to demonstrate that the enhanced exposure provided by LALA translates into measurable improvements in functional outcomes and reduced surgical trauma. This finding substantially advances the current understanding, suggesting that the LALA is not merely a modification of the anatomical approach but a superior strategy capable of comprehensively improving perioperative outcomes and patient recovery. Consequently, this study provides robust empirical evidence supporting the consideration of LALA as a preferred option in the treatment of such fractures.
Furthermore, this study is the first to propose and validate the clinical value of LALA. The results highlight three primary advantages of this technique. 1. Optimized surgical field exposure. Compared with EALA, LALA provides direct visualization of the posterolateral plateau, offering a clearer view of the surgical field and overcoming the limitations associated with soft tissue retraction. 2. Reduced soft tissue trauma. Unlike EALA, LALA requires a smaller incision and causes less soft tissue damage, which helps preserve knee joint stability and reduces the risk of postoperative joint instability and stiffness. 3. Enhanced postoperative rehabilitation. By minimizing surgical trauma, patients achieve a greater early postoperative range of knee motion, contributing to higher early Rasmussen knee function scores and facilitating overall rehabilitation. These mechanisms likely explain why patients in the LALA group demonstrated statistically significant improvements in Rasmussen knee function scores at 1, 3, 6, and 12 months postoperatively compared with those in the anterolateral approach group (p < 0.05). However, given the relatively short follow-up period (only 12 months), further research is required to evaluate long-term functional outcomes.
This study has several limitations. First, as a retrospective study, although statistical models were applied to adjust for known confounding factors, the retrospective design may still be subject to unmeasured biases. Second, the sample size was relatively small, particularly for outcome measures with low incidence, such as complications, which may result in insufficient statistical power. Third, the follow-up period was short (12 months), preventing assessment of the long-term impact of the two surgical approaches on arthritis development and knee function. Future large-sample, multicenter, prospective randomized controlled trials with extended follow-up are warranted to further validate these findings.
Conclusion
This study demonstrates that for the treatment of Schatzker type II–III tibial plateau fractures with posterolateral involvement, LALA represents a minimally invasive, efficient, and reliable alternative that is superior to the traditional EALA. By providing more direct and adequate exposure, LALA enables more precise fracture reduction and stable fixation, resulting in superior midterm functional outcomes with a favorable safety profile. Despite its limitations, these findings provide robust evidence supporting the clinical application of LALA and suggest a promising approach for optimizing the management of these complex fractures.
Footnotes
Acknowledgment
None.
Author contributions
All authors made substantial contributions to this study. Zhang and Hu contributed to the study conception and design. Zhang and Hu were responsible for data collection and analysis. Zhang drafted the manuscript. Hu critically revised the manuscript for important intellectual content. All authors read and approved the final version of the manuscript and agree to be accountable for all aspects of the work.
Data availability statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Potential conflicts of interest and funding sources
The authors declare that there is no conflict of interest.