
Abstract
Fat embolism syndrome (FES) is a complication of long bone fractures that often occurs within 72 hours of injury. Early-onset isolated cerebral fat embolism is catastrophic and rarely reported. We herein present a rare case of delayed-onset isolated cerebral FES that developed 10 days after definite fixation of a left tibial plateau fracture. A 70-year-old woman was injured in a traffic accident and diagnosed with a left tibial plateau fracture. However, she developed sudden loss of consciousness (E4V1M1) and quadriplegia 10 days after fracture fixation. Her vital signs showed no respiratory distress. Diagnosis of isolated cerebral FES was made based on magnetic resonance imaging of the brain, the findings of which were compatible with the clinical neurological findings. After supportive care and rehabilitation, her consciousness became clear on the second day of admission, and her consciousness changed to E4V5M6. She gradually regained strength in her right limbs but had residual left limb paraplegia. Isolated cerebral FES should always be considered for patients who develop a change in consciousness, even beyond 72 hours after injury. Imaging may not initially show definitive abnormalities. Repeated magnetic resonance imaging should be considered if the initial clinical presentation does not fully meet Gurd’s criteria.
Keywords
Introduction
Fat embolism syndrome (FES), first reported by Zenker in 1861, 1 is a rare complication of long bone fractures that often occurs within 12 to 72 hours of injury. 2 Other causes of FES include trauma-related pelvic fractures, fractures of other marrow-containing bones, and orthopedic procedures. However, conditions unrelated to trauma can also reportedly cause FES, including pancreatitis, diabetes mellitus, osteomyelitis, and bone tumor lysis. 3
Fat embolism may occur with or without symptoms, especially if the intramedullary contents are disturbed during surgery. Because FES may not manifest symptoms, its incidence cannot be precisely estimated. However, incidence rates of FES ranging from <1% to 29% have been reported.4,5 The two main theories for the formation of fat embolism are the mechanical theory, which emphasizes vascular obstruction, and the biochemical theory, which emphasizes the inflammatory response that results from the trauma and leads to the development of embolized fat tissue. 6 Multiorgan dysfunction may occur, causing FES and presenting as a clinical triad of hypoxia, change of consciousness, and petechiae. The size and quantity of lipid droplets and the level of systemic involvement may correlate with the severity of FES. 7 Respiratory symptoms are reportedly the earliest signs of fat embolism and occur in 75% of patients.
Since 1974, an incidence rate of 10% has been reported for isolated cerebral FES with primary neurological deficits. 7 A change in consciousness occurs in up to 86% of patients with manifestations ranging from headache to coma.4,5,8 Two cases of early-onset FES have been reported at 3 hours and <12 hours post-injury, respectively.9–11 Although the neurological deficit is thought to be transient and reversible in most cases, the condition may be complicated by misdiagnosis or delayed diagnosis. 12
No specific treatment strategy other than supportive care has been reported to date. Therefore, prevention and early diagnosis are important. Early open reduction and surgical fixation, rather than conservative treatment, may decrease the risk of fat embolism but cannot eliminate FES. Internal fixation by a plate system or external skeletal fixation have some advantages over internal fixation by an intramedullary nailing device, which is likely to elevate the intramedullary pressure and accelerate release of fat emboli. 13 Early-onset isolated cerebral fat embolism is catastrophic and rarely reported. We herein present a rare case of delayed isolated cerebral FES that developed 10 days after definite fixation of a left tibial plateau fracture.
Case report
A 70-year-old nonsmoking woman with a history of hypertension and parkinsonism was injured in a traffic accident involving the collision of a taxi with a pedestrian, leading to deformity in her left knee. Distal sensation, motor function, and circulation were intact. The patient’s Injury Severity Score was 4. A left tibial plateau fracture with pure lateral depression (AO/OTA type 41B2, Schatzker type III) was diagnosed according to a series of radiographs and a computed tomography (CT) scan (Figure 1(a)–(d)). Preoperative echocardiography showed a good left ventricular ejection fraction without a left atrial thrombus and no evidence of a septal defect. Because of the relatively high-energy trauma, we waited 2 days for the soft tissue swelling to subside, and the patient finally underwent open reduction and internal fixation based on stable vital signs and clear consciousness. She was placed in the supine position under epidural anesthesia, and the fracture was reduced by filling the bone defect with an allograft followed by locking plate fixation (Figure 1(e), (f)). The postoperative course was smooth and accompanied by application of a long leg splint for immobilization. She was discharged when her wound had stabilized and her hemodynamic status had normalized.

Preoperative and postoperative radiographs and computed tomography images of the left knee. (a–d) Preoperative anteroposterior and lateral views of the left knee. (e, f) Postoperative anteroposterior and lateral radiographs.
On the 10th postoperative day, she received her first follow-up at the outpatient department. A reddish surgical wound with turbid discharge was noted. Focal surgical wound infection was observed, and intravenous antibiotic treatment was arranged. However, her consciousness status acutely changed from clear to unresponsive. Physical and neurological examination revealed that her Glasgow coma scale score was E4V1M1, and she became dull, mute, and nearly quadriplegic. Her respiratory pattern was smooth without desaturation (respiratory rate, 18 breaths/minute; oxygen saturation, 99% on room air). Her blood pressure was 195/110 mmHg with tachycardia (115 beats/minute). No fever was initially observed. An elevated C-reactive protein concentration, anemia, and a mildly elevated creatinine concentration were also detected. Her disseminated intravascular coagulation profile revealed a low fibrinogen concentration and high fibrin degradation product and D-dimer concentrations. Her blood gas analyses, blood examinations, and biochemical findings were within the reference ranges (Table 1).
Laboratory findings.
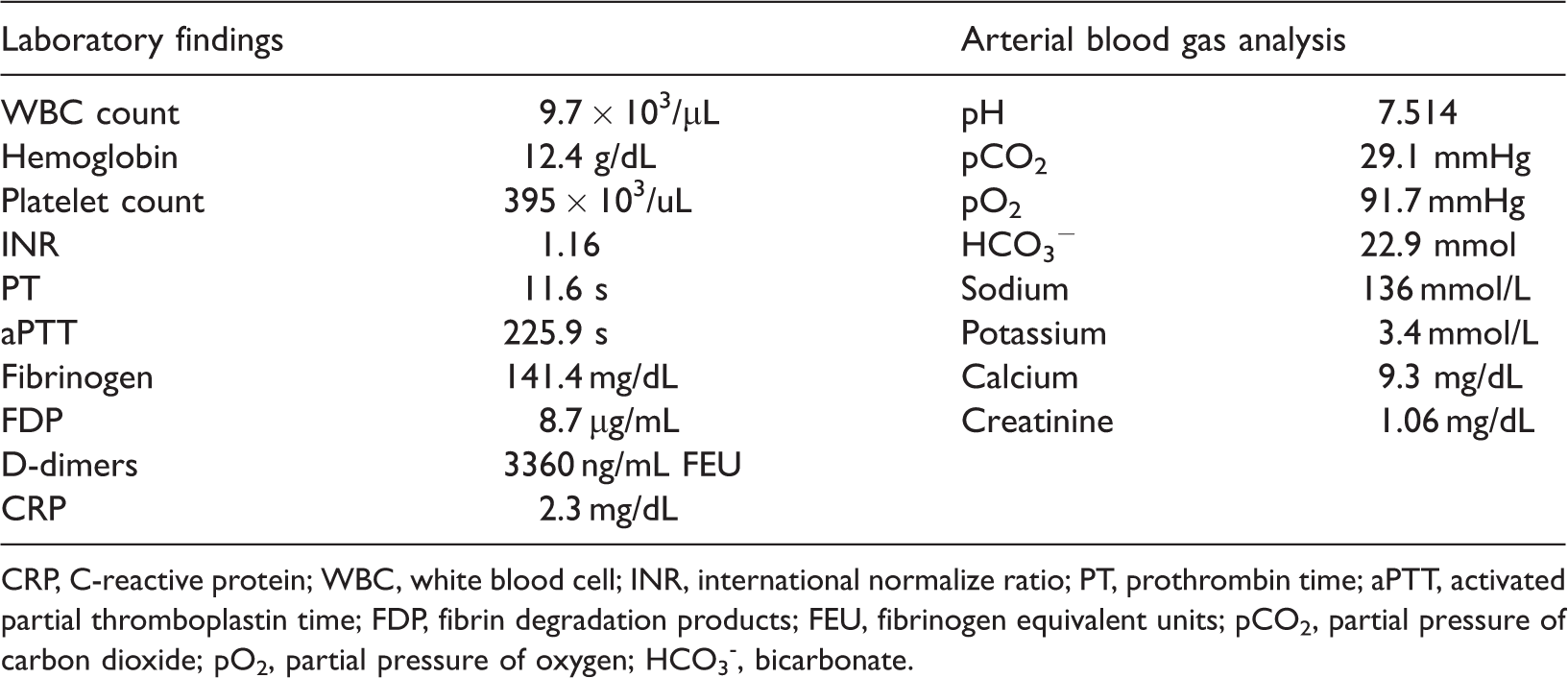
CRP, C-reactive protein; WBC, white blood cell; INR, international normalize ratio; PT, prothrombin time; aPTT, activated partial thromboplastin time; FDP, fibrin degradation products; FEU, fibrinogen equivalent units; pCO2, partial pressure of carbon dioxide; pO2, partial pressure of oxygen; HCO3-, bicarbonate.
Chest X-ray (Figure 2(a)) and brain CT (Figure 2(b)) demonstrated no significant findings. Magnetic resonance imaging (MRI) performed 3 hours after the loss of consciousness (Figure 3(a)) revealed multiple tiny foci of high signal intensity on diffusion-weighted imaging (DWI) at the cortex of the bilateral frontal and right parietal lobes. Based on the images, which involved the bilateral hemispheres, septic emboli or cerebral fat embolism were considered. Twenty-one hours after her change in consciousness, her fever flared up to 38.6°C. Gurd’s criteria were reached with satisfaction of one major criterion (cerebral symptoms in a patient with non-head injury) and four minor criteria (tachycardia, fever, renal changes, and drop in hemoglobin). Repeated echocardiograms also showed no thrombus formation or septal defect.

(a) Chest radiograph and (b) computed tomography image of the brain on the 10th postoperative day.
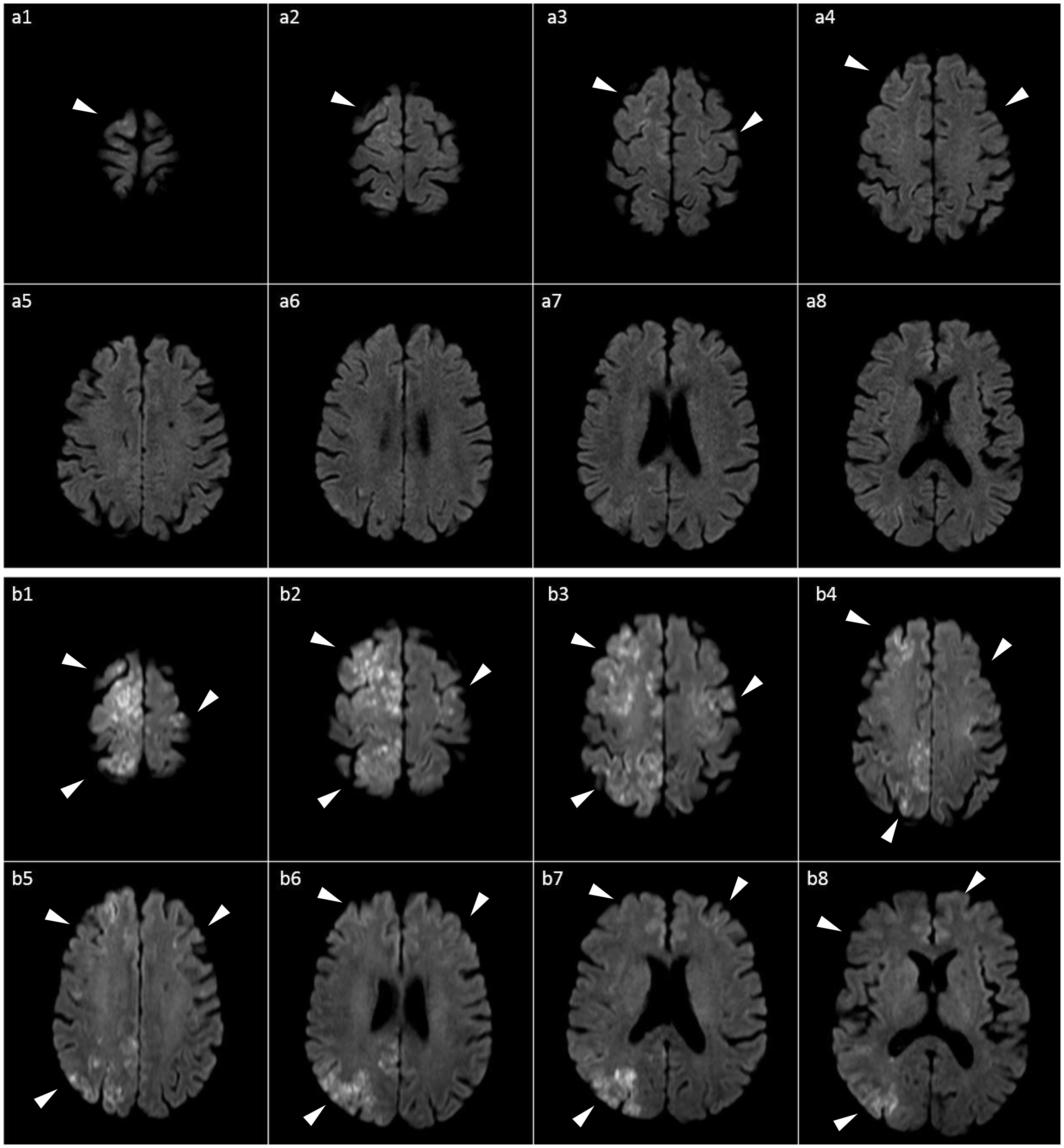
Magnetic resonance imaging series of the brain. (a) Diffusion-weighted image 3 hours after loss of consciousness. (b) Diffusion-weighted image 12 hours after loss of consciousness.
Carotid ultrasound showed no significant carotid atherosclerosis. Repeat brain MRI performed 12 hours after her change in consciousness (Figure 3(b)) showed multiple confluent cortical and subcortical lesions with restrictive diffusion and hyperintensity in the bilateral cerebral hemispheres on DWI, which was compatible with acute cerebral fat embolism.
The patient was admitted to the intensive care unit. She was treated with aspirin (100 mg daily) accompanied by adequate hydration and additional dexamethasone for supportive care. Her consciousness became clear on the second day of admission, and her Glasgow coma scale score changed to E4V5M6. She gradually regained strength in her right limbs but had residual left limb paraplegia (Medical Research Council muscle power score: 4, right upper; 4, right lower; 1, left upper; and 1, left lower). Debridement of the infected wound was arranged on the third day of admission, and intravenous antibiotics (vancomycin and ceftazidime) were administered for wound infection caused by Staphylococcus capitis. The blood culture was negative. On the 27th day of admission, the patient was discharged. She had clear consciousness with residual left limb paraplegia (Medical Research Council muscle power score: 4, right upper; 4, right lower; 1, left upper; and 1, left lower). Further rehabilitation was arranged.
We obtained verbal informed consent from the patient, and she understood that information regarding her diagnosis, laboratory and imaging data, and treatment course were being collected for publication. All patient details have been completely deidentified. This case report conforms to the CARE guidelines. 13
Discussion
Cerebral fat embolism is commonly reported in younger patients with long bone fractures, especially femoral and tibial fractures.12,14–16 To the best of our knowledge, most of the recently reported cases described early-onset embolism. The current report is the first to describe this condition in an older patient who developed extremely late-onset isolated cerebral fat embolism almost 12 days post-injury and 10 days after fixation of the proximal tibial fracture using a plating system with evidence obtained by a thorough MRI series. Thus, this case is extremely rare.
Currently, FES can be diagnosed according to the major and minor diagnostic criteria proposed by Gurd and Wilson. 17 A positive diagnosis of FES is suggested if two major criteria or one major criterion and four minor criteria are met.18,19 The fat embolism index score proposed by Schonfeld is also helpful and is based on seven clinical signs; a positive diagnosis of FES is suggested if a cumulative score of ≥5 is achieved during the first 3 days of hospitalization.4,20
Patients with isolated cerebral fat embolism have no respiratory dysfunction but exhibit a change of consciousness, which is usually accompanied by new-onset neurological deficit, apathy, convulsion, hallucination, facial palsy, or hemiplegia. Although the patient in the current case did not initially meet Gurd and Wilson’s criteria 17 (only one major and three minor criteria were met: cerebral symptoms in a patient with non-head injury, tachycardia, renal changes, and drop in hemoglobin), cerebral fat embolism was strongly considered because the patient presented with sudden unresponsiveness, dullness, and muteness with quadriplegia 10 days after fixation of the left tibial plateau fracture. Her fever developed 21 hours after her consciousness change; thus, the patient met the diagnostic criteria for FES. Blunt carotid artery injury and vertebrobasilar artery thrombosis also need to be considered, especially in patients with no history of head trauma.21,22 In the current case, carotid ultrasound showed no significant carotid atherosclerosis; however, slight atherosclerosis around the right vertebrobasilar artery was detected, which may have had some correlation with the cerebral fat embolism. However, one study demonstrated that bone strength is negatively associated with the bone marrow fat volume, meaning that poor bone quality in association with osteopenia or osteoporosis tends to cause a more comminuted fracture pattern as seen in our patient (AO/OTA type 41B2, Schaztker type III) and may have some correlation with an elevated risk of FES because of the increasing bone marrow fat fraction. 23 Intraoperatively, we observed the release of a large amount of adipose tissue when performing bony procedures. Additionally, the risk of FES was further elevated by postoperative wound infection and osteomyelitis. 24
The diagnostic criteria for cerebral fat embolism are not well documented. To date, MRI has been considered the most sensitive technique for the diagnosis of cerebral fat embolism compared with cerebral CT examination, which usually produces negative findings with the exception of diffuse edema. 12 However, CT is still important because of its ability to rapidly exclude other conditions that alter patients’ mental status.25,26 Typical findings of acute cerebral FES were studied by Parizel et al., 21 who identified the starfield pattern (multiple small areas of high signal intensity appearing as bright spots on a dark background) by diffusion-weighted MRI. T2-weighted MRI scans may show multiple small hyperintense intracerebral lesions several days after injury, which play a limited role in early diagnosis. However, it may be difficult to differentiate cerebral fat embolism from demyelinating disease or post-traumatic diffuse axonal injury.27,28 Thus, repeat brain MRI may be needed when a patient’s clinical presentation is not compatible with imaging findings, especially when the first MRI examination is performed within 6 hours (early hyperacute stage) of symptom onset.
Our patient had an acute embolic infarction pattern based on the presence of hyperintense signals on DWI, which involved the bilateral hemispheres. The two main differential diagnoses were septic emboli and cerebral fat embolism. Septic emboli were less likely because the infection was localized, the blood culture was negative, no active lung lesion was found by chest X-ray examination (Figure 2(a)), and echocardiography showed no evidence of a septal defect. The diagnosis was confirmed based on Gurd’s criteria, the typical MRI pattern, physical examination results, laboratory findings, results of diagnostic modalities (chest X-rays and echocardiography), and discussions with the radiologist and neurologist. Furthermore, this is the first case in which the process of development of a cerebral fat embolism was successfully recorded. Although the first MRI performed 3 hours after loss of consciousness had typical DWI findings showing multiple tiny foci of high signal intensity at the cortex of the bilateral frontal and right parietal lobes, which are highly indicative of fat embolism, the signal was too minute. MRI was repeated the next day and showed progressive hyperintense cortical and subcortical lesions in the bilateral cerebral hemispheres, which was compatible with the diagnosis of isolated cerebral FES.
In addition to the clinical presentation and imaging findings, laboratory tests offer some minor hints. A decreasing hemoglobin concentration and thrombocytopenia have been reported, along with hypofibrinogenemia and features of disseminated intravascular coagulation, such as a prolonged prothrombin time.20,29 Hypocalcemia is thought to be caused by the affinity between fatty acids and calcium or elevated serum lipase, but this is not well documented. The binding of free fatty acids to albumin may also cause hypoalbuminemia.20,30 Although the presence of hypoalbuminemia in our case may have been due to relatively poor nutrition after fracture fixation, it may also be an indicator of FES.
The reported mortality rate of FES ranges from 5% to 15%, and death is mainly due to pulmonary dysfunction such as acute respiratory distress. 31 Supportive care is considered the mainstream treatment for FES.10,32 Even a patient in a prolonged coma due to cerebral fat embolism can achieve complete recovery under adequate ventilatory support and prolonged intensive care. 33
Although our patient showed late-onset isolated cerebral fat embolism, we confirmed the diagnosis based on our initial suspicion within a very short period with almost no delay, facilitating the administration of proper treatment. She achieved good recovery of her mental status but had residual weakness in the left limbs after adequate supportive care. Long-term follow-up is needed for the recovery of limb weakness.
In conclusion, this case demonstrates that isolated cerebral FES should always be considered in patients who develop a change in consciousness, even 72 hours after injury. Patients with infected wounds may be at higher risk, and imaging may not initially show definitive abnormalities. Repeated MRI should be considered if the clinical presentation initially does not fully meet Gurd’s criteria.
Supplemental Material
sj-pdf-1-imr-10.1177_03000605211028415 - Supplemental material for Late-onset isolated cerebral fat embolism syndrome after a simple tibial plateau fracture: a rare case report
Supplemental material, sj-pdf-1-imr-10.1177_03000605211028415 for Late-onset isolated cerebral fat embolism syndrome after a simple tibial plateau fracture: a rare case report by Ta-Li Hsu, Tien-Chi Li, Fei-Pi Lai, Ming Ouhyoung, Chih-Hung Chang and Cheng-Tzu Wang in Journal of International Medical Research
Footnotes
Acknowledgements
We greatly thank all the members of the FEMH Orthopaedic Department of Surgery and Department of Radiology for their assistance.
Ethics approval
The requirement for ethics approval was waived because of the nature of this study (case report). Verbal informed consent was obtained from the patient for the publication of this case report and images.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Availability of data and materials
All data associated with the case are presented in the manuscript.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.