
Abstract
Background
Older adults with hypertension have a high incidence of heart failure and poor prognosis, often accompanied with nutritional, inflammatory, and immune dysregulation. The C-reactive protein–albumin–lymphocyte (CALLY) index provides an integrated measure of these conditions. However, its association with the prevalence and prognosis of heart failure in older hypertensive populations remains unclear.
Objective
The core objective of this study was to explore the correlation between the CALLY index and the prevalence of heart failure as well as mortality risk in the older hypertensive population.
Methods
We included data from 5876 hypertensive individuals aged ≥60 years who participated in the National Health and Nutrition Examination Survey from 2003 to 2016. Complex sampling weights were applied for all analyses. The natural logarithmic transformation of the CALLY index (Ln CALLY) was used as the primary exposure variable to reduce skewness and meet model assumptions. The association between Ln CALLY and heart failure prevalence was assessed using a multivariable logistic regression model, while the analysis of mortality was conducted using a Cox proportional hazards model. Further analyses included restricted cubic spline modeling, stratified analyses with interaction tests, and sensitivity analyses.
Results
Participants in the highest quartile of Ln CALLY had a 44% lower likelihood of heart failure compared with those in the lowest quartile (odds ratio = 0.56, 95% confidence interval: 0.40–0.78). Among individuals with heart failure, those in the highest quartile of Ln CALLY exhibited 54% lower all-cause mortality (hazard ratio = 0.46, 95% confidence interval: 0.31–0.68) and 64% lower cardiovascular mortality (hazard ratio = 0.36, 95% confidence interval: 0.19–0.71) than those in the lowest quartile. Restricted cubic spline modeling demonstrated a linear inverse association between Ln CALLY and heart failure prevalence, all-cause mortality, and cardiovascular mortality (all p for nonlinearity >0.05). The results of the subgroup analysis were consistent with the overall conclusions, and no significant interaction effects were observed (all p-interaction >0.05).
Conclusion
Ln CALLY was significantly and inversely associated with both heart failure prevalence and mortality among older adults with hypertension. As a readily obtainable composite index derived from routine laboratory tests, Ln CALLY may serve as a practical tool for precision management in this high-risk population.
Keywords
Introduction
Heart failure (HF) is one of the primary causes of hospitalization and mortality among older adults with hypertension, and its poor prognosis imposes a substantial public health burden.1,2 In this population, up to 68% of HF cases can be attributed to inadequate blood pressure control, and once HF develops, the 5-year mortality rate often exceeds 50%.3–5 With the continuing rise in both population aging and hypertension prevalence, the burden of HF among older hypertensive individuals is expected to increase further. 6 Older adults with hypertension frequently present with chronic inflammation, malnutrition, and immune dysfunction. This imbalance in nutritional, inflammatory, and immune status not only accelerates disease progression but may also increase the risk of incident HF.7,8 Therefore, identifying biomarkers that can fully reflect such conditions is crucial for the prevention and early management of HF.
The C-reactive protein–albumin–lymphocyte (CALLY) index is a novel composite indicator that simultaneously reflects systemic inflammation, nutritional status, and immune function. Emerging evidence suggests its relevance across a variety of cardiovascular conditions. A cross-sectional study involving 8146 individuals with hypertension reported a significant inverse association between the CALLY index and stroke prevalence, with RCS analysis indicating a linear inverse relationship. 9 Similarly, a study by Xu et al. including 27,978 participants found a significant negative correlation between the CALLY index and cardiorenal syndrome prevalence. 10 These findings suggest that the CALLY index may be closely linked to the risk of multiple chronic cardiovascular-related diseases. Moreover, accumulating evidence highlights the prognostic value of the CALLY index. In a cohort of 320 hospitalized older adults at the Air Force Medical Center, He et al. demonstrated that higher CALLY index values were significantly associated with reduced all-cause mortality, showing strong predictive performance for 1-, 3-, and 5-year survival outcomes. 11 In a similar manner, Han et al. observed that elevated CALLY index levels were independently associated with lower all-cause and cardiovascular mortality among patients with cardiovascular disease (CVD) during a median follow-up of 122 months. 12 Similar associations have been reported in other populations, including patients with chronic obstructive pulmonary disease and those with various types of cancer, where lower CALLY index values were strongly linked to poorer survival outcomes.13–16
Notably, the components of the CALLY index—including serum albumin, C-reactive protein (CRP), and lymphocyte count—are potentially modifiable through interventions targeting nutrition, inflammation, and immune regulation. Nutritional supplementation, anti-inflammatory strategies, and optimization of chronic disease management have been shown to favorably influence these parameters and are individually associated with improved cardiovascular outcomes in previous studies.17–19 Therefore, the CALLY index may serve not only as a risk stratification biomarker but also as a modifiable therapeutic indicator at the population level.
As with many chronic diseases, malnutrition and persistent inflammation are common background conditions in patients with HF and play critical roles in both disease development and prognosis.20,21 The CALLY index provides a quantifiable measure of this combined status. However, no prior study has systematically evaluated the association between the CALLY index and both HF prevalence and mortality risk specifically in older adults with hypertension. To bridge this gap, the present study utilized nationally representative data from the National Health and Nutrition Examination Survey (NHANES) 2003–2016 to, for the first time, investigate the relationship between the CALLY index and HF prevalence as well as mortality among older hypertensive individuals. Based on the available data, these findings may provide a certain degree of new evidence for reference in the risk stratification and precise management of this high-risk population.
Methods
Study population and data source
The reporting of this study conforms to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines for observational studies. 22 The NHANES is an ongoing national research program administered by the US Centers for Disease Control and Prevention (CDC). It aims to collect health and nutrition information from the civilian, noninstitutionalized population of the US through a complex stratified multistage probability sampling method, including household interviews, physical examinations, and laboratory tests. Its research protocol has been approved by the Institutional Review Board (IRB) of the National Center for Health Statistics (NCHS) and complies with the guidelines of the Declaration of Helsinki. All participants provided written informed consent.
This study integrated the NHANES data from seven consecutive biennial cycles between 2003 and 2016, with a total of 71,058 participants included. Based on predefined exclusion criteria, we first excluded 57,827 individuals aged <60 years. Subsequently, 3867 participants without hypertension were excluded. Hypertension was defined as meeting any of the following criteria: an average diastolic blood pressure (DBP) ≥90 mmHg or systolic blood pressure (SBP) ≥140 mmHg, self-reported physician diagnosis, or current use of antihypertensive medication. 23 In addition, 3488 participants were excluded due to missing CALLY index values or incomplete covariate data. In total, 5876 participants were finally included in this study, and the detailed flowchart of the selection process is presented in Figure 1. Among these, 526 participants with HF were identified and included in subsequent survival analyses. A diagnosis of HF was established based on whether respondents had a prior history of physician-diagnosed HF, as documented in the questionnaire. 24 Mortality outcomes were ascertained through linkage of the NHANES data with the National Death Index (NDI). Follow-up began with the NHANES baseline examination as the starting point, with the end-point defined as death or 31 December 2019, whichever occurred first; the causes of death were classified in accordance with the International Classification of Diseases, 10th Revision (ICD-10).
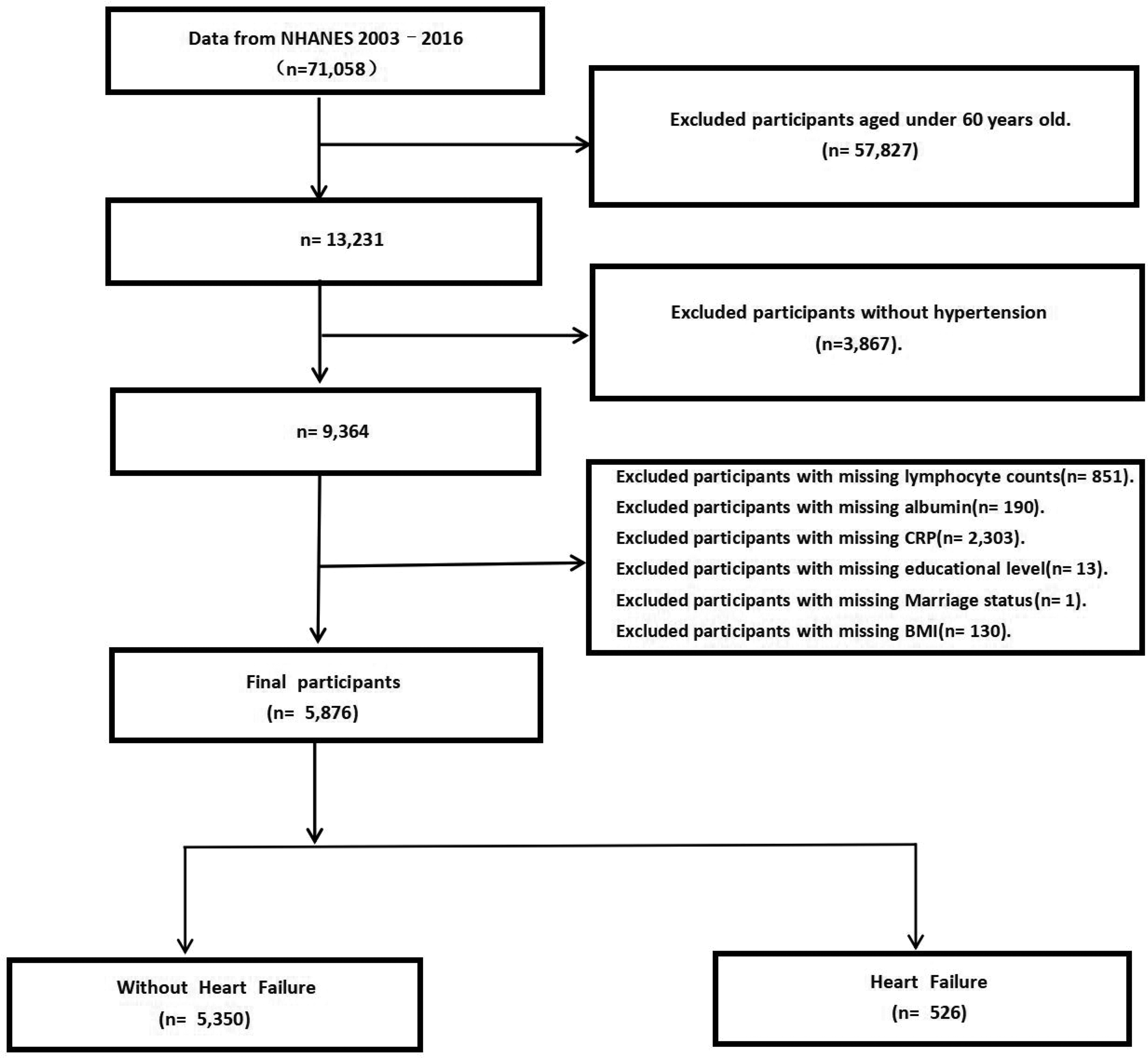
Flowchart of the study participants.
Exposure variables
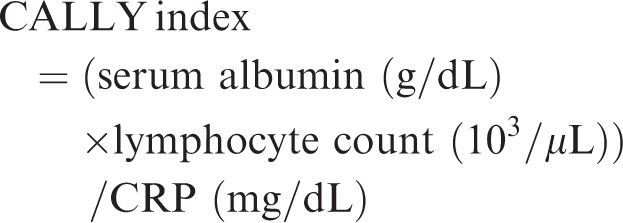
The CALLY index was derived from three routine laboratory parameters available in the NHANES data: CRP (mg/dL) measured using latex-enhanced immunoturbidimetry, serum albumin (g/dL) assessed using the bromocresol green colorimetric method, and lymphocyte count (10³/μL) obtained using an automated five-part differential hematology analyzer. The CALLY index was calculated as follows:
25
Covariates
To control for potential confounders, the models incorporated a range of covariates, including demographic characteristics (age, race, sex, poverty–income ratio (PIR), marital status, and educational level), lifestyle factors (alcohol consumption and smoking status), and comorbid chronic conditions. Diabetes was defined as self-reported physician diagnosis, current use of antidiabetic medication, glycated hemoglobin (HbA1c) ≥6.5%, or fasting plasma glucose ≥126 mg/dL. Chronic kidney disease (CKD) was determined using the CKD–Epidemiology Collaboration (EPI) equation for estimated glomerular filtration rate (eGFR) in combination with the urinary albumin-to-creatinine ratio (UACR) and was defined as UACR ≥30 mg/g or eGFR <60 mL/min/1.73 m2. CVD history included self-reported coronary heart disease, angina, myocardial infarction, or stroke. Because the present study focused on HF prevalence and mortality among older adults with hypertension, HF was not included as a covariate, and CVD referred only to cardiovascular events other than HF. Hypercholesterolemia was defined as total cholesterol ≥240 mg/dL, current use of lipid-lowering therapy, self-reported diagnosis, or low-density lipoprotein cholesterol (LDL-C) ≥160 mg/dL. In addition, body mass index (BMI) was included as an important indicator of metabolic status.
Statistical analyses
To address the marked skewness of the CALLY index, the natural logarithmic transformation of the CALLY index (Ln CALLY) was applied, which improved the model fit, enhanced robustness, and facilitated interpretability of the results. All analyses in this study were performed using R software (version 4.3.3), with the significance threshold for two-tailed tests set at p < 0.05. The NHANES sampling weights were incorporated to account for the complex, multistage survey design and ensure nationally representative estimates. Following the NHANES guidelines, adjustments were made for sampling weights (WTMEC2YR), strata (SDMVSTRA), and clusters (SDMVPSU), with each 2-year cycle weight divided by 7 (the total number of cycles) before being combined. Multicollinearity among covariates was evaluated using the variance inflation factor (VIF), and variables with VIF >10 were excluded. Descriptive statistics were presented as frequencies and percentages for categorical variables and as mean ± SD values for continuous variables. Intergroup differences were assessed using weighted chi-square tests and survey-weighted linear regression.
For inferential analyses, multivariable Cox proportional hazards regression models were employed to estimate hazard ratios (HRs) and 95% confidence intervals (CIs) for evaluating the associations of the CALLY index with all-cause and cardiovascular mortality. Model 1 was unadjusted; Model 2 was adjusted for age, sex, and race; and Model 3 was further adjusted for BMI, PIR, marital status, educational level, smoking status, alcohol consumption, diabetes, CVD, hypercholesterolemia, and CKD. To examine dose–response relationships, Ln CALLY was analyzed both as a continuous variable and by quartiles (Q1–Q4). RCS models were used to evaluate potential linear and nonlinear associations of Ln CALLY with HF prevalence and mortality among HF patients, adjusting for covariates as specified in Model 3. Sensitivity analyses were performed using alternative definitions of hypertension to assess the robustness of the results. Finally, we performed subgroup analyses stratified by variables such as age, BMI, diabetes, and CKD status and tested interaction terms to further validate the prognostic effect of the CALLY index across different populations.
Results
Baseline characteristics
In total, 5876 hypertensive participants aged ≥60 years were included in the final analysis, comprising 57.3% women and 42.7% men, with a mean age of 70.78 ± 7.14 years. Among them, 526 individuals (8.95%) were diagnosed with HF. Baseline characteristics are summarized in Table 1. When stratified by HF status, participants with HF had lower serum albumin levels and lymphocyte count but showed higher CRP levels than those without HF. In addition, patients in the HF group were older; this group had a higher proportion of men, higher BMI, and lower educational level. In terms of lifestyle factors, the proportion of smokers was higher in the HF group. Regarding comorbidities, the prevalence of diabetes, CVD, hypercholesterolemia, and CKD was significantly higher among participants with HF.
Baseline characteristics of older hypertensive participants stratified by heart failure status.
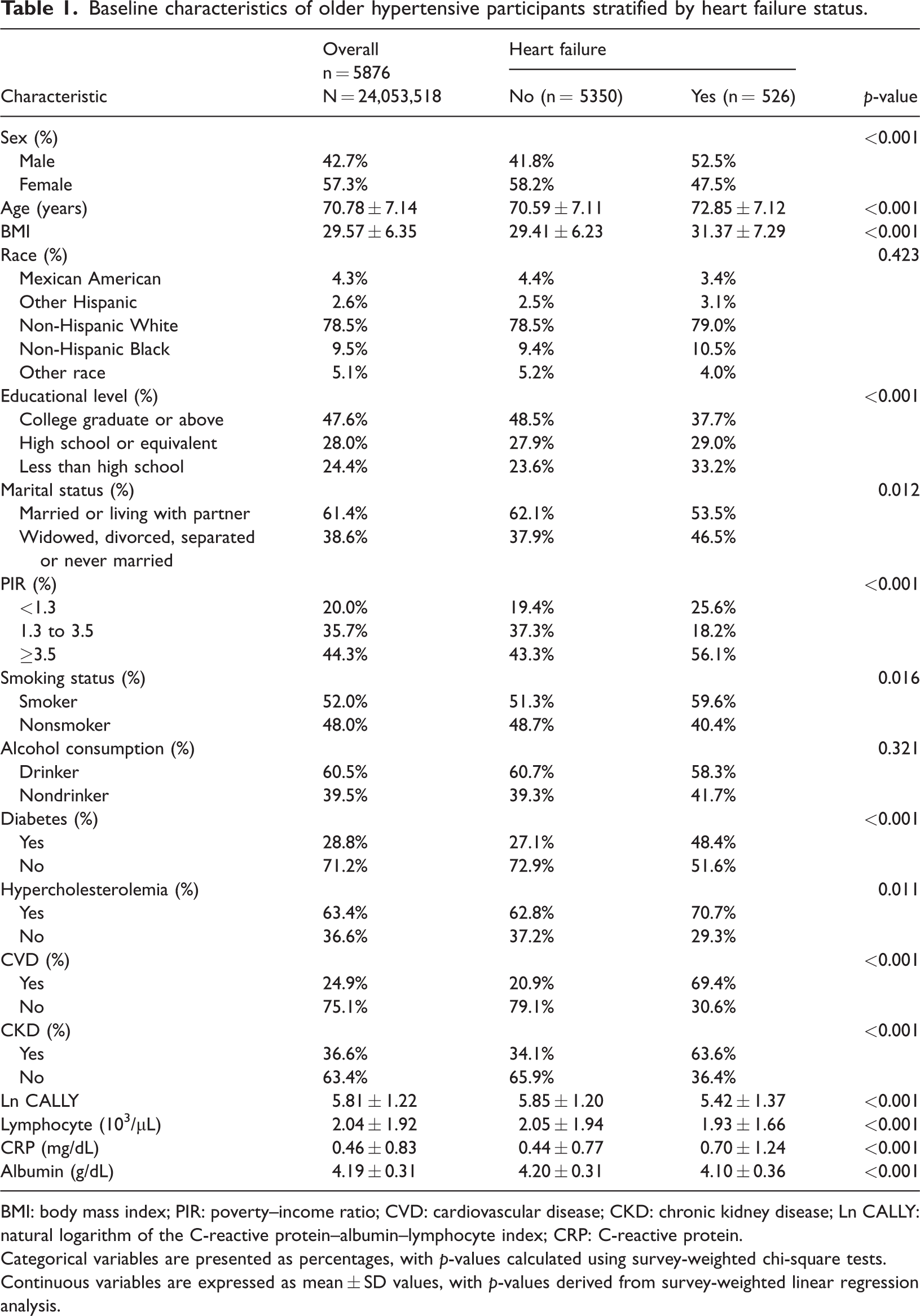
BMI: body mass index; PIR: poverty–income ratio; CVD: cardiovascular disease; CKD: chronic kidney disease; Ln CALLY: natural logarithm of the C-reactive protein–albumin–lymphocyte index; CRP: C-reactive protein.
Categorical variables are presented as percentages, with p-values calculated using survey-weighted chi-square tests. Continuous variables are expressed as mean ± SD values, with p-values derived from survey-weighted linear regression analysis.
Association between Ln CALLY and HF
As shown in Table 2, among older adults with hypertension, higher Ln CALLY was associated with a lower prevalence of HF. When modeled as a continuous variable, each one-unit increase in Ln CALLY corresponded to a 29% lower prevalence of HF in the unadjusted model (odds ratio (OR) = 0.71, 95% CI: 0.65–0.78), and the association persisted after full adjustment (OR = 0.83, 95% CI: 0.74–0.92). In quartile analyses, compared with the lowest quartile (Q1), participants in the highest quartile (Q4) had a 44% lower prevalence of HF (OR = 0.56, 95% CI: 0.40–0.78), and a gradual decreasing trend was observed (p for trend <0.001).
Odds ratios (95% confidence intervals) for the prevalence of heart failure according to the quartiles of Ln CALLY in the older hypertensive population from the NHANES 2003–2016.

Model 1: Unadjusted for covariates.
Model 2: Adjusted for age, sex, and race.
Model 3: Further adjusted for sex, age, race, body mass index (BMI), educational level, marital status, poverty–income ratio (PIR), smoking status, alcohol consumption, hypercholesterolemia, cardiovascular disease, chronic kidney disease, and diabetes.
OR: odds ratio; CI: confidence interval; Ln CALLY: natural logarithm of the C-reactive protein–albumin–lymphocyte index; Q: quartile.
Table 3 presents the Cox regression results. Among participants with previously diagnosed HF, higher Ln CALLY was associated with a lower mortality risk. In the fully adjusted models, when treated as a continuous variable, each one-unit increase in Ln CALLY was associated with an approximately 19% lower risk of all-cause mortality (HR = 0.81, 95% CI: 0.73–0.89) and a 25% lower risk of cardiovascular mortality (HR = 0.75, 95% CI: 0.62–0.91). In quartile comparisons, relative to Q1, participants in Q4 had a 54% lower risk of all-cause mortality (HR = 0.46, 95% CI: 0.31–0.68); a similar pattern was observed for cardiovascular mortality, with a 64% lower risk in Q4 (HR = 0.36, 95% CI: 0.19–0.71).
Hazard ratios (95% confidence intervals) for mortality in older patients with hypertension complicated with heart failure from the NHANES 2003–2016 according to the quartiles of Ln CALLY.

Model 1: Unadjusted for covariates.
Model 2: Adjusted for age, sex, and race.
Model 3: Further adjusted for sex, age, race, body mass index (BMI), educational level, marital status, poverty–income ratio (PIR), smoking status, alcohol consumption, hypercholesterolemia, cardiovascular disease, chronic kidney disease, and diabetes.
HR: hazard ratio; CI: confidence interval; Ln CALLY: natural logarithm of the C-reactive protein–albumin–lymphocyte index; Q: quartile.
RCS analyses were further conducted to explore the associations of Ln CALLY with HF and mortality. As shown in Figure 2(a), Ln CALLY was linearly and inversely associated with HF prevalence (p for nonlinearity = 0.524). Similarly, as shown in Figure 2(b) and (c), Ln CALLY showed linear inverse associations with all-cause mortality (p for nonlinearity = 0.515) and cardiovascular mortality (p for nonlinearity =0.611), respectively. Overall, no significant nonlinear trends were observed in any of the three analyses (p for nonlinearity >0.05).

(a) RCS plot of the relationship between Ln CALLY and heart failure prevalence in older hypertensive participants. (b) RCS plot of the relationship between Ln CALLY and all-cause mortality in patients with heart failure and (c) RCS plot of the relationship between Ln CALLY and cardiovascular mortality in patients with heart failure. RCS: restricted cubic spline; Ln CALLY: natural logarithm of the C-reactive protein–albumin–lymphocyte index.
Subgroup analyses
To assess the stability of the associations between Ln CALLY and HF prevalence and mortality across different subgroups of older hypertensive individuals, subgroup analyses were performed along with interaction tests. No significant differences were observed across subgroups, as all interaction p-values exceeded 0.05. These findings further support the robustness and consistency of our results (Figures 3 to 5).

Relationship between Ln CALLY and heart failure prevalence in each subgroup: point estimates represent ORs, and line segments represent 95% CIs. There was no significant interaction among all subgroups (all p for interaction > 0.05). Ln CALLY: natural logarithm of the C-reactive protein–albumin–lymphocyte index; ORs: odds ratios; CIs: confidence intervals.

Relationship between Ln CALLY and risk of all-cause mortality in each subgroup: point estimates represent HRs, and line segments represent 95% CIs. There was no significant interaction among all subgroups (all p for interaction > 0.05). Ln CALLY: natural logarithm of the C-reactive protein–albumin–lymphocyte index; HRs: hazard ratios; CIs: confidence intervals.

Relationship between Ln CALLY and risk of cardiovascular mortality in each subgroup: point estimates represent HRs, and line segments represent 95% CIs. There was no significant interaction among all subgroups (all p for interaction > 0.05). Ln CALLY: natural logarithm of the C-reactive protein–albumin–lymphocyte index; HRs: hazard ratios; CIs: confidence intervals.
Sensitivity analyses
In the primary analyses, hypertension was defined using the traditional criteria (mean DBP ≥90 mmHg or SBP ≥140 mmHg), which were widely applied during the NHANES 2003–2016 cycles and were consistent with previous studies. To verify the robustness of our findings, we further conducted sensitivity analyses. When the study population was redefined according to the 2017 ACC/AHA guideline criteria (DBP ≥80 mmHg or SBP ≥130 mmHg), 26 the direction and significance of the associations between Ln CALLY and HF prevalence, all-cause mortality, and cardiovascular mortality remained consistent with the main analyses (Supplementary Tables S1 and S2); thus, these results provide strong support for the stability and generalizability of our study findings.
Discussion
Using nationally representative data from the NHANES 2003–2016, this is the first study to systematically evaluate the associations of the CALLY index with HF prevalence and mortality in older adults with hypertension. We found that, after adjusting for demographic factors, lifestyle behaviors, and comorbidities, Ln CALLY was significantly and linearly inversely associated with HF. Compared with participants in the lowest quartile, those in the highest quartile had a 44% lower likelihood of HF (OR = 0.56, 95% CI: 0.40–0.78). Among older hypertensive individuals with a prior medical diagnosis of HF, higher Ln CALLY levels were also associated with markedly reduced risks of all-cause and cardiovascular mortality. RCS analyses further supported these linear associations (p for nonlinearity >0.05). Notably, the spline curves suggested a tendency for risk reduction to plateau at higher Ln CALLY levels. Although the primary statistical conclusion indicates a linear relationship, this flattening pattern should be regarded as a visual indication rather than evidence of a threshold effect, possibly reflecting diminishing incremental benefits once nutritional, inflammatory, and immune status have reached relatively optimal levels. These major findings were consistently confirmed in both subgroup and sensitivity analyses, further strengthening the robustness of our conclusions.
Our findings are consistent with those of previous studies demonstrating strong associations between nutritional and inflammatory markers and HF. A study including 48,155 adults reported that the systemic immune-inflammation index (SII) was significantly associated with HF prevalence (OR = 1.32, 95% CI: 1.06–1.65) in a nonlinear manner. 27 Similarly, a study by Zhang et al. using NHANES data found that elevated neutrophil-to-lymphocyte ratio (NLR) and systemic inflammation response index (SIRI) were both significantly associated with increased HF prevalence. 28 In addition to HF prevalence, inflammatory–nutritional indices serve as important prognostic predictors in patients with HF. A recent meta-analysis including 12,537 HF patients with established malnutrition revealed that malnutrition was associated with a more than two-fold higher risk of all-cause mortality (HR = 2.15, 95% CI: 1.89–2.45). 29 In another study involving 718 HF patients, a higher lymphocyte-to-CRP ratio (LCR) was identified as an independent prognostic factor for both cardiovascular and all-cause mortality, with significantly poorer outcomes in the low-LCR group. 30 Furthermore, Wu et al. demonstrated that both neutrophil-to-albumin ratio (NPAR) and NLR were independently associated with all-cause mortality in HF patients. Over a median follow-up of 66 months, participants in the highest quartiles of NPAR (HR = 1.81, 95% CI: 1.35–2.43) and NLR (HR = 1.59, 95% CI: 1.18–2.15) had substantially increased mortality risks compared with those in the lowest quartiles. 31 Collectively, these studies are in line with our findings on the CALLY index, underscoring the combined impact of inflammation and nutritional status on the development and prognosis of HF and providing compelling rationale for screening and intervention strategies based on multidimensional biomarkers.
Older patients with hypertension are chronically exposed to sustained pressure overload, which induces myocardial hypertrophy and fibrosis, thereby increasing ventricular stiffness and the risk of HF.32,33 Importantly, hypertension-driven cardiovascular remodeling does not occur in isolation but is closely linked to systemic inflammation, metabolic disturbances, and immune dysfunction, together forming the complex pathological background of HF.8,34 Within this context, the CALLY index—which integrates the nutritional status, systemic inflammation, and immune function—may influence HF progression through multiple interrelated mechanisms. Its strength lies in combining three routine laboratory markers—serum albumin, lymphocyte count, and CRP—to capture HF pathophysiology from a multidimensional perspective. Serum albumin is a key protein maintaining homeostasis and nutritional status, playing critical roles in muscle metabolism, redox balance, and inflammation regulation.35,36 Hypoalbuminemia, a hallmark of the malnutrition–inflammation complex syndrome (MICS), directly contributes to skeletal muscle wasting and impaired myocardial function in HF. 37 Elevated CRP reflects systemic inflammation and is mechanistically linked to endothelial dysfunction, vascular stiffness, myocardial fibrosis, and impaired contractility via upregulation of proinflammatory cytokines such as tumor necrosis factor-alpha (TNF-α) and interleukin (IL)-6.38–40 Lymphocyte count indicates immune competence; lymphopenia in chronic HF reflects immune senescence and impaired tissue repair, predisposing patients to infections and worsening outcomes.41,42 Taken together, the CALLY index simultaneously captures the nutritional reserve, inflammatory burden, and immune response, demonstrating its potential as an efficient and comprehensive biomarker for risk stratification and prognosis in older hypertensive patients with HF. In addition to identifying high-risk individuals, it provides a rationale for multidimensional interventions targeting nutrition deficiency, inflammation, and immune modulation. Future studies should focus on clarifying the mechanisms underlying the relationship between the CALLY index and HF-related pathology, conducting longitudinal validation, and facilitating the transformation of this index from an observational marker to a clinically usable tool.
Several notable strengths are evident in this study. First, the data were derived from the nationally representative NHANES cohort in the United States, providing strong generalizability and external validity. Second, we rigorously adjusted for a wide range of covariates and potential confounders, thereby enhancing the robustness of the findings. In addition, subgroup and sensitivity analyses consistently supported the stability of the primary results.
Nevertheless, several limitations should be acknowledged. Although multiple covariates were included, residual confounding cannot be fully excluded, such as medication history and detailed dietary information, which were not available and may influence the accuracy of the associations. In addition, information on HF severity was not available in the NHANES, which may have further contributed to residual confounding. Moreover, due to the lack of echocardiographic data, we were unable to assess cardiac function staging or more refined HF phenotypes. In the NHANES, HF was identified based on self-reported physician diagnosis rather than objective imaging or adjudicated clinical records. Therefore, a certain degree of misclassification cannot be completely ruled out, and differentiation between HF with preserved ejection fraction (HFpEF) and HF with reduced ejection fraction (HFrEF) was not possible. In addition, HF may have been underdiagnosed among older adults, which could lead to an underestimation of its prevalence. However, such misclassification is likely to be nondifferential with respect to the CALLY index and could bias the observed associations toward the null. Furthermore, this study relied on a single blood measurement, whereas nutritional and inflammatory states are dynamic in nature; thus, a one-time assessment may not fully capture long-term individual status and could attenuate the true strength of the associations. Finally, it must be noted that the core coverage of the NHANES sample is restricted to the US adult population. Owing to this sampling characteristic, the generalizability of our study findings to other ethnic groups and populations remains unclear, and further in-depth research is urgently needed to explore this aspect.
Conclusion
Analysis based on the NHANES data showed a significant negative correlation between the CALLY index and the prevalence of HF as well as mortality in older hypertensive patients, which can provide a reference for potential biomarkers in HF risk assessment for this population. To translate the CALLY index into a clinically usable diagnostic and prognostic tool, further validation of its applicable scope is required in older hypertensive populations of different regions and ethnicities through multicenter prospective cohort studies. In conclusion, this study lays a foundation for the application of the CALLY index in HF management among older hypertensive patients, and more high-quality studies are needed in the future to promote its translation into clinical practice.
Footnotes
Acknowledgments
We would like to acknowledge the participants and investigators of the National Health and Nutrition Examination Survey (NHANES).
Author contributions
The study was designed by JW and DX. Data analyses were performed and the initial draft of the manuscript was prepared by YL and YZ. The manuscript was revised by LF. All authors have read and approved the final manuscript.
Clinical trial number
Not applicable.
Consent for publication
Not applicable.
Data availability
Declaration of conflicting interests
The authors declare that they have no competing interests.
Ethics approval and consent to participate
This study was conducted in accordance with the ethical guidelines of the Declaration of Helsinki.
Detailed methods and protocols of the NHANES study were approved by the Center for Disease Control (CDC)/National Center for Health Statistics (NCHS) Research Ethics Review Board. They are publicly available through the CDC website (cdc.gov); this includes informed consent procedures for all participants. All procedures in this study were performed in accordance with the relevant guidelines and regulations. This study was exempt from human participant ethical review as the data are freely available in the public domain.
Funding
This study received no external funding.
Supplemental material
Supplemental material for this article is available online.