
Abstract
Objective
Gallstones, influenced by obesity, hypertension, and diabetes, are a common digestive disorder. The ability of the hepatic steatosis index to predict gallstone risk remains underexplored.
Methods
This study investigated the link between the hepatic steatosis index and the risk of gallstones using the 2017–2020 National Health and Nutrition Examination Survey data. In total, 7244 participants, including 759 with gallstones, were analyzed. Generalized linear models were used to assess the correlation between the hepatic steatosis index and gallstone risk, after adjusting for demographic and lifestyle factors.
Results
A significant positive association was observed between the hepatic steatosis index and gallstone risk, with odds ratios ranging from 1.05 to 1.06 for each unit increase in the hepatic steatosis index. Higher hepatic steatosis index quartiles indicated increased risk, particularly in women and those aged <60 years. Restricted cubic splines analysis suggested a nonlinear relationship, with threshold analysis revealing specific inflection points.
Conclusion
The hepatic steatosis index is a significant predictor of gallstone risk, especially in women and younger populations. These findings highlight the role of the hepatic steatosis index in predicting gallstone risk. Further research into the pathophysiology of gallstone formation is needed for establishing better prevention and treatment strategies.
Keywords
Introduction
Gallstones are a common digestive system disorder, affecting approximately 10%–20% of adults globally.1,2 The incidence of gallstones is higher in western countries and is closely associated with lifestyle factors such as high-fat diets, obesity, and physical inactivity.3–5 Women are more prone to developing gallstones than men, with hormonal factors such as pregnancy, multiple pregnancies, and oral contraceptive use increasing the risk.6,7 Age is another significant factor, with the incidence of gallstones being higher in individuals aged >50 years.8,9 Gallstones can be classified into cholesterol and pigment stones, the latter being more common in Asia.10,11 With advancements in imaging technology, a higher number of asymptomatic cases are being detected, which were previously undiagnosed and not included in older prevalence estimates. This improved detection suggests that previous estimates of prevalence were too low. Epidemiological data indicate that the incidence of gallstones is strongly correlated with lifestyle, dietary habits, and population aging,12,13 emphasizing the need for further research into the underlying mechanisms of gallstone formation.
The hepatic steatosis index (HSI) is a simple and effective noninvasive tool introduced by Lee et al. in 2010, designed to assess the degree of fatty liver in patients with nonalcoholic fatty liver disease (NAFLD). 14 The HSI combines blood biochemical markers (such as the ratio of alanine aminotransferase (ALT) to aspartate aminotransferase (AST)), body mass index (BMI), and diabetic status to create a risk assessment tool for clinical screening. Compared with traditional NAFLD diagnostic methods, the HSI offers higher accuracy and is cost-effective, making it widely applicable in clinical practice. Studies have shown that the HSI not only effectively assesses the risk of NAFLD but is also closely related to metabolic syndrome, diabetes, and other conditions.15–17 As a significant biomarker, the HSI has increasingly become an important tool for evaluating liver fat content and related metabolic diseases.
This study aimed to explore the relationship between the HSI and gallstones. Although previous studies have indicated a close association between the HSI and NAFLD occurrence, the relationship between the HSI and gallstone risk has not been thoroughly investigated. Based on the 2017–2020 data from the National Health and Nutrition Examination Survey (NHANES), this study analyzed whether the HSI is a potential predictor of gallstone risk. The theoretical significance of this research lies in filling the gap in existing HSI studies related to gallstones, evaluating the potential of HSI to enhance our understanding of the pathophysiological mechanisms of gallstone formation, and providing new theoretical support and clinical guidance for the prevention and management of gallstones. The ultimate goal of the study was to assess the application value of the HSI in gallstone risk evaluation, offering a simple and effective tool for clinical practice and promoting improved prevention and management strategies for gallstone-related diseases.
Materials and methods
Study design
This study adopted a cross-sectional design to explore the factors associated with the occurrence of gallstones. Data were sourced from the NHANES database, covering the period from 2017 to 2020. The NHANES, conducted by the Centers for Disease Control and Prevention (CDC), is a large-scale epidemiological survey that assesses the health status, nutritional conditions, and disease burden of the US population. 18 The database offers extensive health examination data, laboratory test results, and detailed lifestyle and socioeconomic information, making it a crucial resource for public health research. The data for this study were obtained from the NHANES public database on 20 April 2025. This retrospective study utilized de-identified, publicly available data, which did not contain any personally identifiable information. The reporting of this study conforms to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines for cross-sectional studies. 19
The study participants were adults who participated in the NHANES from 2017 to 2020, specifically individuals aged ≥20 years with complete data on HSI, gallstone status, and relevant covariates. As per the exclusion criteria, participants aged <20 years and those with missing data on gallstone status, HSI, or covariates were excluded. The selection process is depicted in Figure 1. In total, 7244 eligible participants were included in the analysis, of which 759 were diagnosed with gallstones.

Flowchart of participant selection.
The NHANES study protocol received approval from the Research Ethics Review Board of the National Center for Health Statistics (NCHS), and all participants provided written informed consent. Therefore, no further ethical approval or participant consent was necessary for subsequent data analyses. This study was conducted in accordance with the Declaration of Helsinki (1975, as revised in 2024).
Study variables
Dependent variable
The presence of gallstones was considered the primary outcome variable in this study. Gallstone status was determined based on the survey question “Has a doctor ever told you that you have gallstones?” The responses were then categorized accordingly.
Independent variable: HSI
The HSI formula proposed by Lee et al. in 2010 was used in this study. 14 It has been validated for NAFLD screening. The HSI formula is as follows: HSI = 8 × (ALT/AST ratio) + BMI (kg/m2) + 2 points for females and +2 points for the presence of diabetes.
In this study, we calculated the HSI using data from the NHANES database. ALT and AST levels were assessed according to stringent laboratory standards. Blood samples were collected in the morning after a minimum 8-h fasting period to ensure the accuracy of the results. These standardized laboratory methods ensured the accuracy and reliability of the data, providing a solid foundation for HSI calculation.
Covariates
Based on previous research, this study included several potential confounding factors as covariates in the statistical model to control for their impact on the study outcomes.20,21 In addition to the variables required for HSI calculation, the following covariates were included in the analysis: age, race, educational level, marital status, hypertension, smoking status, alcohol consumption, physical activity, triglycerides, total cholesterol, high-density lipoprotein cholesterol (HDLc), and γ-glutamyl transferase (GGT). Participants were categorized into the following two age groups: <60 years and ≥60 years. Race and ethnicity were categorized as follows: Mexican American, other Hispanic, non-Hispanic White, non-Hispanic Black, and other races (including multiracial). Educational level was classified into the following three groups: lower educational level (<9th grade and 9th–11th grade, including 12th grade without a diploma); medium educational level (high school graduate/general educational development (GED) or equivalent or some college or associate degree); and higher educational level (college graduate or above). Marital status was divided into the following three categories: cohabitation (married or living with a partner), unmarried, and living alone (widowed/divorced/separated). Triglycerides, total cholesterol, and HDLc were included as continuous variables in the analysis as lipid indicators. GGT, a biomarker of liver function, was also analyzed as a continuous variable. Smoking status was classified based on the question “Have you smoked more than 100 cigarettes?”, with “yes” indicating smokers and “no” indicating nonsmokers. Alcohol consumption was classified based on the “alcohol consumption frequency in the past 12 months” into the following three groups: nondrinker (never or never in the past year), occasional drinker (once a month, 2–3 times a month, once a week, or twice a week), and regular drinker (3–4 times a week, almost daily, or daily). Participants were categorized as physically active if they engaged in moderate physical activity, defined as activities that cause small increases in breathing or heart rate, such as brisk walking or carrying light loads, for at least 10 min continuously.
Statistical methods
Continuous variables were presented as mean ± SD, while categorical variables were reported as frequencies or percentages. To explore the relationship between the HSI and the risk of gallstones, this study employed three multivariable generalized linear models as follows: (a) model 1 was not adjusted for any covariates; (b) model 2 was adjusted for age, race, educational level, and marital status; and (c) model 3 was further adjusted for hypertension, triglycerides, total cholesterol, HDLc, GGT, smoking status, alcohol consumption, and physical activity. To explore the potential nonlinear relationship between the HSI and gallstone risk, we employed restricted cubic splines (RCS) with 5 knots placed at the 5th, 27.5th, 50th, 72.5th, and 95th percentiles of the HSI distribution. After establishing a nonlinear association, we employed a recursive algorithm to identify the inflection points, which were used to construct a piecewise linear regression model to examine the changes in the relationship between the HSI and gallstone risk before and after the inflection points. Additionally, subgroup analyses were conducted to explore the differential predictive effect of the HSI across various groups. All statistical analyses were performed using R version 4.3.2 (R Foundation for Statistical Computing, Vienna, Austria; https://www.R-project.org), with a p value <0.05 indicating statistical significance.
Results
Baseline characteristics
In total, 7244 participants were included in this study, of which 6485 had no gallstones (89.5%) and 759 had gallstones (10.5%). Patients with gallstones were significantly older (57.9 ± 15.7 vs. 50.0 ± 17.4 years, p < 0.001), and the majority of them were women (71.5% vs. 48.7%, p < 0.001). Hypertension, diabetes, and smoking habit were more common among patients with gallstones than among those without gallstones (53.9% vs. 36.6%, p < 0.001; 28.7% vs. 17.0%, p < 0.001, and 46.8% vs. 41.7%, p = 0.008, respectively). The comparison of other baseline characteristics, including ethnicity, educational level, marital status, and alcohol consumption, is presented in Table 1.
Baseline data summary for NHANES study participants (N = 7244).
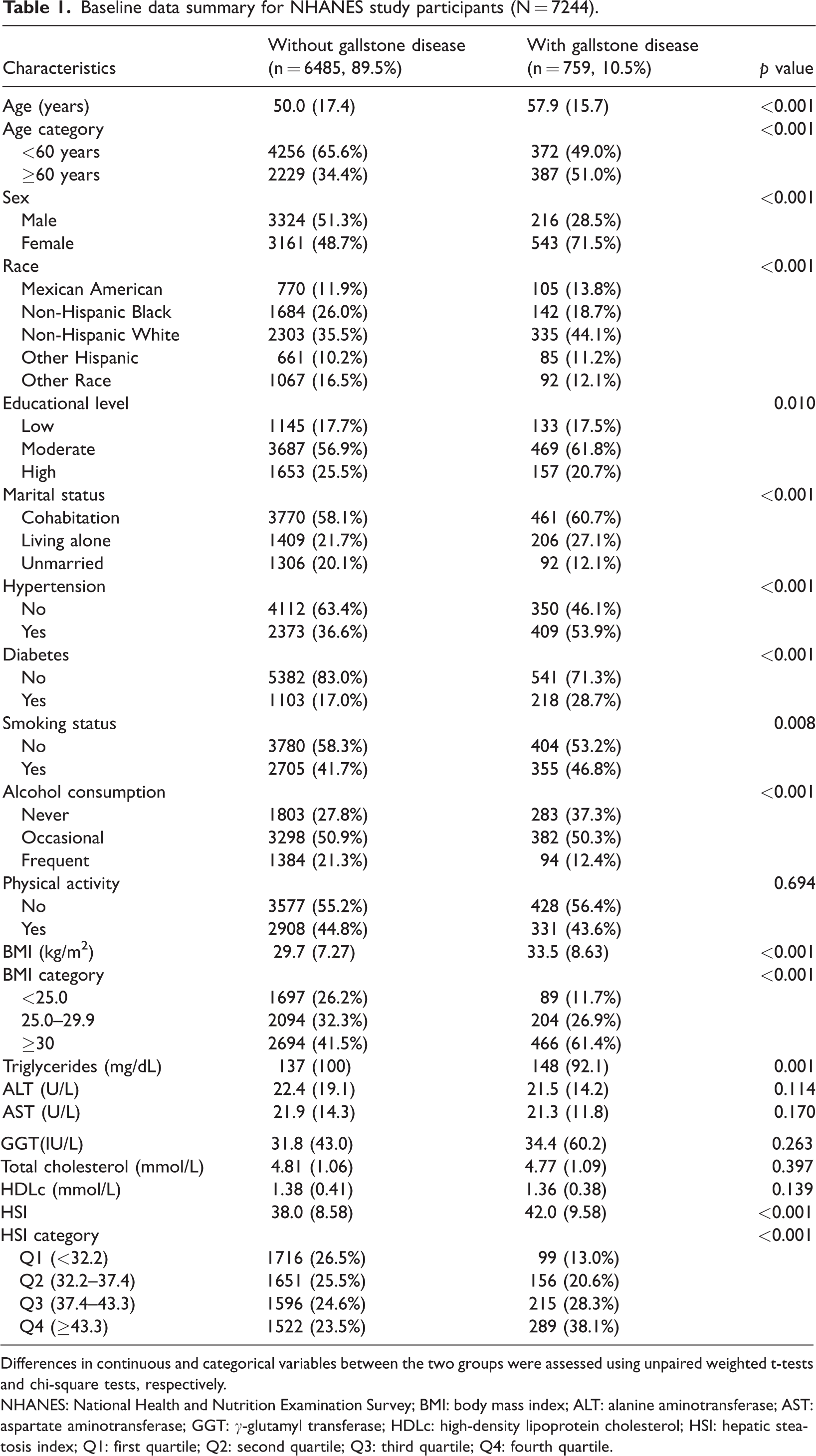
Differences in continuous and categorical variables between the two groups were assessed using unpaired weighted t-tests and chi-square tests, respectively.
NHANES: National Health and Nutrition Examination Survey; BMI: body mass index; ALT: alanine aminotransferase; AST: aspartate aminotransferase; GGT: γ-glutamyl transferase; HDLc: high-density lipoprotein cholesterol; HSI: hepatic steatosis index; Q1: first quartile; Q2: second quartile; Q3: third quartile; Q4: fourth quartile.
Regarding BMI, patients with gallstones had a significantly higher BMI than those without (33.5 ± 8.63 vs. 29.7 ± 7.27 kg/m2, p < 0.001). Further analysis of BMI distribution showed that the proportion of patients with BMI ≥30 kg/m2 was significantly higher in the gallstone group (61.4% vs. 41.5%, p < 0.001). In terms of lipid profile, triglyceride levels were significantly higher in the gallstone group (148 vs. 137 mg/dL, p = 0.001), while there were no significant differences in the total cholesterol, HDLc, ALT, AST, and GGT (p > 0.05) levels between the two groups. Finally, the HSI was significantly higher in the gallstone group (42.0 ± 9.58 vs. 38.0 ± 8.58, p < 0.001). Further analysis of HSI quartile data revealed that the proportion of patients with HSI ≥43.3 (fourth quartile (Q4)) was significantly higher in the gallstone group (38.1% vs. 23.5%, p < 0.001). These results suggest a significant association between the HSI and gallstone risk.
HSI and gallstones
This study utilized three generalized linear models to evaluate the relationship between the HSI and gallstone risk. The results indicated a positive correlation between the HSI and gallstone risk. Specifically, for every 1-unit increase in the HSI, the gallstone risk significantly increased, with odds ratios (ORs) of 1.05, 1.05, and 1.06 (p < 0.001) for the three models, indicating that the HSI is an independent risk factor for gallstone risk. Further analysis explored the relationship between the HSI quartiles and gallstone risk. Compared with the first quartile (Q1; reference group), the OR for the second quartile (Q2) was 1.40 (95% confidence interval (CI): 0.88–2.22; p = 0.146), that for the third quartile (Q3) was 1.83 (95% CI: 1.15–2.90; p = 0.012), and that for Q4 was 2.66 (95% CI: 1.87–3.77; p < 0.001), showing a significant upward trend in model 1. The results from models 2 and 3 further confirmed this association, with Q4 ORs of 2.80 (95% CI: 1.88–4.16; p < 0.001) and 3.01 (95% CI: 1.58–5.71; p = 0.009), respectively. Additionally, trend test showed a significant trend between HSI quartiles and gallstone risk, with a p for trend value of <0.001 (Table 2).
Generalized linear model analysis between HSI and gallstone risk.
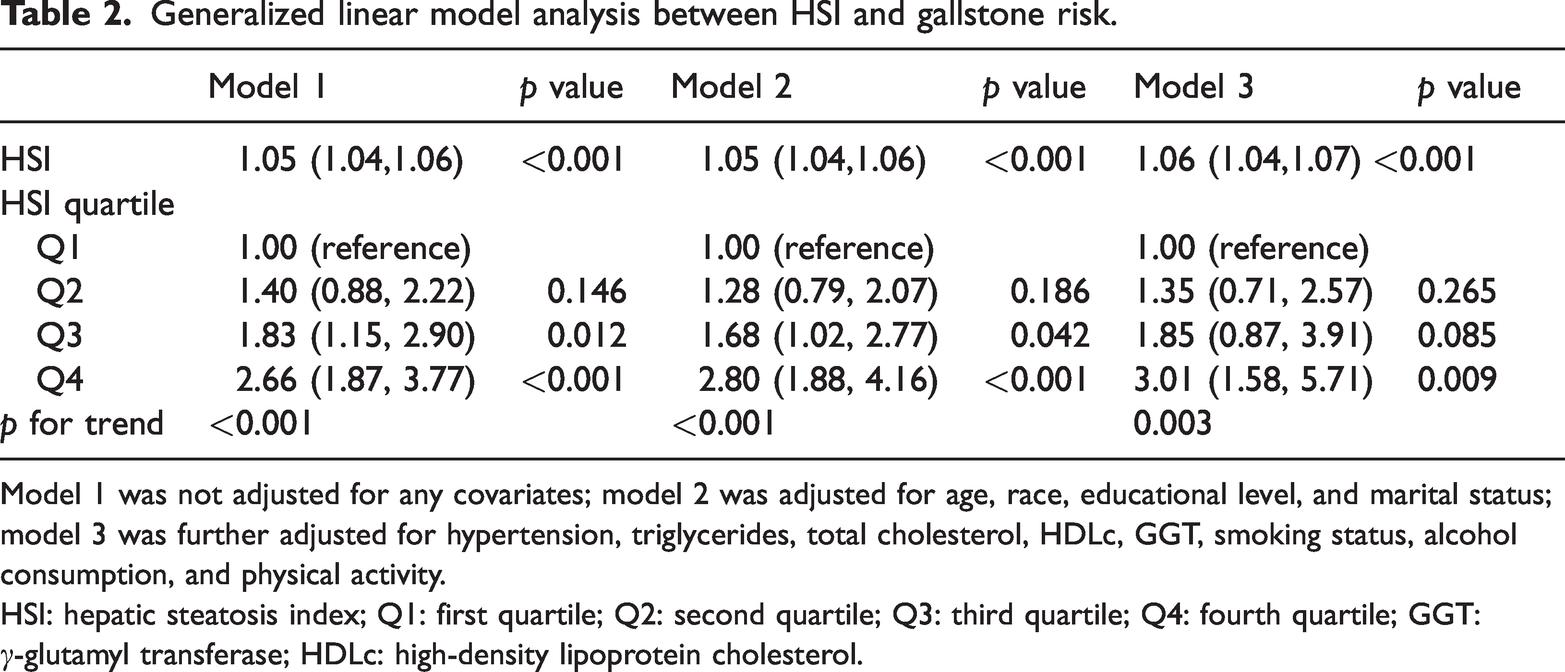
Model 1 was not adjusted for any covariates; model 2 was adjusted for age, race, educational level, and marital status; model 3 was further adjusted for hypertension, triglycerides, total cholesterol, HDLc, GGT, smoking status, alcohol consumption, and physical activity.
HSI: hepatic steatosis index; Q1: first quartile; Q2: second quartile; Q3: third quartile; Q4: fourth quartile; GGT: γ-glutamyl transferase; HDLc: high-density lipoprotein cholesterol.
Further exploration of the nonlinear relationship between the HSI and gallstone risk was conducted using RCS analysis. The results showed that the overall model had a p value of <0.001, indicating a significant relationship between the HSI and gallstone risk, and the p value for nonlinear analysis was 0.023, suggesting a nonlinear relationship (Figure 2). Overall, the results of this study support HSI as a potential predictor of gallstone risk and reveal differences in gallstone risk at various HSI values.

Association between the HSI and gallstone risk using restricted cubic spline analysis.
Threshold analysis
This study further conducted a threshold analysis to examine the relationship between the HSI and gallstone risk, with a focus on its effects across different populations, sex, and age groups. The overall threshold analysis revealed that the inflection point for HSI was 37.54 (Table 3). Below this threshold, each 1-unit increase in the HSI significantly raised the risk of gallstones (OR = 1.08, 95% CI: 1.04–1.13; p < 0.001). However, when the HSI was ≥37.54, the increase in risk per 1-unit rise in the HSI was significantly smaller (OR = 1.04, 95% CI: 1.03–1.06; p < 0.001).
Threshold effect of HSI on gallstone: analysis using a two-piecewise linear regression model.
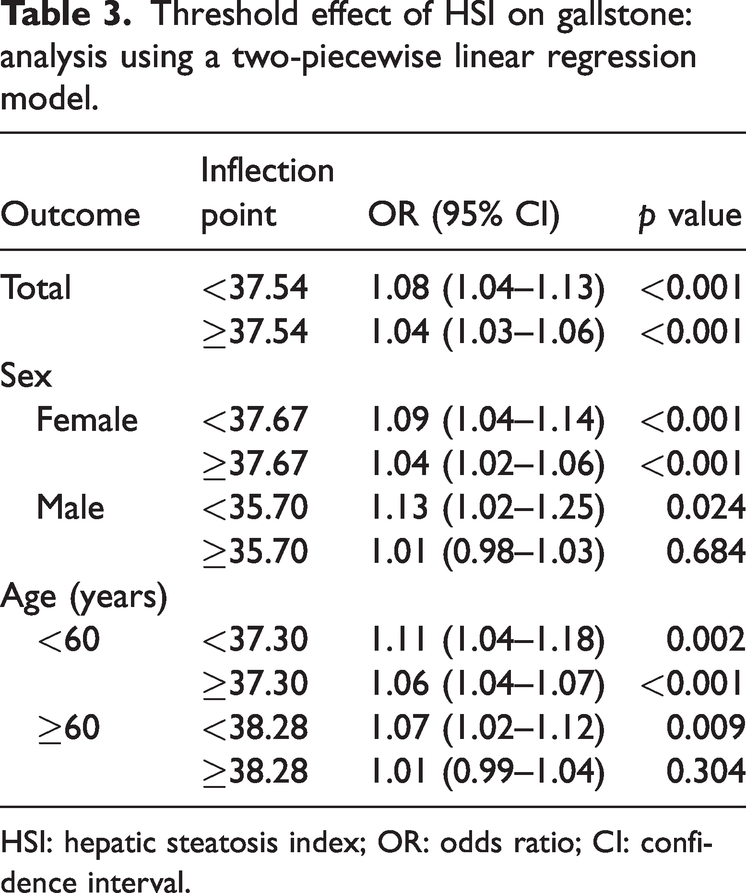
HSI: hepatic steatosis index; OR: odds ratio; CI: confidence interval.
In the sex-specific threshold analysis, the inflection point for women was 37.67. Below this value, each 1-unit increase in the HSI was associated with a higher risk of gallstones (OR = 1.09, 95% CI: 1.04–1.14; p < 0.001). For HSI ≥37.67, the increase remained significantly associated with the risk of gallstones (OR = 1.04, 95% CI: 1.02–1.06; p < 0.001). For men, the inflection point was 35.70. Below this threshold, each 1-unit increase in the HSI significantly increased the risk of gallstones (OR = 1.13, 95% CI: 1.02–1.25; p = 0.024). However, when the HSI was ≥35.70, the effect on gallstone risk was no longer significant (OR = 1.01, 95% CI: 0.98–1.03; p = 0.684).
In the age-specific threshold analysis, for individuals aged <60 years, the HSI inflection point was 37.30. Below this threshold, each 1-unit increase in the HSI significantly raised the risk of gallstones (OR = 1.11, 95% CI: 1.04–1.18; p = 0.002). For HSI ≥37.30, the effect on gallstone risk became more stable (OR = 1.06, 95% CI: 1.04–1.07; p < 0.001). For older participants aged ≥60 years, the inflection point for HSI was 38.28. Below this threshold, each 1-unit increase in the HSI was significantly associated with the risk of gallstones (OR = 1.07, 95% CI: 1.02–1.12; p = 0.009). However, when the HSI was ≥38.28, the effect on gallstone risk was no longer significant (OR = 1.01, 95% CI: 0.99–1.04; p = 0.304).
These findings suggest that the impact of HSI on gallstone risk varies by sex and age, and the risk of gallstones increases significantly within certain HSI ranges. Overall, the HSI demonstrates strong predictive ability for gallstone risk, particularly within key threshold intervals.
Subgroup analyses
Subgroup analyses were used to evaluate the potential influence of various factors on the relationship between the HSI and gallstone risk, as shown in Table 4. Sex-based analysis showed that the OR for women was 1.06 (95% CI: 1.04–1.07; p < 0.001), indicating a significant positive correlation between the HSI and gallstone risk in women. In contrast, the OR for men was 1.03 (95% CI: 0.99–1.06; p = 0.101), representing a statistically non-significant correlation. In terms of age, the OR for individuals aged <60 years was 1.07 (95% CI: 1.04–1.09; p < 0.001), showing a significant positive correlation. For those aged ≥60 years, the OR was 1.03 (95% CI: 1.01–1.06; p = 0.018), indicating a weak positive correlation.
Subgroup analysis of the association between HSI and gallstone risk.

We adjusted the model for age, race, educational level, marital status, smoking status, alcohol consumption, triglycerides, total cholesterol, GGT, HDLc, hypertension, and physical activity but did not adjust for the variables used in the subgroup analysis.
HSI: hepatic steatosis index; OR: odds ratio; CI: confidence interval; BMI: body mass index; GGT: γ-glutamyl transferase; HDLc: high-density lipoprotein cholesterol.
BMI analysis revealed a significant positive correlation between BMI ≥30 kg/m2 and gallstone risk (OR = 1.05, 95% CI: 1.03–1.07; p < 0.001). However, no significant correlation was observed for groups with BMI <25 and 25–29.9 kg/m2 (p = 0.085 and 0.308, respectively). Subgroup analyses for educational level, marital status, smoking status, alcohol consumption, and physical activity showed a significant positive correlation between the HSI and gallstone risk.
Specifically, for the lower educational level group, the OR was 1.07 (95% CI: 1.04–1.10; p < 0.001), and all marital status subgroups showed significant associations (p < 0.05). However, no significant interaction effects were observed for smoking status and alcohol consumption (p = 0.875 and 0.932, respectively). Notably, none of the interaction effects reached statistical significance (p for interaction > 0.05), indicating that the differences in the impact across subgroups did not significantly alter the relationship between the HSI and gallstone risk.
The RCS curves for sex and age subgroups showed an increasing trend in the relationship between the HSI and gallstone risk; however, the trends varied across sex and age groups (Figure 3). For women, the overall p value was <0.001, with a nonlinear p value of 0.044, indicating a nonlinear trend for the effect of the HSI on gallstone risk. The nonlinear p value for men was 0.082, which did not reach statistical significance. In the age analysis, those aged <60 years showed a linear upward trend (p < 0.001), while those aged ≥60 years displayed a nonlinear trend (p = 0.047).
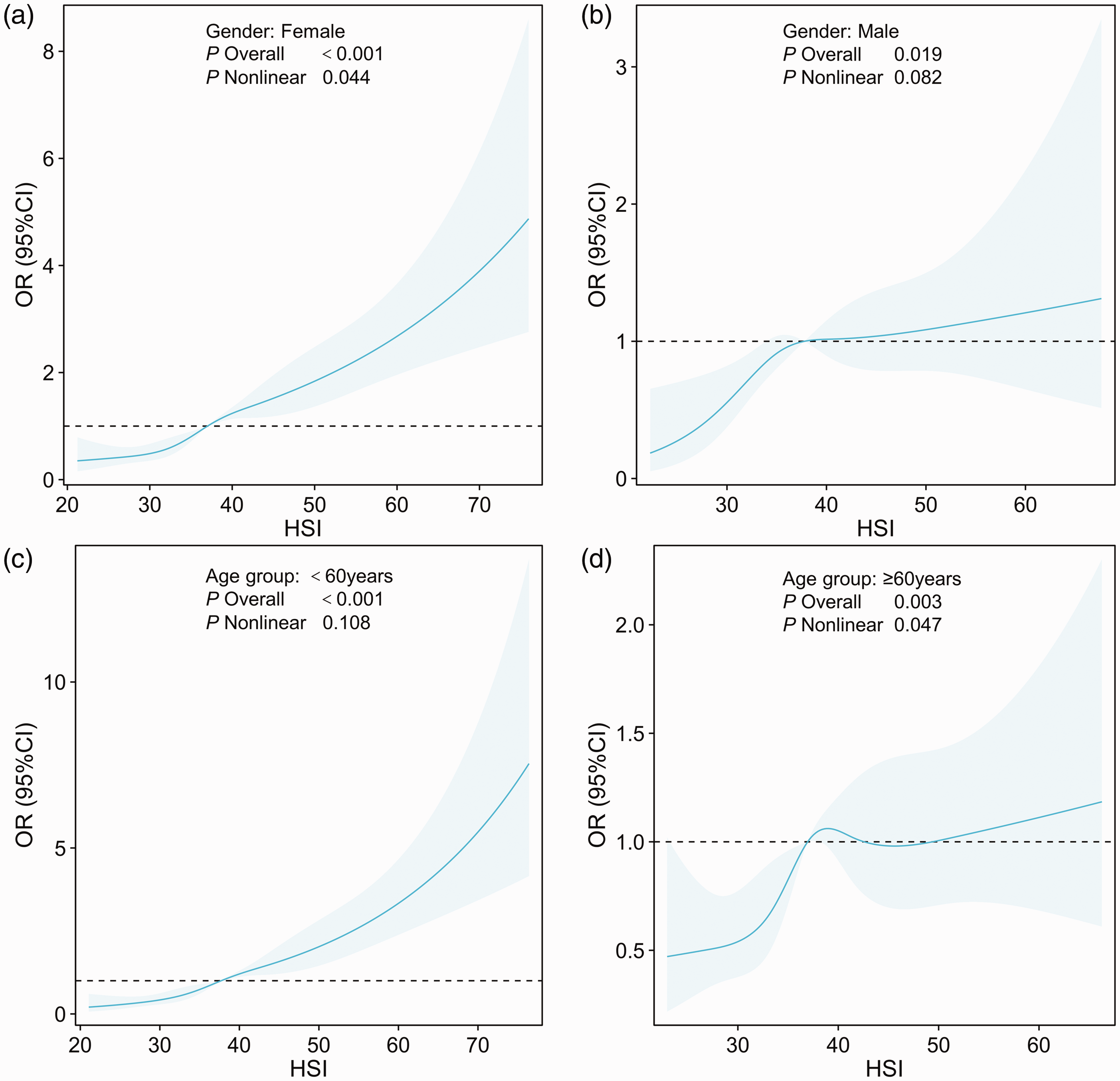
The association between the HSI and gallstone risk analyzed by sex, age, and BMI: (a) female, (b) male, (c) age < 60 years, (d) age ≥ 60 years. We adjusted the model for age, race, educational level, marital status, smoking status, alcohol consumption, triglycerides, total cholesterol, GGT, HDLc, hypertension, and physical activity but did not adjust for the variables used in the subgroup analysis. HSI: hepatic steatosis index; GGT: γ-glutamyl transferase; HDLc: high-density lipoprotein cholesterol.
Discussion
This study analyzed data from the NHANES database from 2017 to 2020 to explore the relationship between the HSI and gallstone risk. The findings indicated a significant positive correlation between the HSI and the risk of gallstones, with this relationship varying across different groups stratified by sex, age, and BMI. Specifically, for each unit increase in the HSI, the risk of gallstones significantly increased. Among the HSI quartiles, the Q4 group (HSI ≥ 43.3) showed a significant association with the risk of gallstones. Further nonlinear regression and threshold analyses revealed variations in the gallstone risk at different HSI values, particularly at a threshold of 37.54, where the association between the HSI and gallstone risk showed distinct risk increments. Moreover, subgroup analysis showed that the HSI had a more pronounced predictive effect for gallstones in women and individuals aged <60 years.
This study found a significant positive correlation between the HSI and gallstone risk, consistent with previous research. HSI, a simple and efficient noninvasive diagnostic tool, has been validated for its effectiveness in screening NAFLD and its related conditions, such as metabolic dysfunction–associated fatty liver disease.22,23 This study not only demonstrated the predictive potential of the HSI for gallstones but also suggested that gallstone formation is influenced by mechanisms such as fatty liver. Fatty liver is considered a potential risk factor for gallstone formation, with disruptions in fat metabolism potentially influencing gallstone development via alteration in bile composition and hepatic lipid accumulation. 24 Common metabolic disturbances in fatty liver patients, particularly the imbalance in cholesterol synthesis and clearance in the liver, are reported to be key factors in gallstone formation. 25 Alterations in the expression of cholesterol transport proteins in the liver, such as ABCA1 and NPC1L1, may lead to the supersaturation of cholesterol in the bile, promoting the formation of cholesterol crystals. 26
The diabetes component of the HSI reflects the presence of insulin resistance, which is not only a key marker of NAFLD but also a known risk factor for gallstones. Insulin resistance promotes gallstone formation through several mechanisms, including increased hepatic fat accumulation and alterations in cholesterol synthesis and bile acid metabolism.27,28 Studies have found that insulin resistance increases the concentration of free fatty acids in the liver, which, by inducing chronic inflammation, further exacerbates cholesterol metabolism disturbances, leading to excessive cholesterol accumulation. 29
In this study, threshold and subgroup analyses revealed the modulatory effects of sex and age on the relationship between the HSI and gallstone risk. Among women, the positive correlation between the HSI and gallstone risk was more pronounced, which may be attributed to characteristics such as fat distribution, hormone levels, and cholesterol metabolism in women. 7 After menopause, changes in hormone levels in women may promote hepatic fat deposition, 30 thereby increasing the risk of gallstone formation. In contrast, the relationship between the HSI and gallstone risk among men was weaker, which could be related to the different characteristics of fat metabolism and hormone levels in men. In the age group analysis, a linear relationship between the HSI and gallstone risk was observed in those aged <60 years, while a nonlinear relationship was noted in individuals aged ≥60 years. This finding suggests that with aging, hepatic fat accumulation may be influenced by other factors, such as the aging process and liver function decline, 31 leading to a different predictive pattern of the HSI for gallstones.
The main strength of this study lies in its use of the NHANES database, a large-scale and representative sample, which effectively reflects the health status of the adult population in the US. Furthermore, the use of HSI, a simple and efficient noninvasive indicator, enhances the clinical value of gallstone risk prediction. We carefully controlled for potential confounding factors such as age and blood lipids to improve the reliability and generalizability of our findings. Although this study provides important empirical evidence for the role of HSI in predicting gallstones, there are certain limitations. First, this study used a cross-sectional design, which cannot establish causal relationships. Therefore, future longitudinal studies should be conducted to validate the causal role of the HSI in the development of gallstones. Second, although the NHANES database provides extensive health data, its reliance on self-reported diagnoses of gallstones may have introduced reporting bias. Although the self-reported data have shown a high degree of consistency with imaging results, further verification is needed. Additionally, there is potential for selection bias due to the exclusion of participants with missing or incomplete data on key variables, which may impact the generalizability of the findings. Moreover, as the NHANES dataset is based on a non-institutionalized population, it does not include individuals living in hospitals or long-term care institutions; this may limit the broader applicability of the results. Finally, although this study controlled for several potential confounders, there may be other unaccounted factors, such as underlying liver diseases or genetic factors.
Conclusion
This is the first study to explore the relationship between the HSI and gallstone risk using the NHANES database, revealing a positive correlation between the HSI and gallstone risk. The HSI may serve as a predictor of gallstones, with stronger predictive ability in women and younger populations. Additionally, this study revealed a nonlinear relationship between the HSI and gallstone risk, indicating that the risk of gallstones may significantly increase within certain HSI ranges. Despite certain limitations, the results of this study provide new insights into the application of the HSI in gallstone risk assessment and offer a theoretical foundation for future clinical research and public health interventions.
Supplemental Material
sj-pdf-1-imr-10.1177_03000605251384456 - Supplemental material for The nonlinear relationship between the hepatic steatosis index and the risk of gallstones: A threshold analysis based on the National Health and Nutrition Examination Survey data
Supplemental material, sj-pdf-1-imr-10.1177_03000605251384456 for The nonlinear relationship between the hepatic steatosis index and the risk of gallstones: A threshold analysis based on the National Health and Nutrition Examination Survey data by Minghao Chen, Li Wang and Guodong Song in Journal of International Medical Research
Supplemental Material
sj-pdf-2-imr-10.1177_03000605251384456 - Supplemental material for The nonlinear relationship between the hepatic steatosis index and the risk of gallstones: A threshold analysis based on the National Health and Nutrition Examination Survey data
Supplemental material, sj-pdf-2-imr-10.1177_03000605251384456 for The nonlinear relationship between the hepatic steatosis index and the risk of gallstones: A threshold analysis based on the National Health and Nutrition Examination Survey data by Minghao Chen, Li Wang and Guodong Song in Journal of International Medical Research
Footnotes
Acknowledgements
We are grateful for the publicly available National Health and Nutrition Examination Survey (NHANES) data used in this study.
Author contributions
MHC: Conceptualized the study, designed the research methodology, and drafted the initial version of the manuscript. LW: Conducted the experiments, collected and analyzed the data, and contributed to the interpretation of the results. GDS: Conducted the literature review, provided critical feedback on the manuscript, and edited the final version for clarity and scientific rigor.
Declaration of conflicting interests
The authors declare no competing interests.
Funding
The authors declare that no financial support was received for this study.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.