
Abstract
This study presents the case of a male patient in his early 50s who was admitted with complaints of “recurrent low back pain accompanied by radiating pain in the left lower extremity for 3 years, with exacerbation over the past month.” Physical examination indicated that his symptoms were due to compression of the left L5 nerve root. Imaging findings corroborated the diagnosis of far-out syndrome secondary to left L5 nerve root compression caused by lateral osteophyte hyperplasia of the L5 and S1 vertebrae. Arthroscopic-assisted uni-portal spinal surgery was performed to treat the condition, during which the hyperplastic osteophytes were resected to achieve complete decompression of the affected nerve root. The patient showed significant symptomatic improvement postoperatively. At the 6-month follow-up, there was no recurrence, and his muscle strength and sensation had fully recovered. This case report aimed to provide a feasible minimally invasive alternative for the diagnosis and management of patients with similar conditions.
Keywords
Background
Far-out syndrome (FOS) denotes a pathological condition characterized by compression of the L5 nerve root at the extraforaminal level. Clinically, affected patients present with radiating pain involving the lower back, ipsilateral buttock, and lower extremity, often accompanied by numbness, impaired sensation, or muscular weakness—the hallmark symptomatology of L5 nerve root compromise. 1 Bertolotti syndrome is considered a form of FOS. 2 Common etiological factors underlying such compression include far-lateral intervertebral disc herniation, hypertrophy of the L5 transverse process, and enlargement of the sacral ala. Notably, only sporadic studies have documented cases in which compression arises from lateral osteophytic overgrowth of the L5 and S1 vertebrae. 3 Prior investigations have demonstrated that for FOS induced by lateral osteophyte-mediated compression, therapeutic interventions typically involve open surgical procedures or channel-assisted osteophyte resection. 4 Additionally, some researchers have explored the feasibility of laparoscopic osteophyte resection, 3 with all the abovementioned surgical modalities yielding satisfactory clinical outcomes.
In recent years, the arthroscopic-assisted uni-portal spinal surgery (AUSS) technique, first introduced by Professor Song En, has been widely adopted in clinical practice owing to its unique advantages. 5 Also known as uni-portal non-coaxial spinal endoscopic surgery (UNSES), AUSS is a minimally invasive spinal surgical system proposed by Professor Song En in 2021. The technique involves percutaneous bimanual operation through a single incision, with one hand holding the endoscope while the other manipulating surgical instruments, integrating the working and observation channels within the same incision. AUSS combines the triangulation principle of arthroscopy with the coaxial translation and swing techniques of spinal endoscopy while introducing its unique non-coaxial rotation method. Additionally, the endoscope and surgical tools can be switched between hands during the procedure to expand the operational space and enhance flexibility. This innovative approach offers magnified visualization of anatomical structures, provides clear intraoperative imagery under a water medium, and allows highly flexible manipulations. Beyond its established utility in managing common spinal pathologies such as intervertebral disc herniation and spinal stenosis, 6 AUSS has been successfully applied in complex scenarios—including thoracic spinal stenosis, resection of the atlas posterior arch, and dissection of thoracic tumors 7 —demonstrating substantial clinical potential. However, the existing literature contains relatively few reports on its application in the treatment of FOS, and no published studies have documented its use in resecting lateral osteophytes of the L5 and S1 vertebrae (inpatient at Yunnan Provincial Hospital of Traditional Chinese Medicine in June 2025). In the present report, we describe a case wherein the AUSS technique was employed to treat a patient with FOS secondary to lateral osteophytes of the L5 and S1 vertebrae, achieving excellent postoperative results. At the 6-month follow-up, the patient’s symptoms had fully resolved without recurrence. All patient details have been de-identified.
Case information
Medical history
The patient was a man in his early 50s who presented with the chief complaint of “recurrent low back pain accompanied by radiating pain in the left lower extremity for three years, with exacerbation over the past month.” Regarding history of present illness, 3 years ago, the patient developed low back pain of unknown etiology, accompanied by radiating pain in the left lower extremity, along with tingling and crawling sensations. He subsequently underwent multiple rounds of conservative treatment at other hospitals, which provided only temporary relief. One month ago, following overexertion, these symptoms recurred with increased severity, causing more intense pain and numbness in the left lower extremity. The patient then sought further evaluation at our hospital and was admitted as an outpatient with a preliminary diagnosis of “lumbar disc herniation.” Since the onset of the illness, the patient’s mental status has been moderate, physical strength poor, appetite and dietary intake normal, and sleep quality adequate. There has been no significant change in body weight, and both bowel and bladder functions have remained normal.
Regarding past medical history, the patient had a 5-year history of hypertension, with the highest recorded blood pressure of 150/90 mmHg. He was on a regular oral regimen of half a tablet of metoprolol succinate and one tablet of irbesartan, both taken once daily. He denied a history of chronic conditions such as coronary heart disease or diabetes. There was no history of previous surgeries, trauma, or blood transfusions. He also denied a history of infectious diseases, including hepatitis and tuberculosis, and his vaccination history was undocumented. Regarding allergy history, the patient reported no known allergies to food or medications. Regarding personal history, he had resided in the local area for an extended period. He had no history of exposure to epidemic-stricken areas, disease outbreaks, or contaminated water sources. His living and working conditions were favorable, with no exposure to industrial toxins, dust, or radioactive materials. Additionally, he did not have any habits of smoking, alcohol consumption, or drug use.
Physical examination
The spine showed no significant scoliosis or kyphosis. There were no scars on the local skin. Tenderness was present between the spinous processes of L4/5 and L5/S1 as well as on the left side of the vertebrae, with radiation to the left lower extremity. Lumbar forward flexion was slightly limited. The results of several tests were as follows. Straight leg raise test: left side approximately 65°, with a positive reinforcement test. Bilateral femoral nerve stretch test (−), bilateral “4” sign (−), bilateral hip flexion test (−), bilateral piriformis tension test (−), bilateral Oppenheim sign (−), bilateral patellar clonus (−), and bilateral ankle clonus (−); no other pathological signs were elicited bilaterally. The left extensor hallucis longus muscle strength was grade 3, while muscle strength in the remaining muscles of both lower extremities was normal. The left Achilles tendon reflex was diminished, the right Achilles tendon reflex was normal, and bilateral knee jerk reflexes were normal. Muscle tone and skin sensation in both lower extremities were normal. The visual analog scale (VAS) scores were 8 points for the left lower limb and 4 points for the back.
Imaging findings
The patient underwent a comprehensive series of lumbar imaging studies, including X-ray, computed tomography.(CT), and magnetic resonance imaging (MRI) scans. Lumbar X-rays (anteroposterior, lateral, flexion, and extension views; Figure 1) showed no evidence of spondylolisthesis or instability, although a transitional vertebral configuration was noted, characterized by the presence of six lumbar vertebrae. Lumbar CT (Figure 2) excluded vertebral destruction or spondylolysis but revealed left-sided osteophytic overgrowth involving the L5 and S1 vertebrae, resulting in nerve root compression. These findings were further confirmed by lumbar MRI (Figure 3), which corroborated the pathological changes described above.

(a) Anteroposterior lumbar X-ray; (b) Lateral lumbar X-ray; (c) Lumbar extension X-ray and (d) Lumbar flexion X-ray. The X-ray images showed no spondylolisthesis or instability. X-ray: radiography.

(a) Coronal lumbar CT showing lateral osteophyte formation on L5 and S1 vertebrae compressing the L5 nerve root (red arrow); (b) Axial lumbar CT showing hyperplastic osteophytes and (c) Axial lumbar CT showing hyperplastic osteophytes and the compressed nerve root (red arrow). CT: computed tomography.
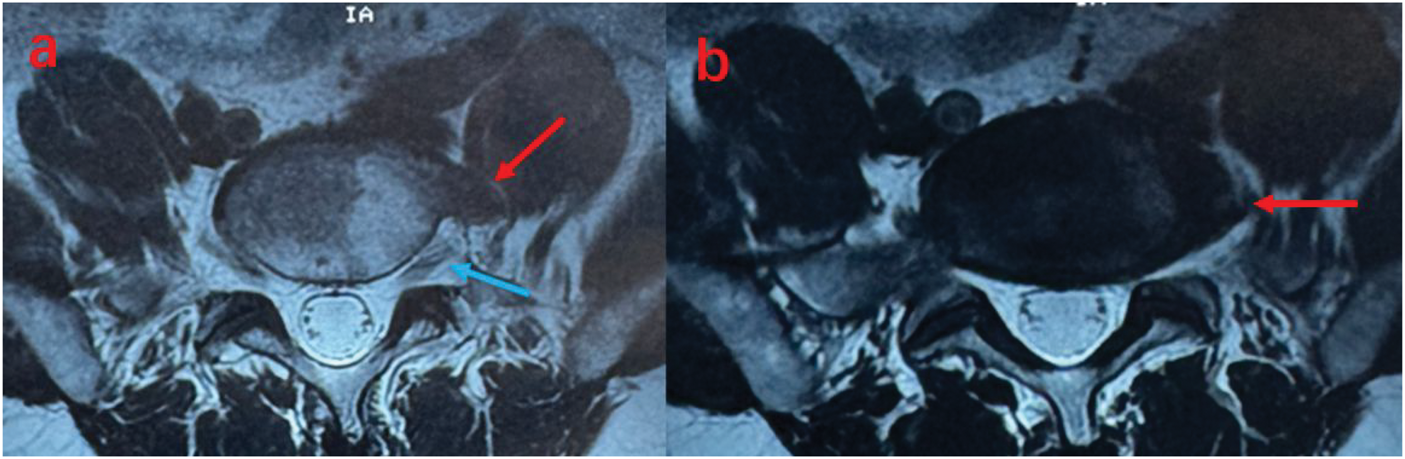
(a) Lumbar MRI showing hyperplastic osteophytes (red arrow) and the compressed nerve root (blue arrow) at the L5–S1 level and (b) Lumbar MRI showing hyperplastic osteophytes (red arrow) at the L5–S1 level. MRI: magnetic resonance imaging.
Diagnosis and treatment
Based on the patient’s clinical history, physical examination findings, and imaging data, a diagnosis of L5–S1 FOS was confirmed. 8 An AUSS procedure was performed to resect the lateral osteophytes of the L5 and S1 vertebrae, achieving complete decompression of the L5 nerve root. The steps of the surgical procedure were as follows: (a) Incision marking. A horizontal reference line was drawn at the L5–S1 intervertebral level, with a perpendicular vertical line at the lateral margin of the L5 transverse process. The intersection of these lines served as the center for a 2.5-cm incision, through which the skin and deep fascia were incised sequentially (Figure 4). (b) Surgical exposure. An arthroscope and radiofrequency device were introduced through the incision to visualize the operative field. Three key bony landmarks—the pars interarticularis, L5 transverse process, and sacral ala—were identified and exposed. A high-speed burr was used to contour these structures, enlarging the surgical corridor. The ligamentum flavum and intervertebral foramen ligaments were then excised to expose the underlying L5 nerve root. (c) Nerve decompression. The Hoffman ligaments, which anchor the nerve root, were resected to enhance its mobility. Following gentle retraction of the nerve root, ventral osteophytes were visualized and systematically removed using a bone chisel until complete decompression was achieved. (d) Closure. A drainage tube was inserted, and the incision was sutured in layers (Figure 5). The total operative time was 106 min. (e) Postoperative assessment. Follow-up CT scans confirmed significant osteophyte resection and comprehensive nerve root decompression (Figure 6).

Incision location map.
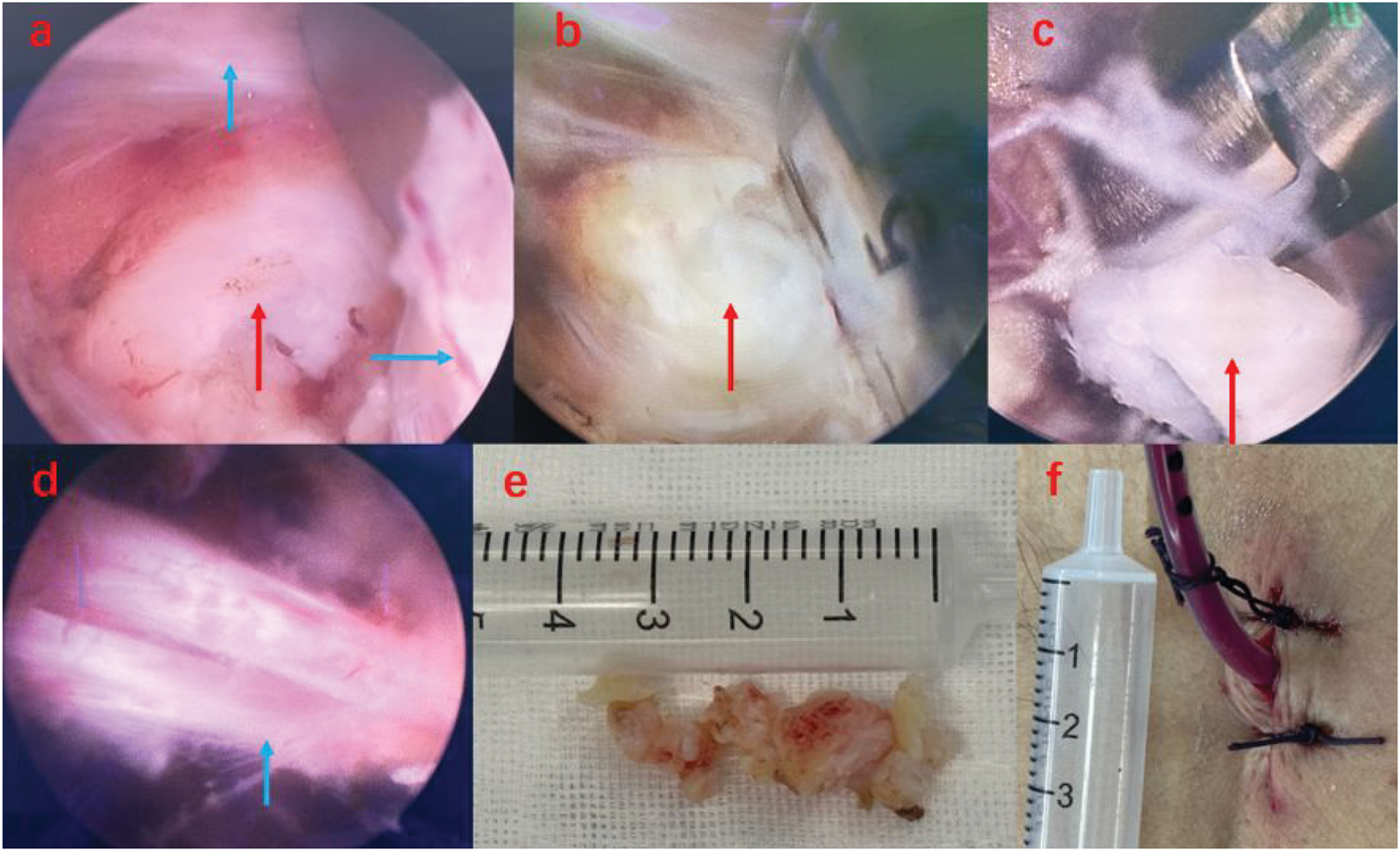
(a) Intraoperative view of protruding osteophytes (red arrow) and the overlying nerve root (blue arrow); (b) osteophyte resection using a bone chisel (red arrow); (c) removal of excised osteophytes with a nucleus pulposus forceps (red arrow); (d) decompressed nerve root (blue arrow); (e) resected osteophytes and (f) drainage tube placement and incision closure.

(a) Postoperative coronal CT showing near-complete osteophyte resection (red arrow); (b) axial CT demonstrating osteophyte removal (red arrow) and (c) 3D CT reconstruction showing the partially resected transverse process (blue arrow) and excised osteophytes (red arrow). CT: computed tomography; 3D: three-dimensional.
Treatment efficacy and follow-up
Immediately after surgery, the patient experienced marked alleviation of left lower extremity pain, with the VAS score decreasing to 2. The Oswestry Disability Index (ODI) score also improved, and numbness symptoms were significantly reduced, although muscle strength remained unchanged in the immediate postoperative period. Routine postoperative treatments, including infection prevention (cefmezole sodium injection, 1 g intravenous daily) and thrombosis prevention (subcutaneous injection of 0.4 mL of nadroparin calcium daily), were administered. The drainage volume was 20 mL within 24 h after surgery; the drainage tube was removed, and prophylactic medications were discontinued 24 h postoperatively. Follow-up CT scans confirmed complete resection of osteophytes and thorough decompression of the nerve root (Figure 6(c)). The patient was discharged on the third postoperative day, with instructions to wear a lumbosacral orthosis for 3 months. At the 3-month follow-up, the patient reported complete resolution of pain, further improvement of numbness, and recovery of left extensor hallucis longus muscle strength to grade 4. By the 6-month follow-up, both pain and numbness had fully resolved, and the muscle strength of the left extensor hallucis longus had returned to grade 5 (Table 1).
Comparison of clinical indicators before and after surgery.
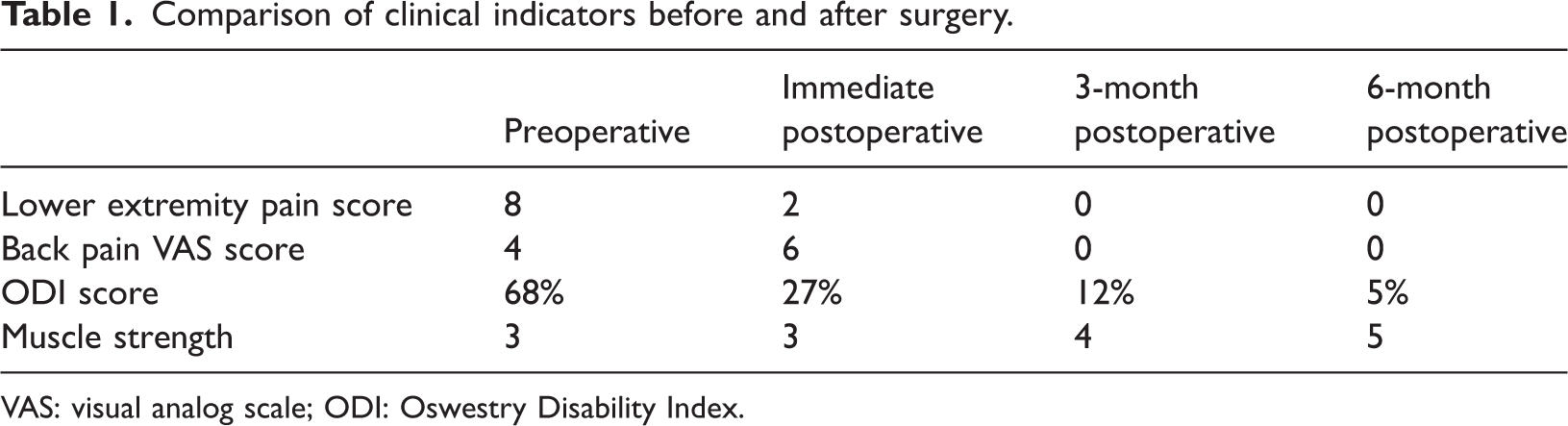
VAS: visual analog scale; ODI: Oswestry Disability Index.
Discussion
With ongoing advances in neural anatomy and disease pathophysiology, diagnostic precision for FOS and Bertolotti syndrome has improved, accompanied by an increasing number of reported cases. Nevertheless, accurate diagnosis and management of FOS remain a significant challenge in spinal surgery, often hindered by underdiagnosis or misdiagnosis. As it exits the intervertebral foramen, the L5 nerve root passes through a confined space bounded by the L5–S1 intervertebral disc, L5 transverse process, and sacral ala. Pathological changes in any of these structures can result in L5 nerve root compression, precipitating the severe radicular symptoms characteristic of FOS. Clinically, this presents as pain involving the lumbosacral region, buttocks, and unilateral lower extremity, accompanied by sensory deficits and muscle weakness. Physical examination typically reveals signs localized to the L5 nerve root innervation area, such as positive straight leg raise and reinforcement tests, along with altered cutaneous sensation. 9 In patients with L5 nerve root symptoms but without evident disc herniation or other compressive lesions at the L4–L5 level, FOS should be considered in the differential diagnosis. Careful distinction from confounding conditions—including piriformis syndrome, lateral femoral cutaneous nerve entrapment, and arteritis—is essential. Rigorous physical assessment and comprehensive imaging are critical to improving diagnostic accuracy, while advanced techniques—such as nerve root angiography, MRI neurography, and diagnostic nerve root blocks—further facilitate precise characterization of FOS. 10 In the present case, the patient demonstrated clear signs of L5 nerve root compression. No compressive pathology was identified at the L4–L5 level; however, extensive lateral osteophyte formation at the L5–S1 level, accompanied by definitive evidence of nerve root impingement on both coronal and axial CT sequences and corroborated by physical findings (e.g. diminished extensor hallucis longus muscle strength), supported a diagnosis of FOS based on strong clinical and radiological evidence.
The AUSS technique, pioneered by Professor Song En, offers several advantages, including high-definition, wide-field visualization, precise intraoperative localization, maneuverability, and a relatively spacious working area. Since its introduction, it has gained considerable recognition among clinicians, reflected by extensive clinical use and a growing body of published research. 11 AUSS differs from the unilateral biportal endoscopy (UBE) technique in its approach: UBE requires two separate incisions—one for the visualization channel and another for the operating channel—both positioned obliquely relative to the target site. In contrast, AUSS utilizes a single incision oriented perpendicular to the target, allowing both the endoscope and operative instruments to access the target site along a vertical trajectory. This design improves intraoperative positioning accuracy, reduces the risk of spatial disorientation during surgery, and provides unique clinical advantages. 12 As AUSS has evolved and gained wider adoption, its application has extended beyond common spinal pathologies to include rare and complex conditions, demonstrating its versatility. By offering surgeons enhanced endoscopic visualization and ergonomic operating conditions, AUSS represents a technique with substantial potential for broader clinical application. 13
Historically, the primary treatment for FOS involved open surgical procedures, such as anterior or oblique lateral approaches for osteophyte resection. However, open surgery carries risks, including potential injury to blood vessels, organs, sympathetic nerves, and lumbar muscles. With advancements in medical technology, microscopic and channel-based techniques have emerged as viable alternatives. 14 Some researchers have reported the use of transforaminal endoscopy for FOS management, 15 while others have recently explored O-arm-guided laparoscopic interventions. 9 Concurrently, with the increasing adoption of UBE, cases of FOS treated using this modality have also been documented. 16 Although these techniques achieve favorable outcomes, each has distinct advantages and limitations. Open surgery, for example, is associated with greater tissue trauma and increased intraoperative bleeding; the depth of the surgical field also limits visibility, making the procedure technically demanding and contributing to its declining use. In contrast, channel-based techniques overcome the limitations of restricted visualization and deep surgical access while minimizing incision size, leading to broader acceptance in FOS management. Additionally, studies have reported successful outcomes with lateral-position laparoscopic resection of vertebral osteophytes and with UBE, both demonstrating positive surgical results.
The emergence of the AUSS technique has introduced an innovative therapeutic option for FOS. In this study, based on experience and expertise gained from prior AUSS procedures, we employed the technique to resect lateral osteophytes in the patient described above. Intraoperatively, the nerve root and osteophytes were visualized with exceptional clarity, enabling thorough osteophyte excision and complete nerve root decompression, which contributed to excellent postoperative outcomes and favorable long-term follow-up results. While managing this FOS case, the AUSS technique demonstrated several distinct advantages. It provides enhanced intraoperative navigation. In UBE-assisted FOS surgery, the small target area and limited visualization of bony landmarks often result in intraoperative disorientation, requiring repeated fluoroscopic guidance. In contrast, AUSS substantially reduces the risk of spatial misorientation during initial site localization and surgical exposure, thereby decreasing dependence on fluoroscopy and streamlining the surgical workflow.
In this FOS case, the etiological factor—lateral osteophytes of the L5 and S1 vertebrae—represents a rarely reported source of compression, located more anteriorly than the typical sites at the L5–S1 interspace, L5 transverse process, or sacral ala. The clear and expansive field of view provided by AUSS enabled comprehensive exposure of the nerve root, from the lateral margin of the intervertebral foramen to its distal segments, as well as the ventral osteophytes. This enhanced visualization not only improved surgical safety but also broadened the scope of decompression. Notably, careful attention to the anatomical relationship between the osteophytes and the ipsilateral common iliac vessels is essential. When osteophytes are in close proximity to these vessels, meticulous dissection and cautious manipulation are required to avoid vascular injury, a potential cause of severe complications. For surgeons with limited endoscopic experience, alternative surgical approaches may be more appropriate for managing such complex cases.
Conclusion
The etiologies of FOS are multifactorial and complex. Beyond the well-recognized compressive factors at the L5–S1 intervertebral disc, L5 transverse process, and sacral ala, 17 clinicians should also consider lateral osteophyte formation at the L5 and S1 vertebrae, which can similarly precipitate L5 nerve root symptoms. As an advanced surgical modality, AUSS has demonstrated efficacy in resecting lateral vertebral osteophytes and achieving complete nerve root decompression. With advantages such as high-definition visualization, minimal intraoperative bleeding, faster postoperative recovery, and consistent therapeutic outcomes, AUSS warrants broader clinical adoption and application.
Footnotes
Acknowledgments
Not applicable.
Authors’ contributions
Y.C. and Y.L. contributed to the conception and design of the study. H.B., W.Z., and J.X. collected and analyzed the clinical data. B.Y. and C.L. prepared the figures and assisted with the interpretation of radiological findings. Y.C. and J.X. drafted the manuscript. Y.L. critically revised the manuscript for important intellectual content and supervised the overall study. All authors reviewed and approved the final version of the manuscript.
Availability of data and materials
All data generated or analyzed during this study are included in this published article.
Clinical trial number
Not applicable.
Consent for publication
The patient provided written informed consent for the publication of the clinical data presented in this manuscript.
Declaration of conflicting interests
The authors declare that they have no competing interests.
Ethics approval and consent to participate
This study was approved by the Medical Ethics Committee of Yunnan Provincial Hospital of Traditional Chinese Medicine (approval number: YYLW-2025-011). All procedures involving human participants were conducted in accordance with the ethical standards of the institutional and/or national research committee and the Helsinki Declaration, including its subsequent amendments. Informed consent was obtained from all participants prior to data collection.
Funding
Yunnan Provincial Department of Science and Technology Basic Research Program (No. 202101AZ070001-119), Yunnan Provincial Department of Science and Technology Basic Research Program (No. 202101AZ070001-178), Yunnan Provincial Department of Education Scientific Research Fund Project (No. 2024J0513), Yunnan Finance and Social Security (2025) (No. 92 2025), and Key Clinical Discipline Project of Traditional Chinese Medicine – Orthopedics.