
Abstract
Objectives
The relationship between the use of oral contraceptives and the risk of rheumatoid arthritis remains unclear. The objective of this meta-analysis was to comprehensively evaluate the association between oral contraceptive use and rheumatoid arthritis risk.
Methods
A systematic search was conducted in PubMed, EMBASE, and Cochrane Library databases for cohort studies published from 1980 to July 2024. Studies were assessed for bias using the Newcastle–Ottawa Scale. Two investigators independently screened abstracts and full-text articles and graded the certainty of evidence according to the Grading of Recommendations Assessment, Development and Evaluation approach. Data were analyzed using random effects models, and publication bias was evaluated using funnel plots and Egger test. A leave-one-out sensitivity analysis was performed, which demonstrated the robustness of the overall pooled estimate.
Results
Twelve cohort studies (1989–2024) with 1,126,554 participants were included. There was no significant overall association between oral contraceptive use and rheumatoid arthritis risk (relative risk = 0.96, 95% confidence interval: 0.93–1.00, I2 = 0.0%, p = 0.920). However, subgroup analysis revealed that oral contraceptive use for ≤5 years was associated with a higher risk of rheumatoid arthritis (relative risk = 1.08, 95% confidence interval: 1.01–1.16, I2 = 59.4%, p = 0.043). Current oral contraceptive use was linked to a reduced risk of rheumatoid arthritis (relative risk = 0.86, 95% confidence interval: 0.77–0.95, I2 = 0.0%, p = 0.840), while past oral contraceptive use showed no such association (relative risk = 0.94, 95% confidence interval: 0.87–1.02, I2 = 0.0%, p = 0.961). No publication bias was detected in the included studies (p = 0.183, Egger test).
Conclusions
This meta-analysis found no overall protective effect of oral contraceptive use on the risk of rheumatoid arthritis but suggested that current oral contraceptive use may lower the risk. Caution must be exercised while interpreting these results, particularly in studies with shorter follow-up periods, wherein the association might be stronger.
Introduction
Rheumatoid arthritis (RA) is an autoimmune disease characterized by synovitis and may eventually lead to joint deformity. The main symptoms of RA are joint swelling, stiffness, pain, and even loss of joint function, which severely compromise patients’ quality of life and cause significant inconvenience. The global incidence of RA is 0.5%–1%, 1 representing a substantial health burden on the society.
Several factors induce RA, including hereditary aspects, infection, environment, and smoking status. Many studies have suggested that estrogen plays an important role in RA pathogenesis. As per our clinical observations and literature review, women are more frequently diagnosed with RA than men.2,3 In addition, in patients with RA who are pregnant, the symptoms associated with RA are observed to gradually reduce during pregnancy.4–6
Oral contraceptives (OCs) typically contain a combination of different types of estrogen and/or progesterone. Since 1980, many epidemiological studies have compared the effect of estrogen and/or progesterone on RA risk between OC users and non-users7–10 and reported contradictory results. Koepsell et al. 7 and Hazes et al. 8 found that OCs may exert a certain protective effect on RA onset, while Chen et al., 9 Spector and Hochberg, 10 and Adab et al. 11 found no significant association between OC use and RA risk.
To minimize biases that may be present in these studies, we performed a meta-analysis of 12 cohort studies published between 1987 and 2024 that examined the association between OC use and RA risk to summarize the evidence and accurately estimate the association.
Materials and methods
This study adhered to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines 12 and followed a preregistered protocol available on the International Prospective Register of Systematic Reviews (PROSPERO) platform (CRD42024618928).
Search strategy
Studies assessing the relationship between OC use and RA risk were identified from PubMed, Corchrane, and EMBASE databases using the following search terms: (“oral contraceptives” OR “estrogens”) AND (“rheumatoid arthritis” OR “RA”) AND (“risk”). The last search was performed on 8 July 2024. The bibliographies of relevant articles were checked manually for additional publications of interest. Detailed description of the search protocol is presented in Supplementary Table 1. The retrieved articles were uniformly imported into the NoteExpress database (NoteExpress V4.X, Beijing Aegean Hailezhi Technology Co., LTD.) for subsequent screening.
Inclusion criteria
Studies were included if they met the following inclusion criteria: (a) patient population, patients with RA; (b) exposure, history of OC use; (c) comparator, healthy participants; (d) results, quantitative point estimates (hazard ratios or relative risks (RRs); and (e) study type, prospective or retrospective cohort study.
The exclusion criteria were as follows: (a) summaries of meetings or letters to the editor; (b) repeated publication; (c) patients diagnosed only with arthritis or lacking a clear diagnosis of RA; and (d) incomplete data or no results of interest.
Data collection
To ensure comprehensive and unbiased study selection, two authors (Liudan Luo and Hejing Pan) independently performed the screening process. Initially, all retrieved references were imported into EndNote (version 21), where duplicate studies were identified and removed using the software’s automated deduplication feature. Following deduplication, the remaining references were subjected to preliminary screening, wherein both authors independently reviewed the titles and abstracts of each reference to systematically exclude studies that were irrelevant or duplicates that were missed by the software. The full texts of the studies considered potentially eligible based on this initial screening were retrieved for further evaluation. Throughout the screening and full-text assessment stages, any disagreements between the two primary reviewers were resolved through discussion. If consensus could not be reached, Xuanlin Li (third reviewer) mediated the discussion to facilitate decision-making and arrive at a decision.
In the analysis, we extracted information about the first author, study location, age of the study population, number of participants, study design, year of case diagnosis or cohort enrollment, length of follow-up for cohort studies, OC exposure assessment method, adjusted RR estimates with corresponding 95% confidence intervals (CIs) from a multivariable model, match factors, and covariates adjusted for.
Quality assessment
We used the Newcastle–Ottawa Scale (NOS) 13 to assess the quality of the included studies based on three aspects: selection, comparison, and results. The NOS scores range from 0 to 9, with higher stars indicating better study quality. Specifically, it assesses the study quality based on three domains: (a) selection of study participants (4 points); (b) comparability between the groups (2 points); and (c) measurement of the exposure factor (3 points). NOS scores ≥7, 4–6, and 0–3 are considered to indicate high-, medium-, and low-quality studies, respectively.
Statistical analyses
Analyses were conducted using STATA version 14 and version 16 (STATA Corporation, College Station, TX, USA). The measure of interest was the RR. Odds ratios (ORs) were considered equivalent to RRs because RA risk was a rare outcome. 14 A random-effect model with the DerSimonian and Laird method, which accounts for heterogeneity across studies, was employed to calculate the pooled RR. We evaluated the heterogeneity using the Cochran’s Q and I2 statistics. Significant heterogeneity was defined based on whether the p-value for heterogeneity was <0.10 or I2 was >50%. Stratified analyses were performed according to duration of OC use and geographical location (European vs. North American vs. Asian studies). In addition, sensitivity analyses were performed to investigate the effect of adjusted confounders (i.e. smoking status, parity, body mass index (BMI), and marital status) on RA risk. We conducted a sensitivity analysis to assess the impact of individual studies on the overall results by excluding one study at a time. Potential publication bias was evaluated using Begg’s funnel plots and quantified using Egger’s test; a p-value <0.05 was considered to indicate statistical significance. The meta-analysis compared OC users and non-users, different durations of OC use, and OC use status. With respect to the duration of OC use, we defined short-term use as ≤5 years and long-term use as >5 years.
Quality of evidence assessment (Grading of Recommendations, Assessment, Development, and Evaluations (GRADE) approach)
The quality of evidence for the main outcome was assessed using the GRADE approach. Two reviewers (Liudan Luo and Hejing Pan) independently evaluated the evidence based on five criteria, namely, risk of bias, inconsistency, indirectness, imprecision, and publication bias. The evidence was initially rated as “high quality” for observational studies and was downgraded by one or two levels for serious or very serious concerns within each domain. Any disagreements were resolved through discussion or via consultation with a third reviewer (Xuanlin Li). The evaluation was conducted manually by the reviewers according to the GRADE guidelines, rather than using software.
Results
Search results and study characteristics
Based on our search terms, a total of 1455 publications were identified from PubMed, Cochrane Library, and EMBASE databases. Figure 1 presents the flowchart of the literature screening process.

Flowchart illustrating the literature screening process.
We identified 22 publications for full-text evaluation. Of these, 10 were excluded because they did not meet the inclusion criteria; they were either abstracts of articles,15–19 contained inaccurate data,20–23 or did not use the standard RA diagnosis criteria. 24 Therefore, our meta-analysis was based on 12 cohort studies published between 1987 and 2024.11,25–35 All studies were published in English. Other characteristics of the included studies are listed in Table 1.
Characteristics of 12 included studies examining the association of RA risk with OC use.
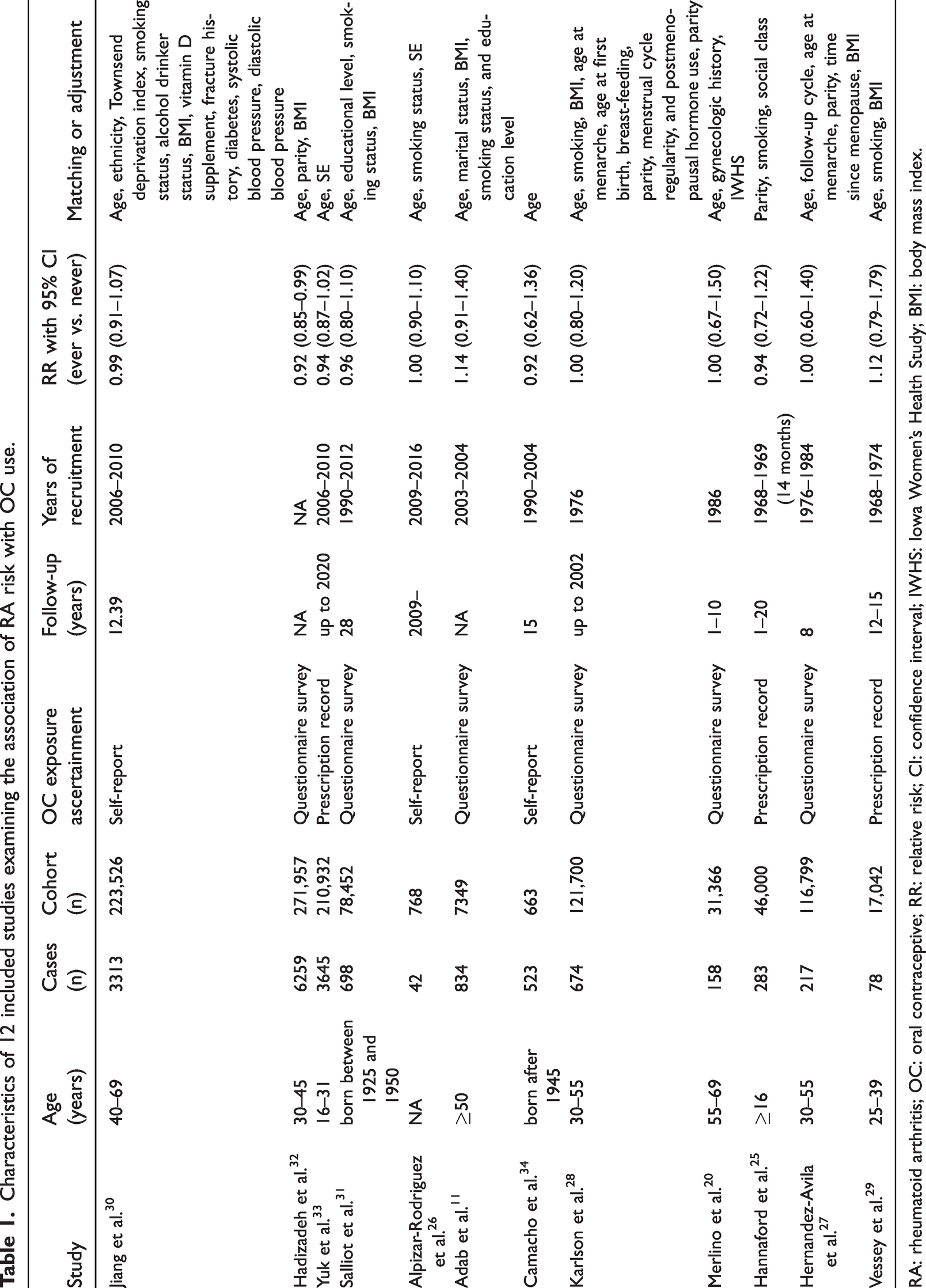
RA: rheumatoid arthritis; OC: oral contraceptive; RR: relative risk; CI: confidence interval; IWHS: Iowa Women’s Health Study; BMI: body mass index.
Quality assessment
The NOS was used to evaluate the quality of the included studies. The evaluation indicators included sample selection, comparability, and exposure factors (Table 2). The average score of the included studies was ≥6 points, including four studies with 6 points, four with 7 points, and five with 8 points, resulting in an average score of 7.08 points. This indicates that the quality of this meta-analysis is high. The detailed NOS scores are presented in Table 2.
Quality of cohort studies based on the Newcastle–Ottawa Scale.

Overall association of OC use with RA risk
Figure 2 presents the study-specific and combined RRs of RA among OC users versus non-users, with corresponding 95% CIs. The total estimate was 0.96 (95% CI: 0.93–1.00, I2 = 0.0%, p = 0.920). In subgroup analysis by geographical location, the estimates for Europe, North America, and Asia were 0.96 (95% CI: 0.92–1.01, I2 = 0.0%, p = 0.883), 1.00 (95% CI: 0.85–1.18, I2 = 0.0%, p = 1.0), and 0.96 (95% CI: 0.89–1.04, I2 = 63.1%, p = 0.01), respectively. Considering the adjusted subgroups, the association of OC use with RA risk did not change significantly based on smoking status, parity, BMI, or marital status (Table 3). In the analysis of OC use duration, the pooled RR was 0.97 (95% CI: 0.83–1.14, I2 = 0.0%, p = 0.738), indicating a lack of statistical significance at a level of 0.10 for cohorts with short-term OC use, and the combined RR was 1.08 (95% CI (1.01–1.16), I2 = 59.4%, p = 0.043), indicating statistical significance at a level of 0.10. In the analysis of OC use status, the pooled RR was 0.94 (95% CI: 0.87–1.02, I2 = 0.0%, p = 0.961) for former/never users and 0.86 (95% CI: 0.78–0.95, I2 = 0.0%, p = 0.840) for current/never users, both indicating a lack of statistical significance at a level of 0.05.

Forest plot showing study-specific and pooled RRs of RA among OC users versus non-users.
Subgroup analyses of RRs for the association between RA risk and OC use.

BMI: body mass index; RR: relative risk; RA: rheumatoid arthritis; OC: oral contraceptive; CI: confidence interval.
Publication bias
Visually, the funnel plot assessing the efficacy of OCs in patients with RA appeared symmetrical. In addition, the Egger test showed no publication bias (p = 0.183). The funnel plot is presented in Figure 3.

Funnel plot assessing publication bias in studies on OC use and RA risk. RA: rheumatoid arthritis; OC: oral contraceptive.
GRADE certainty of evidence
The GRADE evidence level for the association of OC use with RA risk is generally low. Specifically, the evidence for the duration of OC use and the effect of geographical location is rated “very low,” while that for other factors is rated “low.” This evidence level has consistently been rated as “low” in high-, moderate-, and low-quality studies. The certainty of the relevant evidence is detailed in Table 4.
GRADE assessment of the certainty of evidence.

OC: oral contraceptive; GRADE: Grading of Recommendations Assessment, Development and Evaluation; RA: rheumatoid arthritis.
High heterogeneity.
Discussion
Female hormones have long been considered to play an important role in many human immune diseases. However, several epidemiological studies evaluating the relationship between OC use and RA risk have reported conflicting results. To clarify this association, we reviewed six systematic reviews or meta-analyses published between 1989 and 2024.9,35–39
Meta-analyses have reported conflicting results. In a meta-analysis of 13 case–control studies, Qi et al. found that OC use did not exert a protective effect against RA onset (RR = 0.81, 95% CI: 0.63–1.05). 38
Spector and Hochberg reported that OC use was associated with a reduced risk of RA (RR = 0.73, 95% CI: 0.61–0.85). 10 Chen et al. found that OC use was negatively correlated with RA severity and that OC could prevent RA progression (OR = 0.41, 95% CI: 0.22–0.78). 9
Thus, we updated our meta-analysis. Specifically, in our study, we included all studies published to date; excluded overlapping data; (analyzed variables such as source of control, geographical location, marital status and parenthood, educational level, and smoking status; analyzed the dose–response relationship between the duration of OC use and RA risk; assessed the association of current and past OC use with RA risk; and performed publication bias tests for subgroups.
Our current meta-analysis of 12 cohort studies showed no significant association of OC use with RA risk (RR = 0.96, 95% CI: 0.93–1.00). However, some subgroups showed significant differences that warrant further exploration. All subgroup findings are hypothesis-generating and require validation in dedicated studies. Uncorrected multiple testing increases the false-positive risk; thus, nominal p-values should not be over-interpreted.
To assess the impact of OC use duration, we categorized participants as short-term users (OC use duration ≤5 years) or long-term users (OC use duration >5 years). There was an increase in the risk of RA among short-term users, with a statistically significant RR of 1.08 (95% CI: 1.01–1.16). The marginal increase in the RA risk with short-term OC use (≤5 years) warrants further investigation. Although protopathic bias (e.g. OC discontinuation due to prodromal RA symptoms) is a concern, transient proinflammatory effects of early OC adaptation merit investigation in seropositive subgroups. There was moderate heterogeneity in this subgroup (I2 = 59.4%). Further exploration of the causes of heterogeneity revealed that in cases where the duration of OC use was 0–2 years, OC use may not exert any effect on RA onset due to the short duration of action.
Notably, our analysis showed that current use of OC was a protective factor, with an RR of 0.858 (95% CI: 0.77–0.947). However, there was no significant association between OC use and RA risk among past OC users (RR = 0.942, 95% CI: 0.874–1.015). Among the studies discussing the risk of developing RA due to the previous use of OCs, our findings should be interpreted in the context of a recent and comprehensive meta-analysis by Marino et al., 39 which investigated a highly similar research question. Notably, both meta-analyses, despite some methodological differences, establish the same key conclusion: “ever use” of OCs is associated with a statistically significant protective effect against RA development (Marino et al.: OR = 0.80, 95% CI: 0.70–0.91; our study: OR = 0.86, 95% CI: 0.78–0.95). This strengthens the evidence in support of a beneficial role of OC use. There is a primary methodological distinction in the inclusion criteria of these two studies. Our analysis was restricted to cohort studies to prioritize a higher level of evidence for causal inference and minimize potential recall bias; however, Marino et al.’s study included both cohort and case–control studies, which may have enhanced the statistical power but also introduced greater heterogeneity, as indicated by the high I2 values for their “current use” and “past use” subgroups. This difference in the inclusion of studies may explain the more precise estimate we obtained for the overall effect and the variations in subgroup analyses. Therefore, our study complements the findings of Marino et al. by providing estimates derived solely from prospective and retrospective cohort designs, offering a distinct perspective on this topic. The subgroup analysis with n = 3 was considered exploratory. Given the reduced statistical power, the results should be regarded as hypothesis-generating. Future large-scale research is needed to verify these trends.
The Asian subgroup analysis (n = 2) showed substantial statistical heterogeneity (I2 = 63.1%); however, this result could not be interpreted owing to the lack of sufficient studies on this topic. These preliminary data solely highlight the need for future large-scale studies in diverse populations.
The potential limitations of current meta-analyses need to be addressed. First, although the data are reliable and referential because our analysis is mainly based on cohort studies, unmeasured confounders may have exerted notable effects, as is commonly observed in observational studies. The subgroup analysis suggests that the association between OC use and RA risk is not influenced by confounding factors such as BMI, marital status, region, parity, and smoking status; however, the possibility that our findings are influenced by other unmeasured confounders cannot be ruled out. Furthermore, our subgroup analyses based on adjustment for confounders (e.g. smoking status, parity, and BMI) must be interpreted with considerable caution. A key limitation of this meta-analysis, inherent to the methodology, is the substantial variation in confounding adjustment strategies across the included cohort studies (Table 1). Although we attempted to explore the potential influence of these factors by grouping studies that reported adjustments for a specific confounder versus those that did not, these comparisons are not equivalent to a standardized, individual patient-level adjustment. Consequently, the observed differences between subgroups may not solely reflect the true effect of the confounder but could also indicate the influence of residual confounding, variations in study design, and differences in how variables were defined and measured across the primary studies. This lack of standardization highlights a critical challenge in synthesizing evidence from observational research and underscores that our findings regarding these specific confounders should be viewed as exploratory and hypothesis-generating. Future primary studies with more consistent and comprehensive adjustment for key confounders are needed to provide more definitive insights. Second, we could not assess the association of OC composition with RA risk. In the 1980s, OCs were markedly different from those used later in terms of lower estrogen content and three-phase dosing. 40 Thus, the association of OC composition with RA risk remains unclear. Third, the diagnosis of RA was based on different diagnostic criteria in the various included studies, potentially leading to misdiagnosis and incorrect classification of participants. Finally, publication bias may have existed; studies that report a weak or absent association are less likely to be published than those reporting statistically significant results. Although Egger’s test and Begg’s funnel plot did not detect evidence of publication bias in our meta-analysis, these results may not be completely reliable, given the relatively small number of included studies.
Taken together, the results of the current meta-analysis of 13 cohort studies suggest that there is no relationship between OC use and RA risk. However, certain issues warrant resolution. Further large-scale prospective studies are needed to rigorously select eligible cases based on the latest American College of Rheumatology classification criteria, standardize OC formulations, clearly report the OC dose and use duration, and account for confounding factors to further validate our findings.
Supplemental Material
sj-pdf-1-imr-10.1177_03000605251391940 - Supplemental material for Oral contraceptives and the risk of rheumatoid arthritis in women: A systematic review and meta-analysis
Supplemental material, sj-pdf-1-imr-10.1177_03000605251391940 for Oral contraceptives and the risk of rheumatoid arthritis in women: A systematic review and meta-analysis by Liudan Luo, Hejing Pan, Xuanlin Li and Lin Huang in Journal of International Medical Research
Footnotes
Acknowledgements
None.
Author contributions
Liudan Luo (First author): Conceptualization, Data Curation, Formal Analysis, Investigation, Methodology, Software, Visualization, Writing–Original Draft, Writing–Review & Editing;
Hejing Pan: Methodology, Supervision, Data Curation, Investigations;
Lin Huang (Corresponding author): Conceptualization, Funding Acquisition, Resources, Supervision, Validation, Writing–Original Draft, Writing–Review & Editing;
Xuanlin Li: Supervision, Validation.
All authors have read and approved the current version of the manuscript.
Author statement
We declare that this manuscript is original, has not been published before and is not being considered for publication elsewhere.
Data availability statement
The data analyzed in this meta-analysis were obtained from publicly available databases, including PubMed, Cochrane Library, and EMBASE. All original datasets can be accessed through their respective platforms using the search strategies described in the Methods section. The extracted data supporting the findings of this study are available from the corresponding author upon reasonable request.
Declaration of conflicting interests
There are no conflicts of interest in this study.
Funding
This work was supported by the Zhejiang Provincial Natural Science Foundation of China (Grant Number LY24H270004).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.