
Abstract
Objective
This meta-analysis explored the diagnostic value of anti-cyclic citrullinated peptide antibody (anti-CCP) and rheumatoid factor (RF) for rheumatoid arthritis (RA) in the Asian population.
Methods
Embase, Medline, Cochrane Library, Chinese Science and Technology Periodicals, China National Knowledge Infrastructure, and China Wanfang Databases were searched from 1 January 2000 to 1 February 2021 to collect studies on the combined detection of anti-CCP and RF for diagnosing RA. The sensitivity, specificity, diagnostic odds ratio (DOR), positive likelihood ratio (+LR), and negative likelihood ratio (−LR) were combined and analyzed. Summary receiver operating characteristic (SROC) curves were drawn.
Results
Twenty-four published papers were analyzed, including 21 combined in series and 8 combined in parallel. In the tandem analysis, the sensitivity = 0.64 [95% confidence interval (CI): 0.58–0.70], specificity = 0.97 (95%CI: 0.95–0.98), +LR = 19.70 (95%CI: 12.74–30.46), −LR = 0.37 (95%CI: 0.31–0.43), DOR = 53.43 (95%CI: 34.46–82.40), and area under the SROC curve = 0.89. In the parallel combination, the sensitivity = 0.87 (95%CI: 0.80–0.92), specificity = 0.76 (95%CI: 0.67–0.84), +LR = 3.68 (95%CI: 2.62–5.17), −LR = 0.17 (95%CI: 0.11–0.26), DOR = 21.56 (95%CI: 11.63–39.99), and area under the SROC curve = 0.89.
Conclusion
Anti-CCP and RF combined detection improves the diagnostic efficiency of RA, providing a potential strategy for early clinical screening in the Asian population.
This trial was retrospectively registered in the INPLASY/Research Registry (https: //inplasy.com/) with the registration number INPLASY202180106.
Keywords
Introduction
Rheumatoid arthritis (RA) is a multi-systemic inflammatory autoimmune disease that mainly affects the surrounding joints, with a worldwide prevalence of 1%.1–3 In low- and middle-income countries, such as Southeast Asia, the prevalence of RA is slightly lower than that in Europe, The Americas, and the Western Pacific. 4 For example, in China, the prevalence is 0.32% to 0.5%, and the total number of patients affected is approximately 5 million. 5 The joints of patients with RA are stiff, deformed, and dysfunctional, leading to disability in severe cases. 6 Patients with RA mainly show chronic inflammation throughout large and small joints and abnormal proliferation of rheumatoid arthritis synovial cells in the diseased joints.7,8 Its specific etiology is unclear and may be related to two factors: infectious agents and genetic predispositions.9,10 Therefore, early diagnosis and treatment are particularly crucial for patients with RA.
Previous clinical diagnostic criteria for RA are mainly based on clinical manifestations (symptoms and signs), rheumatoid factor (RF) detection, and imaging (X-ray) examination. In the early stage of RA, drug treatment effectively controls the disease and alleviates disease progression. 11 However, drug treatments show poor efficacy in the late stage. To achieve the early diagnosis and treatment of patients with RA and reduce bone erosion in those with advanced RA, identifying autoantibodies that can be detected at an early stage with good specificity is of great significance. 12 In recent years, the detection of autoantibodies, such as RF and anti-cyclic citrullinated peptide (anti-CCP), has provided an important basis for early diagnosis and disease activity evaluation. 5 , 6 , 12
Currently, RF is one of the most commonly used serum indicators for the diagnosis of RA, which has certain sensitivity but poor specificity. RF tests show a 5% to 10% false-positive rate, 13 indicating low specificity. In 2000, Schellekens et al. first artificially synthesized CCP and detected serum anti-CCP levels in patients with RA, demonstrating a high specificity and sensitivity in RA diagnosis. 14 Researchers have comprehensively confirmed the clinical application value of anti-CCP in the diagnosis of RA.15,16 A study conducted by Zeng et al. in 2001 suggested that the specificity and sensitivity of anti-CCP were 96.6% and 46.6%, respectively. 17 Bizzaro et al. 18 found that anti-CCP levels were highly correlated with early RA and not significantly correlated with patient’s general clinical data (sex and age). Moreover, some studies have explored the significance of the combined detection of RF and anti-CCP in the diagnosis of RA. 19
To objectively evaluate the clinical applicability of the combined detection of RF and anti-CCP in the diagnosis of RA, this meta-analysis systematically evaluated published trials in the Asian population, thereby providing a theoretical and clinical basis for the use of this combined detection method for the diagnosis of RA.
Methods
Retrieval strategy
This trial was retrospectively registered in the INPLASY/Research Registry (https: //inplasy.com/) with the registration number INPLASY202180106. We conducted this meta-analysis based on the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA). 20 Because this study was a meta-analysis, ethical board approval and informed consent were not required. Two investigators independently collected relevant literature from the Excerpta Medica Database (Embase), Medline, Cochrane Library, Chinese Science and Technology Periodicals Database, China National Knowledge Infrastructure (CNKI), and China Wanfang Database from 1 January 2000 to 1 February 2021 to evaluate the diagnostic value of RF and anti-CCP combined tests for RA in Asia. The retrieval strategy was as follows: (“anti-cyclic citrullinated peptide antibody” OR “anti-CCP”) AND (“rheumatoid factor” OR “RF”) AND (“rheumatoid arthritis” OR “RA”). Additional references were obtained from review articles, guides, and conferences as necessary. All studies were independently extracted by two researchers and then cross-checked. Any disagreements were resolved through discussion.
Literature inclusion and exclusion criteria
The inclusion criteria were as follows: (1) study on the diagnosis of RA by the combined detection of RF and anti-CCP, (2) reported the sensitivity and specificity of the combined detection of RF and anti-CCP in RA or provided the information necessary to calculate the sensitivity and specificity, and (3) subjects were the Asian population.
The following exclusion criteria were used: (1) research with repeated content, (2) research with incomplete original data, (3) full text of the original research unavailable, and (4) conference abstracts, summaries, guidelines, letters, and case reports.
Quality assessment
The Quality Assessment of Diagnostic Accuracy Studies (QUADAS-2) 21 was used to assess the quality of all included studies. The checklist contained 11 standards, with each evaluated as “yes”, “no”, and “unclear”. “Yes” satisfied the criterion, “no” meant not satisfied or not mentioned, and “unclear” was defined as partial satisfaction or insufficient information from the literature.
Data extraction
The following information was extracted: 1) author, year of publication, country, language, age group of subjects, number of cases, cut-off value and 2) number of true positives, false positives, false negatives, and true negatives. All data were independently extracted by two researchers and then cross-checked.
Statistical analysis
Using Stata 15.0 Statistical Software (Stata Corp, College Station, TX, USA), a meta-analysis of diagnostic test accuracy was performed. Spearman’s correlation coefficient was applied to evaluate the diagnostic threshold effect. Heterogeneity was assessed using Cochran’s Q statistic and the I2 index. The pooled sensitivity, specificity, positive likelihood ratio (+LR), negative likelihood ratio (−LR), and diagnostic odds ratio (DOR) were calculated using a bivariate mixed model. The area under the curve (AUC) was calculated using the summary receiver operating characteristic (SROC) curve to analyze the diagnostic performance of the combined detection of RF and anti-CCP for RA. AUC values in the range of 0.5 to 0.7 indicated low diagnostic value, AUC values in the range of 0.7 to 0.9 indicated moderate diagnostic value, and AUC values greater than 0.9 indicated high diagnostic value. The overall sensitivity and specificity of the selected studies were summarized through a bivariate mixed model. Deek’s funnel plot was used to assess publication bias. Finally, sensitivity analysis was conducted to verify the robustness of the conclusion. If P < 0.05, the difference was statistically significant.
Results
Literature research and study characteristics and quality
Based on the strict inclusion and exclusion criteria, 24 published papers were included in this meta-analysis,22–45 including 21 combined in series and 8 combined in parallel. In total, 7151 cases of RA and 5913 controls were included. Among them, 5 studies contained parallel and series diagnostic data.23,24,29,30,43 The screening flow diagram was shown in Figure 1, and an overview of the included literature was shown in Table 1. The quality of the included literature was displayed in Figure 2 (A, B).

A flow diagram of the study selection process.
General characteristics of the reviewed studies and the primary results.

FN: false negative, FP: false positive, TN: true negative, TP: true positive, NR: non-report, RA: rheumatoid arthritis, NRA: not rheumatoid arthritis, RF: rheumatoid factor, anti-CCP: anti-cyclic citrullinated peptide, RU: relative units.

Results of literature quality evaluation following QUADAS-2. A: Bar chart showing the quality score of diagnostic test literature; B: Methodological quality evaluation results. + represents Yes, − represents NO, and ? represents unclear.
Meta-analysis results
In the included studies, the logarithms of the sensitivity and 1-specificity were analyzed by Spearman’s correlation. With the diagnostic test interpreted in series and parallel, the correlation coefficients were 0.202 and 0.157, respectively, indicating no obvious threshold effect. The SROC curves were displayed in Figure 3 (A, B). The relevant indicators of the diagnostic value of the combination method versus RF or anti-CCP alone in RA were shown in Table 2. The data of 8 parallel studies were tested for heterogeneity, and the DOR (P < 0.05, I2 = 100.00%), sensitivity (P < 0.05, I2 = 92.00%), specificity (P < 0.05, I2 = 86.88%), +LR (P < 0.05, I2 = 75.27%), and −LR (P < 0.05, I2 = 91.59%) were all heterogeneous. A bivariate mixed-effects model was applied for data merging. The results indicated that the pooled sensitivity = 0.87 [95% confidence interval (CI): 0.80–0.92], specificity = 0.76 (95%CI: 0.67–0.84) (Figure 4A), +LR = 3.68 (95%CI: 2.62–5.176), −LR = 0.17 (95%CI: 0.11–0.26), DOR = 21.56 (95%CI: 11.63–39.99), and AUC = 0.89 (95%CI: 0.86–0.91). Moreover, Deek’s funnel plot showed P>0.05, indicating no significant publication bias (Figure 5A). Subgroup analysis and meta-regression showed that region, number of patients with RA, and published language might be the main sources of heterogeneity (Figure 6A).

SROC curve for the accuracy of combined detection with anti-CCP and RF in the diagnosis of rheumatoid arthritis. A: “anti-CCP OR RF”; B: “anti-CCP AND RF”.
Diagnostic value of two methods for rheumatoid arthritis.
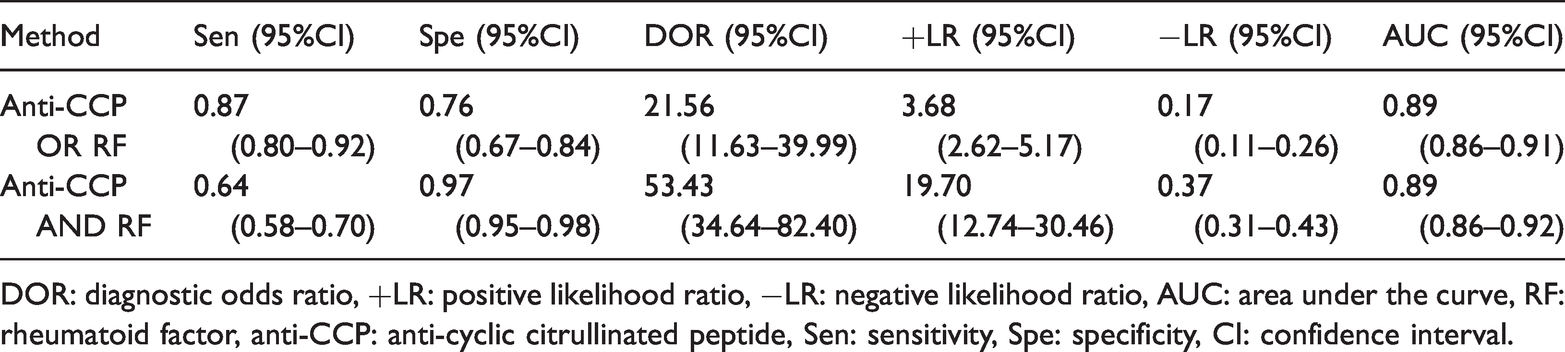
DOR: diagnostic odds ratio, +LR: positive likelihood ratio, −LR: negative likelihood ratio, AUC: area under the curve, RF: rheumatoid factor, anti-CCP: anti-cyclic citrullinated peptide, Sen: sensitivity, Spe: specificity, CI: confidence interval.
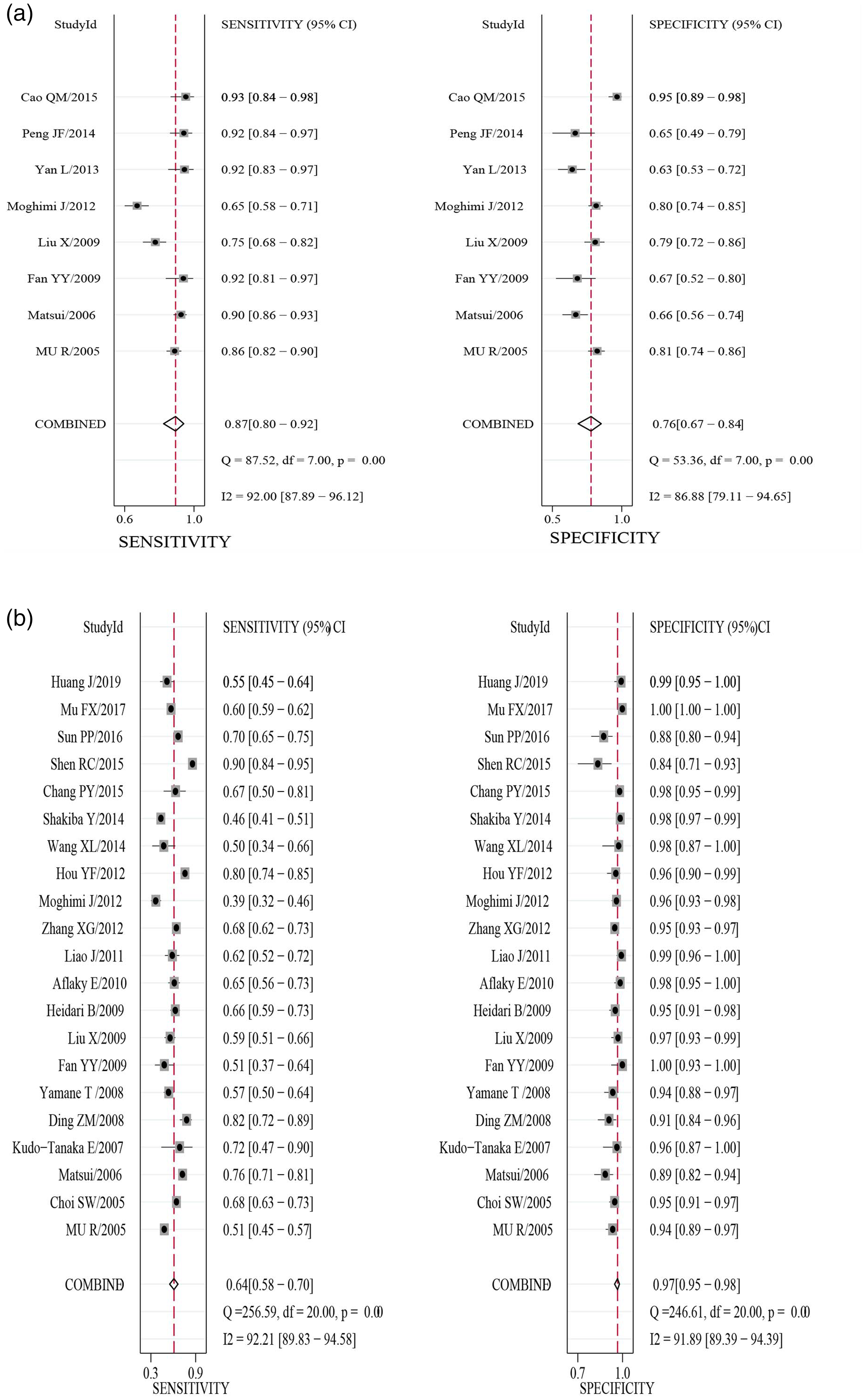
Sensitivity and specificity of combined detection with anti-CCP and RF for the diagnosis of rheumatoid arthritis. A: “anti-CCP OR RF”; B: “anti-CCP AND RF”.

Deeks’ funnel plot of combined detection with anti-CCP and RF for the diagnosis of rheumatoid arthritis. A: “anti-CCP OR RF”, B: “anti-CCP AND RF”.

Univariable meta-regression and subgroup analyses. A: “anti-CCP OR RF”; B: “anti-CCP AND RF”. *P<0.05, **P<0.01, ***P<0.001.
The data of 21 serial studies were tested for heterogeneity, and the DOR (P < 0.05, I2 = 100.00%), sensitivity (P < 0.05, I2 = 92.21%), specificity (P < 0.05, I2 = 91.89%), +LR (P < 0.05, I2 = 85.23%), and −LR (P < 0.05, I2 = 91.85%) were all heterogeneous. A bivariate mixed-effects model used for data merging. The results indicated that the pooled sensitivity = 0.64 (95%CI: 0.58–0.70), specificity = 0.97 (95%CI: 0.95–0.98) (Figure 4B), +LR = 19.70 (95%CI: 12.74–30.46), −LR = 0.37 (95%CI: 0.31–0.31), DOR = 53.43 (95%CI: 34.46–82.40), and AUC = 0.89 (95%CI: 0.86–0.92). Furthermore, Deek’s funnel plot showed P < 0.05, indicating obvious publication bias (Figure 5B). Subgroup analysis and meta-regression showed that publication year, region, number of participants with RA, and publication language might be the main sources of heterogeneity (Figure 6B). Together, these data suggest that the combined detection of RF and anti-CCP had a good diagnostic performance for RA in the Asian population.
Sensitivity analysis
To verify the robustness of the conclusion, we carried out a sensitivity analysis. Goodness-of-fit (Figure 7A, 8A) and bivariate normal distribution (Figure 7B, 8B) suggested that the bivariate mixed-effects model for this meta-analysis was robust. In the parallel analysis, influence evaluation (Figure 7C) and outlier detection (Figure 7D) found one study 42 that might impact the conclusions. After excluding this study, the AUC, sensitivity, and specificity were 0.84, 0.86, and 0.73, respectively. In the series analysis, influence evaluation (Figure 8D) and outlier detection (Figure 8D) found three studies43–45 that might influence the robustness of the conclusions. After omitting the three studies, the AUC, sensitivity, and specificity were 0.90, 0.64, and 0.96, respectively. Therefore, the results were not significantly changed after excluding outliers, indicating that the findings of our meta-analysis are robust.

Sensitivity analysis of anti-CCP and RF in the parallel diagnosis of rheumatoid arthritis. (a) Goodness-of-fit; (b) Bivariate normality; (c) Influence analysis; (d) Outlier detection.

Sensitivity analysis of anti-CCP and RF in the tandem diagnosis of rheumatoid arthritis. (a) Goodness-of-fit; (b) Bivariate normality; (c) Influence analysis; d: Outlier detection.
Discussion
RA is a chronic systemic inflammatory disease. Recent studies found that ant-CCP and RF are important for the diagnosis and monitoring of RA. The positive rate of RF in early RA is approximately 40% to 60%, and RF may appear before the disease in some patients. Additionally, the specificity of RF is poor. Bas et al. 46 reported that anti-CCP levels are significantly related to bone erosion in patients with RA. Anti-CCP is a specific indicator for the early prediction, identification, and diagnosis of RA and a good indicator of bone destruction in patients with RA. Syversen et al. 47 selected 99 cases with a disease course of <1 year who did not receive disease-modifying anti-rheumatic drugs, and the results suggested that changes in anti-CCP titers predicted the progression of joint destruction. In 2009, the American College of Rheumatology/European League Against Rheumatism jointly proposed new diagnostic criteria for RA, establishing the important position of anti-CCP in the diagnosis of RA. 48
Following strict selection criteria, 24 published articles were included in our meta-analysis. According to the QUADAS-2, all included studies were of high quality, and only a certain high-risk bias existed in two evaluation items for all patients included in the analysis. The results indicated that in patients with both RF and anti-CCP positivity (21 studies included), the sensitivity for the diagnosis of RA was 0.64, which was lower than that of RF (0.71) and anti-CCP (0.67). 49 These findings suggest that 64% of Asian patients with RA were diagnosed, with a missed diagnosis rate as high as 36%. The positive predictive value was 19.70, which was considerably higher than RF (3.96) and anti-CCP (9.8) individual tests, 49 indicating that when RF and anti-CCP were both positive, the subjects were highly likely to suffer from RA. Moreover, the specificity of the combined detection of RF and anti-CCP was 0.97, indicating that 97% of patients without RA were excluded by the test, with a misdiagnosis rate of 3%. As the specificity of diagnosing RA by anti-CCP alone was as high as 94%, 49 the combined detection of RF and anti-CCP and anti-CCP alone achieved the same efficacy in correctly rejecting healthy patients without RA. The combined detection of RF and anti-CCP for RA showed an AUC of 0.89 and DOR of 53.43, indicating that the combined detection of RF and anti-CCP had a good diagnostic value for RA. Sensitivity analysis verified the robustness of the conclusions.
When either RF or anti-CCP was positive, the diagnostic sensitivity of RA was 0.87, which was significantly higher than that of RF (0.71) and anti-CCP (0.67) individual tests. 49 However, the specificity decreased to only 0.76, indicating that 24% of patients without RA might be misdiagnosed with RA. Therefore, when only RF or anti-CCP is positive, other diagnostic indicators should be used to prevent misdiagnosis. The negative predictive value was 0.17, which was lower than RF (0.37) and anti-CCP (0.35) tested separately. 49 When both RF and anti-CCP were negative, the subjects did not likely have RA. No significant publication bias was found in the parallel analysis. Sensitivity analysis verified the robustness of the conclusions. The area under the ROC curve (0.89) and DOR (21.56) were significantly different, indicating that the combination of RF and anti-CCP had a good diagnostic performance for RA in the Asian population.
We conducted a subgroup analysis and meta-regression to explore the sources of the heterogeneity across the studies included. The results showed that the region, sample size, and published language had a significant influence on the heterogeneity in both parallel and series analyses. The impact of region on patients with RA might be due to ethnic differences. The effect of sample size on diagnostic performance might be caused by statistical efficiency. The heterogeneity caused by published language might be associated with differences in the quality of studies published in English compared with those published in Chinese.
This study also had several limitations: 1) The sample size included in this study was limited, which might have a certain impact on the robustness of the conclusion. 2) Because only English and Chinese studies were included, some high-quality literature in other languages might have been missed, which may cause publication bias. 3) Publication bias existed in the series analysis. 4) In the included literature, the diagnostic threshold was inconsistent, which might affect the consistency among studies.
In conclusion, the combined detection of RF and anti-CCP improved the diagnostic efficiency of RA in Asia. Additionally, RF and anti-CCP detection increased the ability to distinguish between true-positive and true-negative cases. Different combined methods may be used in clinical applications based on the diagnostic requirements. This analysis is the first to comprehensively analyze the diagnostic value of the combined detection of RF and anti-CCP in Asian patients with RA, which has a crucial clinical significance. Owing to the limitations of this study, more clinical trials and data are needed to further verify the above conclusions.
Footnotes
Author contributions
XY designed the study, conducted the analysis, and drafted the manuscript. YC participated in the study design and critically reviewed the manuscript. BX participated in the study design, participated in the analysis, and critically reviewed the manuscript. XY, YC, BX, and BZ contributed to patient recruitment and critically reviewed the manuscript. All authors contributed substantially to the work, revised the manuscript critically, approved the submitted version, and agree to be accountable for all aspects of the work.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.