
Abstract
Objective
Peritoneal injury is a common complication during totally extraperitoneal inguinal hernia repair, potentially affecting surgical outcomes and patient recovery. Identifying risk factors associated with peritoneal injury is crucial to improving surgical techniques and optimizing patient care.
Methods
This retrospective study analyzed data from 334 patients who underwent totally extraperitoneal inguinal hernia repair between August 2019 and April 2024. Patients were divided into two groups based on the occurrence of peritoneal injury: injury group (n = 69) and noninjury group (n = 265). Univariate and multivariate logistic regression analyses identified independent risk factors for peritoneal injury. A predictive nomogram was constructed using significant variables from the multivariate analysis. The performance of the nomogram was evaluated using the area under the receiver operating characteristic curve (AUC), calibration plots, and decision curve analysis.
Results
Peritoneal injury occurred in 20.7% of the cases. Multivariate analysis identified the following five independent risk factors: anatomical misrecognition (odds ratio: 7.55; p = 0.005), insufficient peritoneal tension (odds ratio: 2.95; p = 0.007), hernial sac diameter ≥4 cm (odds ratio: 2.75; p = 0.008), prior infraumbilical surgery (odds ratio: 2.50; p = 0.021), and use of sharp medial hernia sac dissection techniques (odds ratio: 5.20; p = 0.006). Body mass index was a significant factor in univariate analysis (p = 0.004) but not in multivariate analysis (p = 0.180). The nomogram demonstrated good discriminative ability (AUC = 0.841) and calibration. The decision curve analysis indicated that the nomogram provided clinical utility across a range of threshold probabilities.
Conclusions
The study identified key risk factors for peritoneal injury during totally extraperitoneal inguinal hernia repair and developed a predictive nomogram with strong discriminative ability. Awareness of these factors enables surgeons to preoperatively stratify risk based on imaging-assessed hernia characteristics and patient history, thereby guiding technique selection.
Introduction
Inguinal hernia is one of the most common conditions in the field of surgery, significantly affecting patients’ quality of life. 1 With the rapid advancement of minimally invasive surgical techniques, totally extraperitoneal (TEP) is a widely adopted minimally invasive approach for inguinal hernia repair, offering advantages such as reduced postoperative pain, although its complication profile varies with surgeon expertise and patient factors. 2
However, peritoneal injury during TEP remains one of the major challenges faced by surgeons. 3 Peritoneal injury can lead to limited surgical visualization and loss of pneumoperitoneum, thereby prolonging operative time and increasing the risk of intraoperative conversion to transabdominal or open surgery. 4 Peritoneal injury and its associated sequelae not only prolong the patient’s hospital stay but may also increase the risk of postoperative infections, thereby adversely affecting patient outcomes. 5
Currently, the prevention of peritoneal injury relies mainly on the surgeon’s experience and surgical skills, as no effective risk prediction tool exists to assist clinical decision-making. Establishing a model that can accurately predict the risk of peritoneal injury preoperatively is of great significance for formulating individualized surgical plans and reducing surgical complications.
The predictive nomogram primarily incorporates factors that can be assessed before surgery or reliably anticipated based on clinical and imaging findings. Although certain factors are ultimately confirmed intraoperatively, their risk can be screened during preoperative planning, which can contribute to patient counseling and surgical decision-making prior to skin incision.
This study aimed to construct a nomogram to estimate the risk of peritoneal injury, primarily based on factors available or anticipated before surgery through clinical history and imaging. The model is intended to serve as a preoperative risk stratification tool for guiding surgical planning and patient counseling.
Materials and methods
Patients
This retrospective study included patients who underwent TEP inguinal hernia repair at our hospital between August 2019 and April 2024. The inclusion criteria were as follows: (a) patients diagnosed with unilateral or bilateral inguinal hernia; (b) aged ≥18 years; (c) underwent primary TEP performed by experienced surgeons; and (d) had complete clinical and operative data available. The exclusion criteria included the following: (a) conversion to transabdominal preperitoneal (TAPP) repair or open hernia surgery; (b) recurrent hernias requiring alternative surgical approaches; (c) severe comorbidities contraindicating laparoscopic surgery; and (d) incomplete medical records.
A total of 334 patients met the inclusion criteria and were enrolled in the study. Among them, 265 patients did not experience peritoneal injury during surgery, while 69 patients did. The study was approved by the institutional review board of our hospital, and the requirement for informed consent was waived due to the retrospective nature of the study. The reporting of this study conforms to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines. 6 The study was conducted in accordance with the principles of the 1975 Declaration of Helsinki, as revised in 2024.
Data collection
Clinical, laboratory, and surgical data were retrospectively collected from the hospital’s electronic medical records and operative reports for all patients included in the study. Demographic and clinical characteristics recorded for each patient comprised age, sex, body mass index (BMI), American Society of Anesthesiologists (ASA) physical status classification, comorbidities such as hypertension and diabetes, and history of alcohol consumption.
Preoperative laboratory tests were reviewed, including white blood cell count, preoperative hemoglobin levels, and preoperative albumin levels, to assess baseline hematological and nutritional status. These parameters provided insights into the patients’ general health condition prior to surgery.
Detailed surgical information was extracted from operative reports. Instances of anatomical misrecognition were documented, defined as any confusion or errors in identifying anatomical structures during the procedure. The hernia site was recorded and classified as left, right, or bilateral. Cases of insufficient peritoneal tension were identified, referring to situations where the peritoneum lacked adequate tension during surgery, potentially increasing the risk of injury. The hernial sac diameter was measured intraoperatively and categorized as <4 or ≥4 cm, as larger sacs may pose a higher risk for peritoneal injury. Operation time, defined as the duration of surgery in minutes, was documented for each patient. Information on prior infraumbilical surgery was collected, including any history of surgeries below the umbilicus such as appendectomy (open or laparoscopic), prostate surgery, rectal surgery (open or laparoscopic), uterine and adnexal surgery, and other surgeries. Additionally, the use of sharp medial hernia sac dissection techniques on the medial aspect of the hernia sac was recorded, as this may impact the likelihood of peritoneal injury.
The primary outcome measured was the occurrence of peritoneal injury during TEP. Peritoneal injury was defined as any unintended breach or tear of the peritoneum documented intraoperatively by the surgeon. Data on peritoneal injuries were extracted from operative reports and surgical logs to ensure accuracy.
All collected data were anonymized to ensure patient confidentiality and were entered into a secure database for analysis. Quality checks were performed by independent reviewers to verify the accuracy and completeness of the data. This comprehensive data collection allowed for a thorough analysis of potential risk factors associated with peritoneal injury during TEP.
Statistical analysis
Statistical analyses were conducted using GraphPad Prism version 8.0 (GraphPad Inc., CA, USA) and IBM SPSS Statistics version 23.0 (IBM Corp., Armonk, NY, USA). The results were reported as mean ±standard deviation or in terms of counts and percentages (n, %). Depending on the nature of the data, appropriate statistical tests such as the chi-square test, Student t-test, or Mann–Whitney U test were used. Risk factors were examined through binary univariate and multivariate logistic regression analyses using the “Enter” method. A nomogram incorporating the identified risk factors was developed and assessed via R software (version 4.0.1) using the ‘rms’ package. Receiver operating characteristic (ROC) curve analysis was performed to evaluate the predictive ability of the nomogram for peritoneal injury. Statistical significance was determined at a p-value less than 0.05.
Results
Patient characteristics
A total of 334 patients who underwent TEP inguinal hernia repair were included in the study. Of these, 69 (20.7%) experienced peritoneal injury during the procedure, while 265 (79.3%) did not. The mean age was comparable between the two groups (no peritoneal injury: 46.0 ± 13.0 years; peritoneal injury: 48.5 ± 14.2 years; p = 0.172). There were no significant differences in sex distribution, ASA physical status classification, or comorbidities such as hypertension and diabetes (p > 0.05). However, patients who experienced peritoneal injury had a significantly higher BMI than those who did not (25.0 ± 3.2 vs. 23.3 ± 2.7 kg/m2; p = 0.004).
Univariate analysis of risk factors
Univariate logistic regression analysis revealed that several factors were significantly associated with the occurrence of peritoneal injury during TEP (Table 1, Figure 1). A higher BMI was linked to an elevated risk of peritoneal injury (p = 0.004). The presence of anatomical misrecognition during the procedure significantly increased the likelihood of peritoneal injury (p = 0.002). Patients with insufficient peritoneal tension had a higher incidence of peritoneal injury than those without (p = 0.019). Additionally, hernial sacs with a diameter of ≥4 cm were more frequently associated with peritoneal injury than smaller sacs (p = 0.007). A history of infraumbilical surgery was also identified as a significant factor (p = 0.031). The use of sharp medial hernia sac dissection techniques was correlated with an increased risk of peritoneal injury (p = 0.012).
Univariate logistic regression analysis of the risk factors for peritoneal injury.
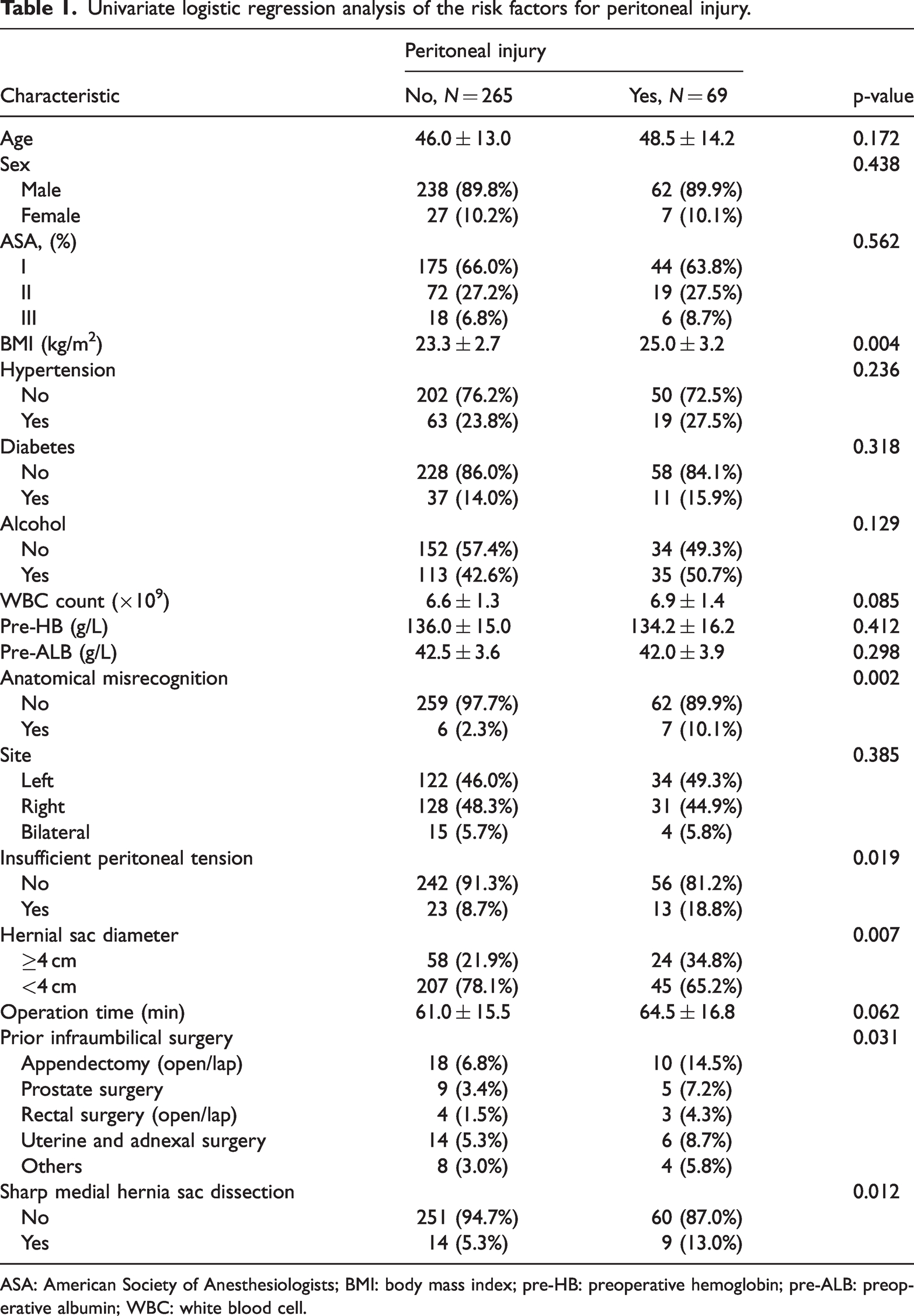
ASA: American Society of Anesthesiologists; BMI: body mass index; pre-HB: preoperative hemoglobin; pre-ALB: preoperative albumin; WBC: white blood cell.
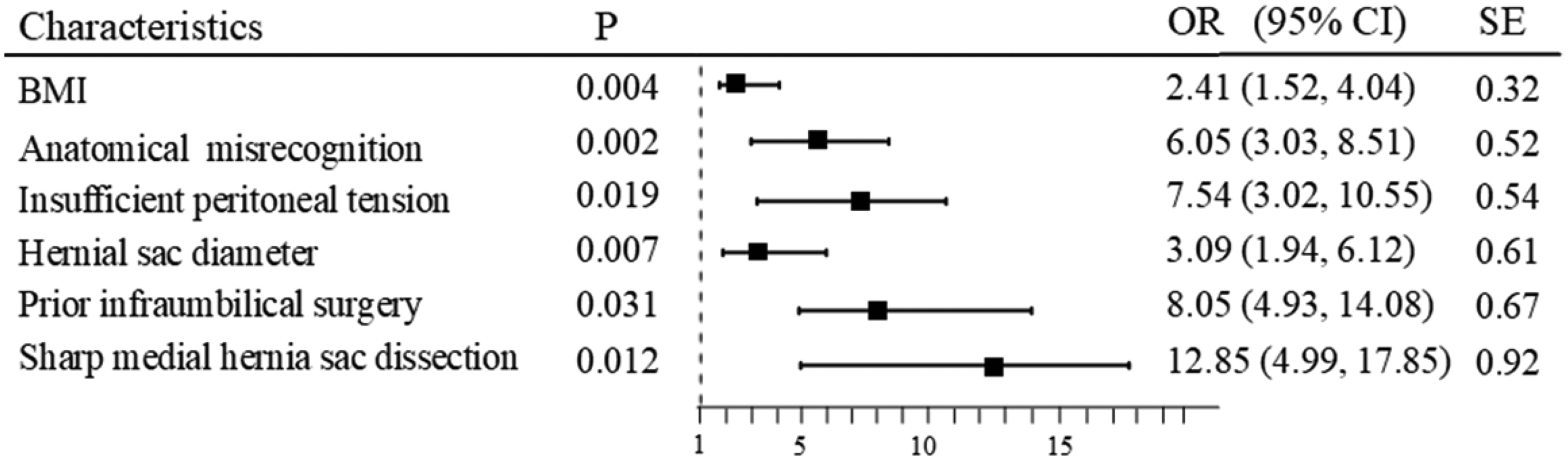
A forest plot of univariate logistic regression analysis for peritoneal injury.
Multivariate analysis of risk factors
Multivariate logistic regression analysis identified independent risk factors for peritoneal injury during TEP (Table 2, Figure 2). Anatomical misrecognition emerged as a significant independent predictor, with an odds ratio (OR) of 7.55 (95% confidence interval (CI): 1.50–9.88; p = 0.005). Insufficient peritoneal tension remained significantly associated with peritoneal injury (OR: 2.95; 95% CI: 1.35–6.45; p = 0.007). Patients with a hernial sac diameter of ≥4 cm showed a higher risk of peritoneal injury (OR: 2.75; 95% CI: 1.30–5.80; p = 0.008). A history of infraumbilical surgery was independently associated with an increased risk of peritoneal injury (OR: 2.50; 95% CI: 1.15–5.40; p = 0.021). The use of sharp medial hernia sac dissection techniques significantly elevated the risk of peritoneal injury (OR: 5.20; 95% CI: 2.40–12.50; p = 0.006). In contrast, BMI did not remain a significant independent risk factor in the multivariate model (p = 0.180).
Multivariate logistic regression analysis of the risk factors for peritoneal injury.

BMI: body mass index; CI: confidence interval; OR: odds ratio.

A forest plot of multivariate logistic regression analysis for peritoneal injury.
Development of the nomogram
Based on the significant independent risk factors identified, a nomogram was constructed to predict the risk of peritoneal injury during TEP (Figure 3). The nomogram incorporated factors such as anatomical misrecognition, insufficient peritoneal tension, hernial sac diameter ≥4 cm, prior infraumbilical surgery, and the use of sharp medial hernia sac dissection techniques. Each risk factor was assigned a score proportional to its regression coefficient from the multivariate analysis.

Nomogram for predicting the risk of peritoneal injury during totally extraperitoneal inguinal hernia repair.
Validation of the nomogram
The predictive performance of the nomogram was evaluated using ROC curve analysis, calibration plot, and decision curve analysis (DCA). The area under the ROC curve (AUC) was 0.841, indicating good discriminative ability of the nomogram (Figure 4). The calibration plot demonstrated good agreement between the predicted probabilities and actual observed outcomes, suggesting that the nomogram is well-calibrated (Figure 5). The DCA showed that the nomogram provided a net clinical benefit across a range of threshold probabilities, indicating its potential utility in clinical decision-making (Figure 6).

Receiver operating characteristic (ROC) curve for the nomogram.

Calibration plot for the nomogram.
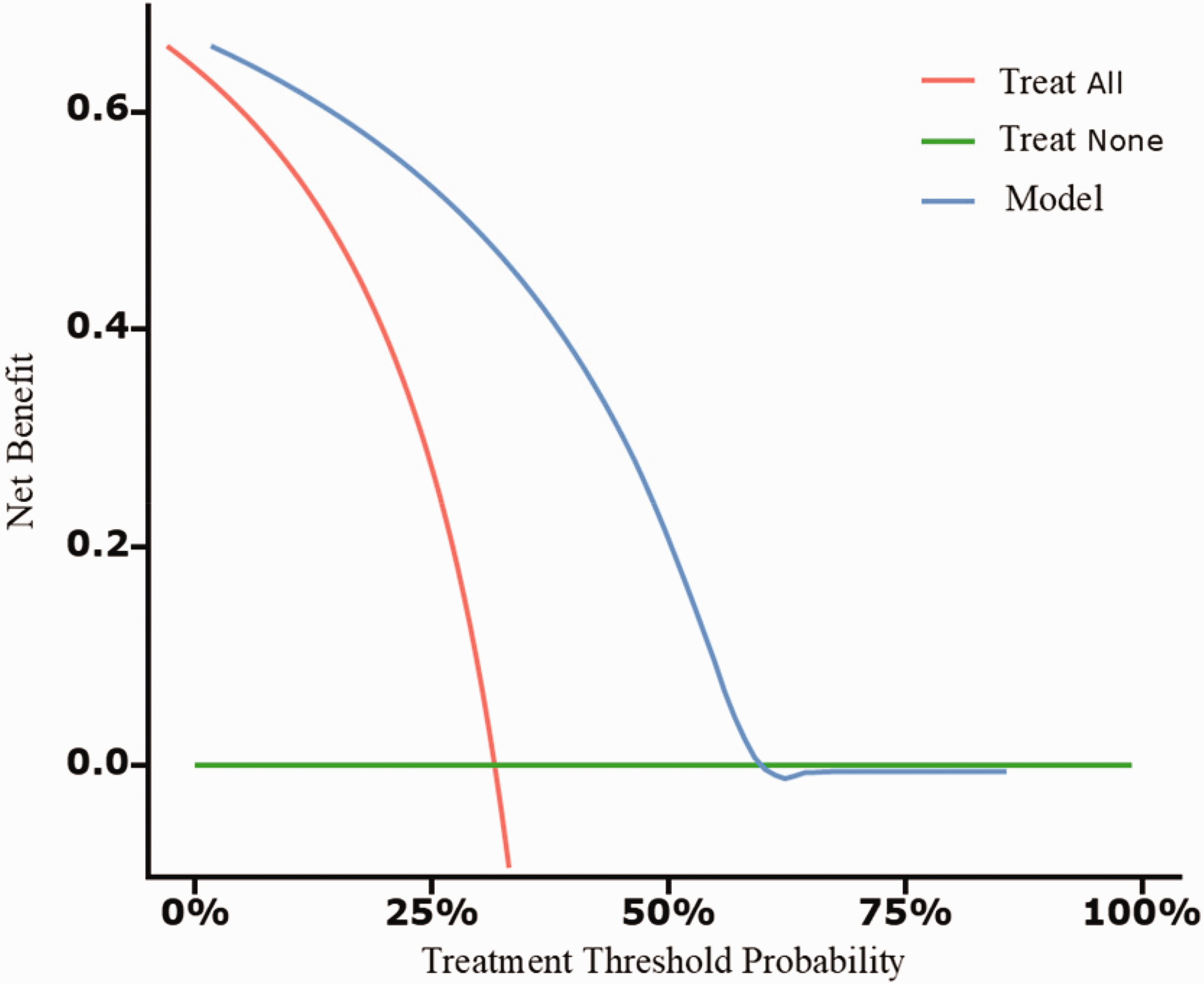
Decision curve analysis (DCA) for the nomogram.
Discussion
This study aimed to identify independent risk factors for peritoneal injury during TEP inguinal hernia repair and develop a predictive nomogram based on these factors. The findings provide valuable insights into the factors that contribute to peritoneal injury, a common complication that can adversely affect surgical outcomes and patient recovery. Peritoneal injury during TEP presents significant challenges, such as loss of the preperitoneal working space, prolonged operative time, and potential conversion to TAPP repair or open surgery. The incidence of peritoneal injury in our study was 20.7%, which aligns with previously reported rates ranging from 10% to 30% in laparoscopic hernia repairs. 7 Understanding the risk factors associated with peritoneal injury is crucial for improving surgical techniques and patient outcomes.
Anatomical misrecognition emerged as the most significant independent risk factor for peritoneal injury (OR: 7.55, p = 0.005). This underscores the importance of surgeon expertise and familiarity with the intricate anatomy of the inguinal region. In TEP procedures, the preperitoneal space is accessed and navigated without breaching the peritoneum. Misidentification of anatomical landmarks can lead to inadvertent peritoneal tears. Existing literature emphasizes that the learning curve for TEP is steep, and surgeon proficiency significantly impacts complication rates.8,9 Continuous training, simulation-based education, and mentorship programs can enhance anatomical recognition skills, potentially reducing the incidence of peritoneal injury.
Insufficient peritoneal tension was independently associated with peritoneal injury (OR: 2.95, p = 0.007). Adequate tension in the peritoneum facilitates safe dissection by providing a clear operative field and minimizing unintended contact with the peritoneum. Factors contributing to insufficient tension may include technical aspects such as suboptimal pneumoperitoneum pressure or patient-related factors (e.g. tissue laxity). 10 Surgeons should ensure optimal insufflation pressures and consider patient positioning strategies that enhance peritoneal tension. Employing traction and countertraction techniques can also help maintain appropriate tension during dissection.
A hernial sac diameter of ≥4 cm was a significant risk factor (OR: 2.75, p = 0.008), indicating that larger hernias pose greater challenges during TEP. We hypothesize that a large hernia sac can constrict the operative workspace, thereby increasing the risk of injury. Moreover, when the hernia sac is substantial in size, the peritoneum is naturally thinner and weaker, increasing the risk of injury. 11 Large hernial sacs may involve extensive adhesions and require more meticulous dissection, increasing the risk of peritoneal breach. 12 This finding corroborates those of previous studies that reported higher complication rates in patients with large or scrotal hernias undergoing laparoscopic repair.13,14 Preoperative imaging, such as ultrasound or magnetic resonance imaging, can assist in assessing hernia size and complexity. In cases of large hernias, surgeons might consider alternative approaches, such as TAPP repair, which may provide better visualization and access for safe dissection.
Prior infraumbilical surgery was identified as an independent risk factor (OR: 2.50, p = 0.021). Previous surgeries can lead to fibrosis and altered anatomical planes, making dissection more challenging and increasing the risk of peritoneal injury. Consistent with existing literature, patients with a history of lower abdominal surgeries exhibit higher complication rates in laparoscopic hernia repairs due to adhesions and scar tissue.7,15,16 Preoperative planning should include a thorough surgical history and, if necessary, imaging studies to evaluate the extent of adhesions. In some instances, open repair may be more appropriate to manage the complexities presented by prior surgeries.
The use of sharp medial hernia sac dissection techniques significantly increased the risk of peritoneal injury (OR: 5.20, p = 0.006). Sharp dissection, although precise, can inadvertently damage adjacent tissues, especially in areas with obscured anatomical landmarks. Blunt dissection methods are generally preferred in TEP procedures to minimize tissue trauma. The medial aspect of the hernia sac tends to be closely attached to underlying structures such as the vas deferens. 17 Consequently, performing dissection on this adherent membrane, particularly using sharp techniques, could contribute to the risk of peritoneal injury. Surgeons should evaluate the necessity of sharp dissection on a case-by-case basis and employ it judiciously. Training programs that emphasize safe dissection techniques and the development of advanced laparoscopic skills can mitigate this risk.
Although BMI was a significant factor in univariate analysis, it did not remain significant in the multivariate model (p = 0.180). This suggests that although higher BMI may be associated with increased technical difficulty during TEP, it is not an independent predictor of peritoneal injury when other factors are considered. Obesity can present challenges such as limited workspace and reduced visibility.18–20 However, adherence to meticulous surgical technique can offset these difficulties. 21 Further research may explore the interplay between BMI and other patient-specific factors influencing surgical outcomes.
The nomogram developed in this study integrates the identified independent risk factors to predict the likelihood of peritoneal injury during TEP. The nomogram demonstrates good discriminative ability, with an AUC of 0.841. It serves as a valuable tool for preoperative risk stratification, enabling surgeons to identify high-risk patients and tailor surgical strategies accordingly. For instance, in patients with a high predicted risk, surgeons may opt for alternative surgical approaches, allocate additional resources, or prepare for potential intraoperative challenges.
Implementing the nomogram in clinical practice can enhance patient counseling by providing individualized risk assessments. This facilitates shared decision-making, where patients are informed of potential risks and the rationale behind selected surgical strategies. Moreover, the nomogram can aid in surgical training programs by highlighting critical risk factors and emphasizing areas where surgical technique and decision-making can be improved.
The strengths of this study include a sizeable patient cohort and the use of multivariate logistic regression to adjust for potential confounders. The comprehensive data collection allowed for a thorough analysis of relevant clinical and operative variables. However, limitations must be acknowledged. The retrospective design introduces the possibility of selection bias and limits causal inference. As this is a single-center study, the findings may not be generalizable to all practice settings. Additionally, unmeasured variables, such as the surgeon’s level of experience and intraoperative decision-making skill, were not accounted for, although they may influence the risk of peritoneal injury.
Future research should focus on validating the nomogram in multicenter, prospective studies to enhance its generalizability. Incorporating additional variables, such as surgeon experience and intraoperative technical adjustments, may refine the predictive accuracy of the model. Exploring interventions aimed at mitigating identified risk factors, such as enhanced training programs targeting anatomical recognition and safe dissection techniques, could further reduce the incidence of peritoneal injury. Additionally, integrating technological advancements such as augmented reality or robotic assistance may aid in overcoming anatomical challenges associated with TEP.
Conclusion
In summary, this nomogram highlights intraoperative factors associated with peritoneal injury during TEP inguinal hernia repair. Although most predictor variables are not reliably accessible before surgery, the model can serve as a practical intraoperative guide to heighten surgeon awareness. Its preoperative use in patient counseling and shared decision-making is limited, and further research with prospective data on preoperative predictors is needed. Recognizing and addressing these risk factors can lead to improved surgical planning and patient outcomes. By incorporating the nomogram into clinical practice, surgeons can enhance preoperative risk assessment, tailor surgical techniques, and potentially reduce the incidence of peritoneal injury. Ultimately, this approach contributes to the advancement of minimally invasive hernia repair and the optimization of patient care.
Footnotes
Acknowledgments
The authors thank the medical staff of our hospital for database management. No artificial intelligence (AI) tools or AI-assisted technologies were used in the design, data analysis, or writing of this study.
Author contributions
Jingbin Wang drafted the manuscript and performed the literature review. Yuanfang Sun performed the procedures. Yanhao Sun collected and analyzed the data. All authors read and approved the final manuscript.
Data availability statement
The datasets used or analyzed during the current study are available from the corresponding author on reasonable request.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.