
Abstract
Objective
A randomized, double-blind, prospective, controlled study to determine the lowest concentration of lidocaine that provides satisfactory anaesthesia and analgesia for inguinal hernia repair.
Methods
Patients with inguinal hernia undergoing tension-free mesh repair under local infiltration anaesthesia were randomized to receive 0.25% (Group A), 0.33% (Group B) or 0.5% (Group C) lidocaine. Total dose and volume of lidocaine consumed and intraoperative visual analogue scale (VAS) pain scores were recorded for each patient. Each patient’s degree of satisfaction and the incidence of anaesthesia- and procedure-related complications were recorded and assessed.
Results
A total of 120 patients were randomized. There were no between-group differences in median VAS scores, degree of satisfaction, volume of lidocaine consumed or incidence of complications. Patients in group A consumed significantly lower doses of lidocaine than those in both other groups.
Conclusions
The mean dose of lidocaine consumed in group A was significantly lower but exerted similar efficacy to that in the other groups, and may lead to a lower risk of local anaesthetic toxicity.
Introduction
General, spinal (subarachnoid and epidural) and local anaesthesia are widely used in inguinal hernia repair.1,2 Local anaesthesia is preferred to other methods due to its better safety profile, shorter recovery time, reduced urinary morbidity and lower overall cost.3–5 The local anaesthetic lidocaine has a rapid onset, high dose limitation and moderate duration of action.6–8 The concentration of lidocaine used for hernia repair ranges between 0.5% and 2%,3,7,9,10 but lidocaine toxicity increases as its concentration rises7,11,12 and when used in combination with other anaesthetics or epinephrine.13,14 In our experience, a lidocaine concentration of <0.5% provides satisfactory anaesthetic effect in hernia repair without the use of other anaesthetics or epinephrine. The aim of this randomized, double-blind, prospective, controlled study was to evaluate the efficacy of three different lidocaine concentrations (0.25%, 0.33% and 0.5%) for tension-free inguinal hernia repair under local infiltration anaesthesia, in order to determine the lowest concentration of lidocaine that provides satisfactory anaesthesia and pain relief.
Patients and methods
Study population
The study recruited adults with unilateral, primary and reducible inguinal hernias, undergoing tension-free mesh hernia repair under local infiltration anaesthesia at the Hernia Centre of West China Hospital of Sichuan University, Chengdu, China, between October 2011 and December 2011. Patients who were allergic to lidocaine or who had psychiatric or neuralgic diseases were excluded from the trial. Age, sex, disease course, American Society of Anesthesiologists (ASA) classification, 15 side of hernia, Gilbert classification of hernia type, 16 and body mass index (BMI) were recorded for each patient.
The study was approved by the Research Ethics Committee of West China Hospital of Sichuan University and was conducted in accordance with the Declaration of Helsinki. All patients provided written informed consent.
Study design and data collection
Patients were randomly divided into one of three groups, using a computer-generated randomized sequence, to receive one of: 0.25% lidocaine (group A); 0.33% lidocaine (group B); or 0.5% lidocaine (group C). A visual analogue pain scale (VAS) was demonstrated to patients before surgery, with 0 cm representing no pain and 10 cm representing unbearable pain. Each patient provided VAS scores at skin incision, 10 min after the beginning of surgery and at the end of the surgery. At the end of surgery, each patient and surgeon evaluated the anaesthesia and surgical procedure as ‘very good’, ‘acceptable’ or ‘unacceptable’. Electrocardiogram, noninvasive blood pressure, oxygen saturation via pulse oximetry and respiration were monitored throughout surgery. Lidocaine-associated cardiovascular adverse effects and central nervous system toxicity were evaluated according to vital and clinical signs.
Surgical and anaesthetic procedure
No sedation or analgesia was used as premedication before surgery. Anaesthetic solutions were prepared by a scrub nurse just before surgery and comprised 2% simple lidocaine and normal saline (without any other agents) to a total volume of 200 ml, with the final lidocaine concentration determined according to group allocation. All surgical procedures were performed by a single experienced surgeon (W-Z. L.) who was blinded to the lidocaine concentration. Stepwise infiltration anaesthesia3,10 was performed using a 10-ml syringe and a 22-gauge needle, with 10 ml injected subcutaneously from the pubic tubercle to 1 cm above the middle of the inguinal ligament (the internal inguinal ring), 5 ml injected to the intradermal, 10 ml to the inguinal canal, and 5 ml to the pubic tubercle. A further 10 ml was injected to the internal inguinal ring, with the needle withdrawn to prevent injection of anaesthetic into blood vessels. Skin incision was performed, the subcutaneous fascia was opened to expose the external oblique aponeurosis and 10 ml of anaesthetic solution was injected into the subaponeurosis. Next, the external oblique aponeurosis was opened, the spermatic cord was mobilized (as appropriate), and 5–10 ml of solution was injected around the internal inguinal ring (indirect hernia) or underneath the transverse fascia (direct hernia). Additional anaesthetic could be applied at any time, according to the patient’s needs and the requirements of the procedure.
All repairs were made using the Ultrapro™ Hernia System (UHS) (Ethicon, Norderstedt, Germany), with placement of materials undertaken using the Prolene™ Hernia System (PHS).10,17 The ilio-inguinal, iliohypogastric and genital branches of the genitofemoral nerve were preserved if they were encountered during the operation.
The dose and volume of lidocaine used were carefully measured and recorded by the scrub nurse. The numbers of patients converted to general or spinal anaesthesia, those requiring sedation or analgesia and the type and dose of drugs used were also recorded. The duration of surgery, and any anaesthesia- and procedure-related complications, were recorded and assessed. Patients were under no restrictions regarding movement or diet, and the majority were discharged from hospital the following day. All of the observations and records were implemented by students who were specially trained to take part in the study.
Statistical analyses
Continuous variables were presented as mean ± SD or median (range); categorical variables were presented as n (%). One-way analysis of variance or the Kruskal–Wallis test were used to analyse continuous variables. The numbers of patients with anaesthesia- or procedure-related complications were analysed using contingency table analysis and Fisher's exact test. Multiple comparisons were made using least significant difference or Nemenyi tests. Pearson’s correlation coefficient was used to determine correlations between lidocaLine dose and volume, and BMI. Statistical analyses were performed using SPSS® software, version 19.0 (SPSS Inc, Chicago, IL, USA) for Windows®. All comparisons were two-tailed and a P-value <0.05 was considered statistically significant.
Results
Demographic and clinical characteristics of adults with unilateral, primary or reducible inguinal hernias, undergoing tension-free mesh hernia repair under local infiltration anaesthesia, who were enrolled in a study to compare the effects of 0.25% (group A), 0.33% (group B) or 0.5% (group C) lidocaine (n = 120.

Data presented as mean ± SD or median (range).
BMI, body mass index; ASA, American Society of Anesthesiologists.
P = 0.004 versus group B; one-way analysis of variance.
Volume and total dose of lidocaine and intraoperative visual analogue scale (VAS) pain scores in adults undergoing hernia repair under local infiltration anaesthesia, randomized to receive 0.25% (group A), 0.33% (group B) or 0.5% (group C) lidocaine (n = 120.
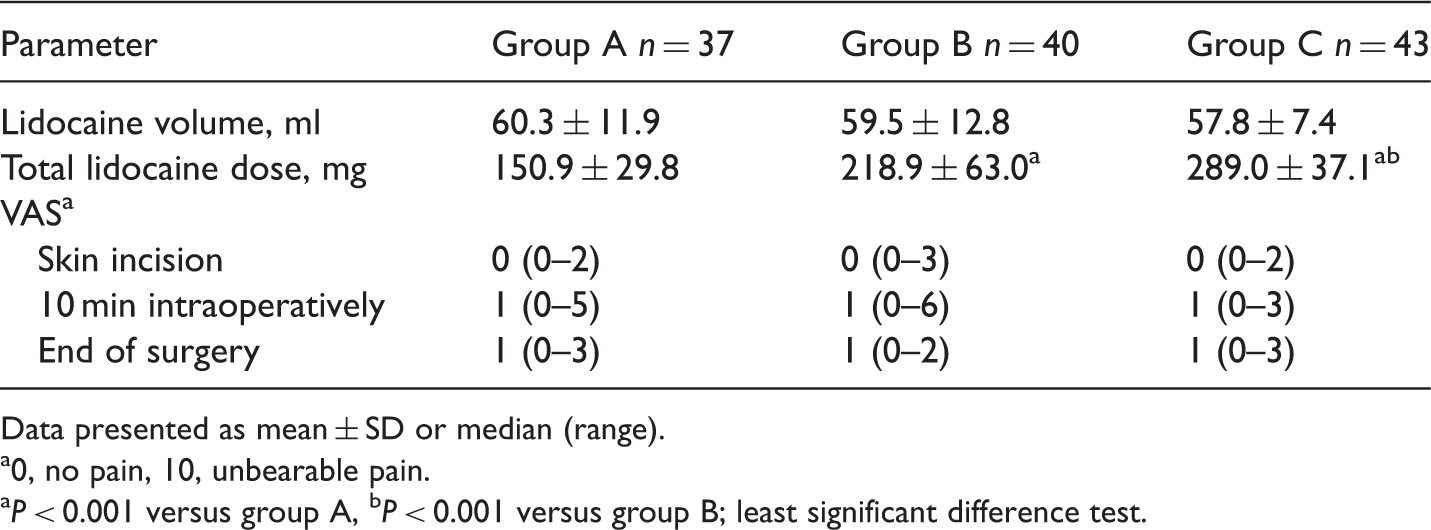
Data presented as mean ± SD or median (range).
0, no pain, 10, unbearable pain.
P < 0.001 versus group A, bP < 0.001 versus group B; least significant difference test.
Duration of surgery, degree of satisfaction and number of patients with procedure-related complications in adults undergoing hernia repair under local infiltration anaesthesia, randomized to receive 0.25% (group A), 0.33% (group B) or 0.5% (group C) lidocaine (n = 120.
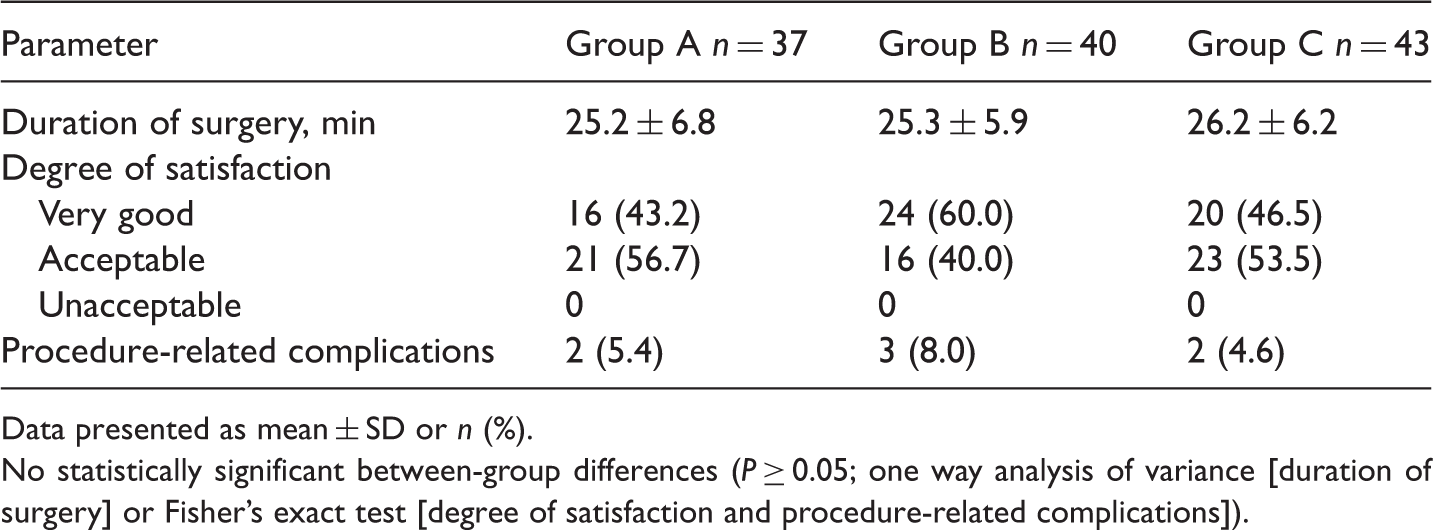
Data presented as mean ± SD or n (%).
No statistically significant between-group differences (P ≥ 0.05; one way analysis of variance [duration of surgery] or Fisher’s exact test [degree of satisfaction and procedure-related complications]).
All patients were treated successfully and none required conversion to general or spinal anaesthesia. There were no cases of cardiovascular or central nervous system toxicity and no patient required sedation or analgesia. In group B, two hypertensive patients forgot to take their oral medication and were administered intravenous antihypertensive drugs. There were no between-group differences in intraoperative vital signs.
Discussion
The concentration of lidocaine used for inguinal hernia repair usually varies between 0.5% and 2%,3,7,9,10 and may be combined with other local anaesthetics or epinephrine.18,19 High-dose lidocaine is acceptable in situations where only a small volume is required (such as dentistry) but may lead to overdose in more complex procedures such as goitre or hernia repair; 7 a problem compounded by the increased toxicity of lidocaine in the presence of other local anaesthetics (e.g. bupivacaine) or epinephrine.13,14 The current study used low concentrations of lidocaine (0.25%–0.5%) for hernia repair under local infiltration anaesthesia. All patients successfully completed surgery, with none requiring conversion, sedation or analgesia, and no cases of cardiovascular or central nervous system toxicity. The procedure and anaesthesia were evaluated as ‘very good’ or ‘acceptable’ in all cases. These findings indicate that a lidocaine concentration of 0.25% provides satisfactory anaesthesia in inguinal hernia repair.
Hernia repair under local anaesthesia is confined to specialized hernia hospitals and centres,20,21 and has a high conversion rate to general or spinal anaesthesia,22,23 possibly due to pain or an unpleasant experience during surgery.24,25 Patients in the current study were not given preoperative sedation or analgesia, in order to ensure the accuracy of VAS scores. Care was taken to record VAS scores at skin incision, 10 min after the beginning of surgery and again at the end of surgery, in contrast to others who only evaluated pain at the end of the procedure.10,19,24 The absence of statistically significant between-group differences in VAS scores in the present study suggests that all lidocaine concentrations reached the upper portion of the dose-response curve, obscuring potency differences and resulting in similar effects for different doses. 26
Lidocaine had a rapid onset in the present study, with 93% of patients reporting a VAS score of 0–1 immediately after anaesthesia (at skin incision). The duration of surgery was well within the 1–2 h duration of action of lidocaine. 6 Lidocaine-related toxicity is common and often associated with overdose.7,11,12 The recommended maximum dose is 500 mg lidocaine (for local anaesthesia) when used in combination with epinephrine. 27 The use of high concentrations of lidocaine makes it easier to exceed this maximum, in particular when patients are obese or have larger, bilateral or recurrent hernias.28,29 The present study indicated positive correlations between BMI and lidocaine volume, and total dose. Lidocaine is mainly metabolized by the liver, and may therefore be associated with a higher level of toxicity at normally safe doses, in patients with hepatic diseases.22,30 An additional problem encountered in local infiltration anaesthesia is a shortage of anaesthetic, especially in obese patients. 28 The low concentrations of lidocaine used in the present study allow the use of additional anaesthetic with little risk of overdose.
The current study has several limitations. First, plasma concentrations of lidocaine were not measured, and it is therefore not possible to determine whether each concentration reached the upper portion of the dose–response curve. Secondly, the failure to exclude patients with hepatic or renal disease may have influenced the accuracy of the data.
In conclusion, each of the three lidocaine concentrations assessed in the present study provided satisfactory anaesthetic effects and pain relief. The mean dose of lidocaine consumed in group A (0.25%) was significantly lower than that used in the other two groups, and may have led to a lower risk of local anaesthetic toxicity. Local anaesthesia with 0.25% lidocaine has been routinely used in unilateral, bilateral and recurrent inguinal hernias in our centre.
Footnotes
Declaration of conflicting interest
The Authors declare that there are no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.