
Abstract
Objective
The study evaluated the clinical intraoperative effects of intrathecal administration of fentanyl on shoulder tip pain in patients undergoing laparoscopic total extraperitoneal inguinal hernia repair (TEP) under spinal anaesthesia.
Methods
Patients undergoing TEP were allocated in a double-blinded, prospective, randomized manner to two groups. Spinal anaesthesia was induced by intrathecal administration of 2.8 ml of 0.5% hyperbaric bupivacaine (14 mg) in the control group and with 2.6 ml of 0.5% hyperbaric bupivacaine (13 mg) and 10 µg fentanyl (0.2 ml) in the experimental group.
Results
The quality of muscle relaxation, adequacy of operative space and incidence of pneumoperitoneum were similar in the two groups (n = 36 per group). Compared with the control group, the experimental group had significantly fewer cases of hypotension (12 [33.3%]) versus 23 [63.9%]) and shoulder tip pain (nine [25%] versus 18 [50%]). Intraoperative shoulder tip pain was more severe in the control group than in the experimental group.
Conclusions
Addition of intrathecal fentanyl to local anaesthetic can relieve shoulder tip pain with no change in complications, especially hypotension, during TEP under spinal anaesthesia.
Keywords
Introduction
With the technical advances that have been made, laparoscopic total extraperitoneal inguinal hernia repair (TEP) is considered a procedure with a good safety profile that offers advantages over open repair.1,2 TEP has conventionally been performed under general anaesthesia. The reasons for preferring general anaesthesia for TEP rather than spinal anaesthesia include anaesthetists’ unfamiliarity with spinal anaesthesia for laparoscopic surgery, fears of complications resulting from a relatively high level of spinal block, and difficulty in the management of intraoperative pain and discomfort. However, haemodynamic instability, delayed or eventful recovery, sore throat and postoperative cognitive dysfunction are commonly observed during and after general anaesthesia. The need for general anaesthesia has therefore been considered a major disadvantage of TEP.3,4
Although there have been several reports of experience with TEP and of the safety and feasibility of TEP under regional anaesthesia,5–9 few studies have provided detailed descriptions of TEP under regional anaesthesia from an anaesthetic perspective, such as the amount of intrathecal anaesthetics required, the requirement for intravenous analgesics, the adequate sensory level of anaesthesia and the management of intraoperative discomfort and pain. Moreover, there have been no published studies comparing clinical effects according to the addition or omission of intrathecal lipophilic opioids during TEP under spinal anaesthesia. Intrathecal opioids are usually added to local anaesthetics for spinal anaesthesia in order to improve analgesic quality without prolonging motor block.10,11
We hypothesized that adding an opioid to hyperbaric bupivacaine for spinal anaesthesia would improve anaesthetic quality without leading to additional complications during TEP. The aim of the study was to evaluate the anaesthetic quality of intrathecal administration of bupivacaine alone, compared with bupivacaine plus fentanyl, in patients undergoing TEP under spinal anaesthesia.
Patients and methods
Study population
The study was approved by the Institutional Review Board of Konyang University Hospital, Daejeon, Republic of Korea (reference, 11-87) and registered with the Korean Clinical Research Information Service (http://cris.nih.go.kr; KCT0000687). Written informed consent was obtained from patients before the study was begun. Patients were excluded if any of the following criteria were fulfilled: (i) coagulopathy or other bleeding diathesis; (ii) infection at the injection site for spinal anaesthesia; (iii) a history of allergy or hypersensitivity to local anaesthetics; (iv) age <20 years; (v) TEP scheduled for both sides. The study was conducted as a parallel-group trial and patients of American Society of Anesthesiology physical status I–III (http://www.asahq.org) were randomly allocated (allocation ratio 1 : 1) to undergo the procedure either in a group given bupivacaine alone (control) or in a group given bupivacaine plus fentanyl (experimental group). Randomization was done before anaesthesia induction using the sealed envelope method.
All patients were informed about the possibility of conversion to general anaesthesia at any time during the operation, at the request or on the advice of the patient, anaesthetist or surgeon, because of pain or discomfort.
Anaesthesia
On the patient’s arrival at the operating theatre, without premedication, routine noninvasive monitoring, comprising pulse oximetry, electrocardiography and noninvasive blood pressure monitoring commenced. Oxygen was given at 6 l/min using a face mask; end-tidal carbon dioxide was monitored. Before spinal anaesthesia, the stopcock of the peripheral vein fluid line for crystalloid was fully opened, and an 18 gauge angiocatheter was used. The patient was positioned in the right or left lateral decubitus position for spinal anaesthesia according to the side involved. Using an aseptic technique, a 25 gauge Quincke spinal needle was inserted into the subarachnoid space through the L3/4 or L4/5 intervertebral space using a midline approach.
Intrathecal anaesthetics were prepared by a registered nurse who was blind to the study group allocation of the patients and did not participate in patient care; the syringes for the two study groups (bupivacaine versus bupivacaine plus fentanyl) were indistinguishable. Once the intrathecal position of the needle had been confirmed by leakage and slight aspiration of cerebrospinal fluid, the intrathecal anaesthetics were introduced. On the basis of other research,5,6,12 2.8 ml of 0.5% hyperbaric bupivacaine (14 mg) was administered in the control group and 2.6 ml of 0.5% hyperbaric bupivacaine (13 mg) plus 10 µg fentanyl (0.2 ml) in the experimental group. Spinal anaesthesia in all patients was conducted and managed by an anaesthetist who was blind to both the study group allocation of the patients and the intrathecal anaesthetics being administered; the anaesthetist was instructed only to follow the protocol for spinal anaesthesia.
After the administration of intrathecal anaesthetics, the position of the patient was changed to supine and adjusted to reach the maximal block level of T6. After the maximal block level of T6 had been confirmed and maintained for 20 min, the patient was moved to the neutral position and the operation was performed. The sensory block level was assessed using the pinprick test (24 gauge hypodermic needle), while the motor block level was assessed using the Modified Bromage scale (MBS, 0, no paralysis; 1, unable to raise extended leg; 2, unable to flex knee; 3, unable to flex ankle). 13 The ability to reach a sensory block at T6 and an MBS of 0 within 20 min after injection of the intrathecal anaesthetics was considered to constitute block failure. Hypotension was defined as a fall in mean systemic blood pressure (MBP) to >25% of preanaesthetic MBP or to <60 mmHg. Phenylephrine (50 µg) was injected if hypotension occurred without bradycardia (<60 beats/min); ephedrine (5 mg) was injected if hypotension occurred with bradycardia; atropine (0.5 mg) was injected if bradycardia occurred without hypotension.
Surgical procedure
Under spinal anaesthesia, all patients were placed in the supine position. The skin of the entire abdomen was prepared and a vertical skin incision ∼15 mm in length was made directly below the umbilicus. The linea alba was visualized and grasped on either side with Kocher clamps. The linea alba was elevated and a vertical 10-mm incision was made through the fascia. After exposure of the rectus muscle, blunt dissection was performed between the rectus muscle and the posterior rectus sheath using a Kelly clamp. Using a Spacemaker™ Structural Balloon Trocar system (Autosuture, Norwalk, CT, USA), the distension balloon was then inflated. After the balloon had been removed, carbon dioxide gas was introduced into the extraperitoneal space at 10 mmHg. A standard 0° videoscope was introduced into the port and advanced into the preperitoneal space. One trocar port was placed suprapubically 3 cm above the symphysis pubis, and another trocar was placed between the camera port and the suprapubic port. The inferior epigastric vessels were identified along the lower portion of the rectus muscle and retracted anteriorly. Lateral dissection was carried out to the anterior superior iliac spine. The gonadal vessel and the vas deferens were parietalized in male patients. After full dissection of the preperitoneal space, the herniated sac was retracted using atraumatic forceps. A Parietex™ Mesh (Sofradim, Trévoux, France) was inserted through the camera port and positioned on the anterior abdominal wall covering the Hesselbach triangle, the internal inguinal ring and the medial portion of the external iliac vein. The Parietex™ mesh was then secured to the pubic tubercle with a Tacker™ fixation device (Autosuture) in all patients. Surgery was performed using the same surgical protocol and the same surgical team in both groups. Operation time was defined as the interval from skin incision to completion of skin closure after the surgical procedure.
Anaesthetic care and measurements
Shoulder tip pain was assessed after carbon dioxide insufflation, using four grades [0, no pain; 1, mild pain but no need for analgesic; 2, moderate pain and need for analgesic; 3, severe pain and no response to analgesics (need for conversion to general anaesthesia)]. If any patient experienced shoulder tip pain, ketamine was administered intravenously at 0.5 mg/kg. If shoulder tip pain had not subsided within 3 min, ketamine was again administered intravenously at 0.5 mg/kg. Intravenous fentanyl was administered at 0.5 µg/kg if shoulder tip pain had not subsided after a total dose of 1.0 mg/kg ketamine. At the end of surgery, for those patients who had not complained of shoulder tip pain during surgery, we checked whether shoulder tip pain had occurred during surgery. The surgeon, who was unaware of the study details, was asked about the occurrence of pneumoperitoneum secondary to peritoneal tear, quality of muscle relaxation and adequacy of operative space immediately after surgery.
All side-effects, such as nausea, headache, urinary retention, etc., were assessed on the first postoperative day by a registered nurse on the ward, who was aware that the anaesthetic method was spinal anaesthesia and not general anaesthesia, but was unaware as to which study group each patient had been allocated.
Statistical analyses
Data were analysed using SPSS® software, version 18.0 (SPSS Inc., Chicago, IL, USA) for Windows®. The primary outcome variable was the frequency of shoulder tip pain after carbon dioxide insufflation. The incidence of shoulder tip pain was 50% in a previous pilot study of 10 patients given 2.8 ml of 0.5% hyperbaric bupivacaine for TEP. A 75% reduction in the frequency of shoulder tip pain was considered clinically significant. For a power of 0.9 and an α-value of 0.05, a sample size of 36 for each group was required. Normal distribution of continuous variables was assessed using the Kolmogorov–Smirnov test. Continuous variables were expressed as mean ± SD and compared using the two-tailed Student’s t-test or the Mann–Whitney U-test, as appropriate. Categorical variables were compared using the χ2-test or Fisher’s exact test, as appropriate. The difference in the degree of shoulder tip pain between the two groups was analysed using the χ2-test for trend (linear × linear association). A P-value < 0.05 was considered statistically significant.
Results
Patient flow during the study period is shown in Figure 1. In total, 84 patients underwent TEP, of whom 10 were excluded (four were aged <20 years, one was scheduled for TEP on both sides and five declined to participate). Two patients in the control group were withdrawn because of failed spinal block and conversion to general anaesthesia. Thus, 36 patients in each group were included in the final analysis (Figure 1). There were no significant differences in patient characteristics between the two groups (Table 1).
CONSORT flow diagram for a study comparing the effects of intrathecal fentanyl on shoulder tip pain in laparoscopic total extraperitoneal inguinal hernia repair under spinal anaesthesia. Experimental group received intrathecal bupivacaine plus fentanyl; control group received intrathecal bupivacaine only. Patient characteristics and operative data in patients given intrathecal hyperbaric bupivacaine with (experimental group) or without (control group) intrathecal fentanyl for total extraperitoneal inguinal hernia repair under spinal anaesthesia. Data presented as mean ± SD or n patients. There were no significant differences between the two groups. Student’s t-test (two-tailed). Fisher’s exact test. χ2-test. ASA, American Society of Anesthesiologists (http://www.asahq.org).

Relationship between pneumoperitoneum and shoulder tip pain in patients given intrathecal hyperbaric bupivacaine, with or without intrathecal fentanyl, for total extraperitoneal inguinal hernia repair under spinal anaesthesia.

Data presented as n (%) of patients.
Presence of shoulder tip pain, pneumoperitoneum versus no pneumoperitoneum, P = 0.000 (Fisher’s exact test).
Intraoperative characteristics assessed by the surgeon in groups of patients given intrathecal hyperbaric bupivacaine with (experimental group) or without (control group) intrathecal fentanyl for total extraperitoneal inguinal hernia repair under spinal anaesthesia.

Data presented as n (%) of patients.
There were no significant differences between the two groups.
Fisher’s exact test.
χ2-test.
Intraoperative clinical effects in groups of patients given intrathecal hyperbaric bupivacaine with (experimental group) or without (control group) intrathecal fentanyl for total extraperitoneal inguinal hernia repair under spinal anaesthesia.

Data presented as n (%) of patients or mean ± SD.
χ2-test.
Student’s t-test (two-tailed).
χ2-test for trend (linear × linear association).
Fisher’s exact test.
NS, not significant.
Postoperative side-effects in groups of patients given intrathecal hyperbaric bupivacaine with (experimental group) or without (control group) intrathecal fentanyl for total extra-peritoneal inguinal hernia repair under spinal anaesthesia.
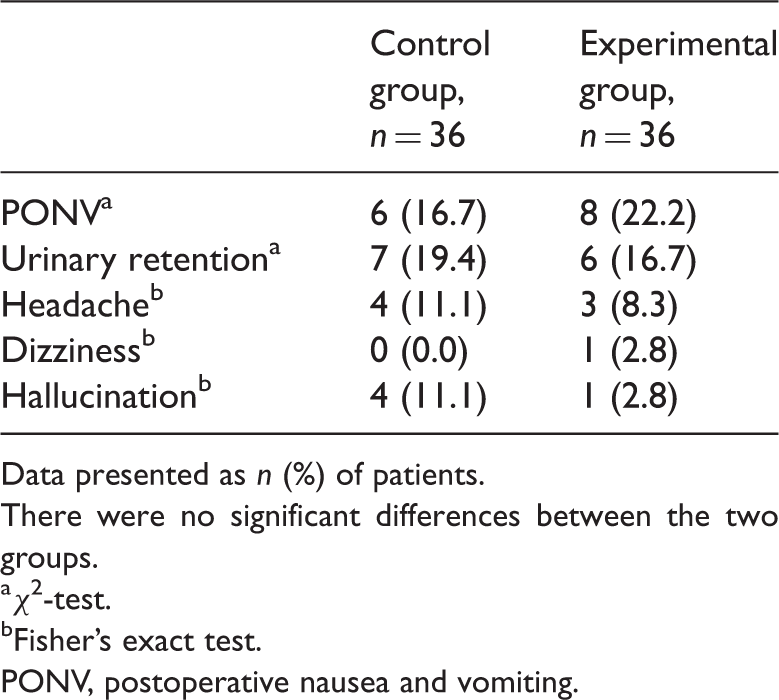
Data presented as n (%) of patients.
There were no significant differences between the two groups.
χ2-test.
Fisher’s exact test.
PONV, postoperative nausea and vomiting.
Discussion
The present study showed that the addition of 10 µg of fentanyl to 0.5% hyperbaric bupivacaine for spinal anaesthesia decreased the frequency of intraoperative hypotension and the frequency and severity of intraoperative shoulder tip pain, compared with a similar single-injection volume of 0.5% hyperbaric bupivacaine, for spinal anaesthesia in patients undergoing TEP. The experimental regimen did not increase intra- or postoperative complications compared with the same volume of intrathecal injection of 0.5% hyperbaric bupivacaine.
Shoulder tip pain is one of the leading causes of conversion to general anaesthesia in patients undergoing TEP under spinal anaesthesia. This pain is strongly associated with the occurrence of pneumoperitoneum. 7 The frequency of pneumoperitoneum during TEP has been reported to be between 10 and 64%.14–16 In the present study, pneumoperitoneum was seen in 25 of the 72 (34.7%) participating patients. Shoulder tip pain was more frequent in patients with pneumoperitoneum, regardless of whether they were in the experimental or the control group. Pneumoperitoneum-induced shoulder tip pain is mainly attributable to diaphragmatic and peritoneal irritation from carbon dioxide, mediated by the phrenic and cervical spinal nerves. Thus, it was considered that complete prevention of shoulder tip pain in patients undergoing TEP with spinal anaesthesia could not be achieved simply by using spinal anaesthesia. 7 However, the present study showed a significant reduction in shoulder tip pain in the group receiving fentanyl in addition to hyperbaric bupivacaine under spinal anaesthesia. The reduction in shoulder tip pain when fentanyl is added to hyperbaric bupivacaine might be explained as follows. Intrathecal administration of fentanyl would produce analgesic effects in regions separate from the site of fentanyl administration through a neurally mediated action. 17 Opioid was detectable in the cisterna magna within 30 min after lumbar intrathecal administration 18 and was redistributed within the cerebrospinal fluid (CSF). This distribution of opioid within the CSF could explain the clinically significant effects, such as respiratory depression, that occur immediately after lumbar spinal injection. 19
Intraoperative shoulder tip pain control is an important factor affecting the successful performance of TEP under regional anaesthesia when a pneumoperitoneal tear occurs. 7 In the present study, shoulder tip pain, regardless of the occurrence of pneumoperitoneum, was easily managed with intravenous ketamine and fentanyl. Ketamine has potent analgesic and sedative effects while maintaining protective airway reflexes and minimal respiratory depression, 20 and often increases blood pressure and heart rate. 21 TEP under spinal anaesthesia requires a relatively high level of anaesthetic block and is associated with hypotension, bradycardia and respiratory depression. Ketamine was therefore the first choice of analgesic agent in the present study, in which a small initial dose (0.5 mg/kg) and subsequent incremental use (up to 1 mg/kg) provided effective control of shoulder tip pain without cardiovascular complications.
Studies have reported that intrathecal fentanyl added to bupivacaine could decrease the incidence of hypotension while maintaining adequate anaesthesia because it reduced the dose of bupivacaine required for spinal anaesthesia.22,23 This concurs with the results obtained in the present study, in which the incidence of hypotension in the experimental group was significantly lower than that in the control group (P = 0.009). However, hypotension was easily corrected, without complications, by intravenous administration of ephedrine and phenylephrine in both groups.
The optimum doses of intrathecal anaesthetics and adequate block level have not been established for TEP under spinal anaesthesia. Lau et al. 5 reported that 3–3.5 ml of 0.5% hyperbaric bupivacaine could produce sensory block at the T10 level with adequate analgesia for TEP under spinal anaesthesia. Ismail and Garg 6 used 4 ml of 0.5% hyperbaric bupivacaine for TEP under spinal anaesthesia, but did not mention an adequate anaesthetic level. Lal et al. 7 and Azurin et al. 24 recommended that a sensory level of above T67 and above T4, 24 was adequate for the success of TEP under epidural anaesthesia. On the basis of other reports,5,7,24 the block level was regarded as T6 in the present study. However, we used 2.8 ml of bupivacaine in the control group and 2.6 ml in the experimental group because the patients enrolled in the present study were smaller and older than those enrolled in previous studies.5,6,12
Postoperative nausea and vomiting (PONV) is among the most troublesome postoperative side-effects and reduces patients’ overall satisfaction rates. 25 Intra- and postoperative use of intravenous opioids increase the risk of PONV.26,27 In contrast, a single intrathecal administration of fentanyl does not increase the frequency of PONV.28,29 The frequency of PONV was similar in the two groups in the present study, although opioid was used intraoperatively in the experimental group.
The present study had the limitation that it did not include patients undergoing bilateral TEP. Intrathecal fentanyl might be expected to show the same effects on shoulder tip pain in bilateral TEP as in unilateral TEP because of the redistribution of the opioid in the CSF. However, the effect of intrathecal fentanyl on shoulder tip pain in bilateral TEP under spinal anaesthesia could not be guaranteed, because of the longer duration of the surgical procedure required and the longr exposure to carbon dioxide insufflation.
In conclusion, the addition of 10 µg of fentanyl to 0.5% hyperbaric bupivacaine for TEP under spinal anaesthesia decreased the incidence and severity of shoulder tip pain with no change in complications. It also decreased the incidence of intraoperative hypotension, compared with same volume of intrathecal injection of 0.5% hyperbaric bupivacaine alone for spinal anaesthesia.
Footnotes
Declaration of conflicting interest
The authors declare that there are no conflicts of interest.
Funding
This research was supported by the Basic Science Research Program through the National Research Foundation of Korea (NRF), funded by the Ministry of Education, Science and Technology (grant number 2012R1A1A1001819).