
Abstract
Objective
To explore the efficacy and safety of single-incision laparoscopic (SIL) technique compared with the traditional three-port total extraperitoneal (TEP) technique for inguinal hernia repair.
Methods
This prospective, randomised study involved patients who underwent surgery for inguinal hernia at our hospital from December 2021 to July 2023. Patients were randomly assigned to SIL-TEP or TEP groups based on a computer-generated random number table. Perioperative clinical indicators for the surgical approaches were evaluated.
Results
Of the 127 patients eligible for study, 66 were randomised to the SIL-TEP group and 61 to the TEP group. The operation time for SIL-TEP was significantly longer than for TEP but the time to return to normal activities was significantly shorter and short-term pain score was significantly lower. There were no differences between groups in intraoperative blood loss, postoperative hospital stays, pain relief time, hospitalization costs or cosmetic satisfaction scores.
Conclusion
While SIL-TEP is more challenging than TEP for hernia repair, we found that at our centre it is comparable with regard to overall safety and feasibility. Further studies are needed to validate our findings.
Introduction
Single-incision laparoscopic total extraperitoneal (SIL-TEP) hernia repair was first described in 2009.1,2 Early studies suggested that the SIL technique would reduce the number of incisions, minimize surgical trauma, alleviate postoperative pain, and result in a superior cosmetic outcome. 3 However, as the technique evolved, specific problems and limitations became apparent. 4 For example, it has been suggested that the limited operating space, interference between instruments, and increased difficulty of the procedure, coupled with a steep learning curve, could potentially raise the risk of complications. 5 To avoid operational interference, flexible single-port laparoscopic instruments have been developed, but they have not been widely adopted due to their high cost. 6 Nevertheless, recent optimizations and improvements in SIL-TEP have significantly enhanced its efficacy. Indeed, several studies and a recent systematic review and meta-analysis, found no significant differences between SIL-TEP and the traditional TEP in operation time, blood loss, postoperative hospital stay, complications, outcomes, or recurrence rates.6–10 Moreover, the data were comparable to results where open tension-free repair techniques had been used.11,12 We designed this study to explore the efficacy and safety of the SIL-TEP technique compared with the traditional three-port TEP technique for inguinal hernia repair at our centre.
Methods
This prospective, randomised study involved patients who underwent surgery for inguinal hernia at our hospital from December 2021 to July 2023. Using a computer-generated, random number table, patients requiring hernia repair were assigned to either the SIL-TEP group or the traditional TEP group. To ensure blinding of allocation, the randomization process was conducted by researchers not involved in the clinical treatment of the patients. Inclusion criteria were as follows: ≥18 years of age; diagnosed with inguinal hernia for the first time; agreed to undergo laparoscopic surgery; American Society of Anaesthesiologists (ASA) score of ≤3. 13 Patients with severe concurrent disease, coagulation disorders, history of lower abdominal surgery, or strangulated/recurrent inguinal hernia, were excluded from the study.
The study was approved by the medical ethics committee of Longshan Central Hospital, Cixi, Zhejiang (BD 34). All participants were fully informed about the purpose, procedures, potential risks, and benefits of the study and provided written informed consent before its commencement. All data were collected and retained anonymously. The reporting of this study conforms to STROBE guidelines. 14
Data collection
All patients underwent a comprehensive clinical evaluation at the start of the study with sex, age, body mass index (BMI), and type, and location of the hernia being recorded. Detailed data related to the hernia repair surgery and a minimum of one year follow-up data were also collected to assess surgical outcomes and incidence of complications. Evaluation of surgical outcomes included: operation time; intraoperative blood loss; need for conversion to a different surgical method; intraoperative complications; postoperative pain score; time required to resume normal activities; length of postoperative hospital stay; incidence of postoperative complications.
Operation time was calculated from the beginning of the skin incision to the end of skin closure. Intraoperative blood loss was estimated from the volume of contents in the suction device and weight difference of soaked gauze. Instances requiring conversion from laparoscopic to open surgery and reasons for the change were noted. Pain intensity was evaluated using a visual analogue scale (VAS), with trained medical personnel uniformly scoring at 1, 3, and 7 days, and one-month postoperatively, on a scale of 0 to 10 (0, no pain; 10, unbearable pain). Postoperative complications that were screened included: chronic pain; incision infection; seroma; local hematoma; urinary retention; incisional hernia; hernia recurrence. In addition, one-month post-surgery, using a 10-point scale (0, no satisfaction; 10, complete satisfaction) that encompassed factors such as incision healing speed and overall aesthetic satisfaction, patients were asked to rate their satisfaction regarding the incision's cosmetic outcome.
Surgical methods
Two surgeons from our team with extensive experience in laparoscopic procedures performed all surgeries. For patients in the TEP group, a traditional three-port laparoscopic TEP inguinal hernia repair was conducted. The operation began with a transverse incision slightly lateral to the umbilical edge, approximately 1 cm long. After incising the skin and subcutaneous fat layer, the anterior sheath of the rectus muscle on the affected side was exposed and incised. Subsequently, with the aid of a retractor, the rectus muscle was dissected, and a 10-mm trocar was placed in front of the posterior sheath of the rectus muscle to establish a CO2 pneumoperitoneum, maintained at 12 mmHg. After the initial creation of the Retzius space using a blunt dissection technique, two 5-mm trocars were inserted at the upper and lower thirds of the line connecting the umbilicus to the pubic symphysis, serving as operative ports. The posterior sheath of the rectus muscle was partially incised, and the Bogros space was dissected. The hernia sac was reduced, ensuring at least 6 cm of peritonealisation of the spermatic cord. At this point, the maximum diameter of the hernia orifice was measured. A suture was laid along the longest axis of the hernia orifice, cut, and then removed from the body. The length of the suture was measured outside the body using a ruler, determining the maximum diameter. After completely freeing the myopectineal orifice, a 15 × 10 cm Bard 3 D-Max mesh was placed, ensuring coverage medially to the midline, laterally up to the level of the anterior superior iliac spine, superiorly extending 3 cm above the internal ring, and inferiorly 2 cm below the pubic tubercle. The mesh was ensured to lie anterior to the peritoneal reflection. Finally, under direct vision, the gas was evacuated, the laparoscope was withdrawn, and the trocar sites were closed.
For patients in the SIL-TEP group, the operation commenced with a semi-circular incision below the umbilicus, approximately 2.5 cm long. After incising the skin and subcutaneous tissue, the anterior sheath of the rectus muscle on the affected side was exposed and incised. A single-port laparoscopic device was then inserted and secured anterior to the posterior sheath of the rectus muscle to establish a CO2 pneumoperitoneum. Subsequently, using a 30-degree laparoscope and a dual-grasper technique, the space anterior to the posterior sheath of the rectus muscle was dissected to create access to the Retzius space. A disposable wound retractor (60 mm diameter) was used to retract the fascia and served as a base, over which a sterile surgical glove was fitted. Four stitches were used to secure the glove to the retractor, and the upper ring of the retractor was inverted to expand the incision and tighten the retractor and glove. Trocars of 10, 5, and 5 mm were placed at the glove's thumb, index, and ring finger positions, respectively, to serve as working channels and were tied with sutures to ensure stability. The 10-mm trocar was used for the camera and CO2 insufflation (Figure 1). Subsequent steps were similar to the three-port TEP group, and included partial incision of the posterior sheath of the rectus muscle, dissection of the Bogros space, hernia sac reduction, at least 6 cm of peritonealisation of the spermatic cord, and placement of the Bard 3 D-Max mesh. Under direct vision, gas was evacuated, the laparoscope was withdrawn, and the trocar sites were closed.

Single-port laparoscopic hernia repair schematic.
Statistical methods
All data collected were analysed using R software (version 4.3.1). A P-value < 0.05 was considered to indicate statistical significance. Categorical variables were expressed as frequencies (percentages) and analysed using χ2 tests or Fisher's exact tests as appropriate. Continuous variables were expressed as mean ± standard deviation and analysed using t-tests or Mann-Whitney U-tests as appropriate. Additionally, we conducted a linear regression analysis using data on hernia diameter and operative time.
Results
In total, 127 patients (109 men, 18 women) with inguinal hernias were recruited into the study. Their baseline demographic and clinical characteristics are shown in Table 1. Overall, there were 101 cases of unilateral inguinal hernia and 26 cases of bilateral inguinal hernia. Most hernias were of the indirect type (112 cases), with direct hernias being the second most common (11 cases). There were just two cases for each of scrotal and femoral hernias.
Baseline Demographics and Clinical Characteristics.

Data are expressed as, n, n (%) or mean ± SD.
SIL, single-incision laparoscopic; TEP, total extraperitoneal, ns, not statistically significant.
Of the 127 patients, 66 patients were allocated the SIL-TEP procedure and 61 the traditional TEP procedure. For the SIL-TEP group, average age was 63.8 ± 10.5 years and average hernia ring diameter was 4.32 ± 1.19 cm. For the TEP group, average age was 66.5 ± 9.6 years and average hernia ring diameter was 4.21 ± 1.56 cm. There were no statistically significant differences in baseline demographic or clinical characteristics between the two groups (Table 1).
While the average surgery time for unilateral and bilateral hernias was statistically significantly longer for the SIL-TEP group compared with the TEP group, the time to return to normal activities was statistically significantly shorter (P < 0.05; Table 2). However, there were no statistically significantly differences between groups in intraoperative blood loss, postoperative hospital stays, pain relief time, hospitalization costs or cosmetic satisfaction scores (Table 2).
Comparison of perioperative data.
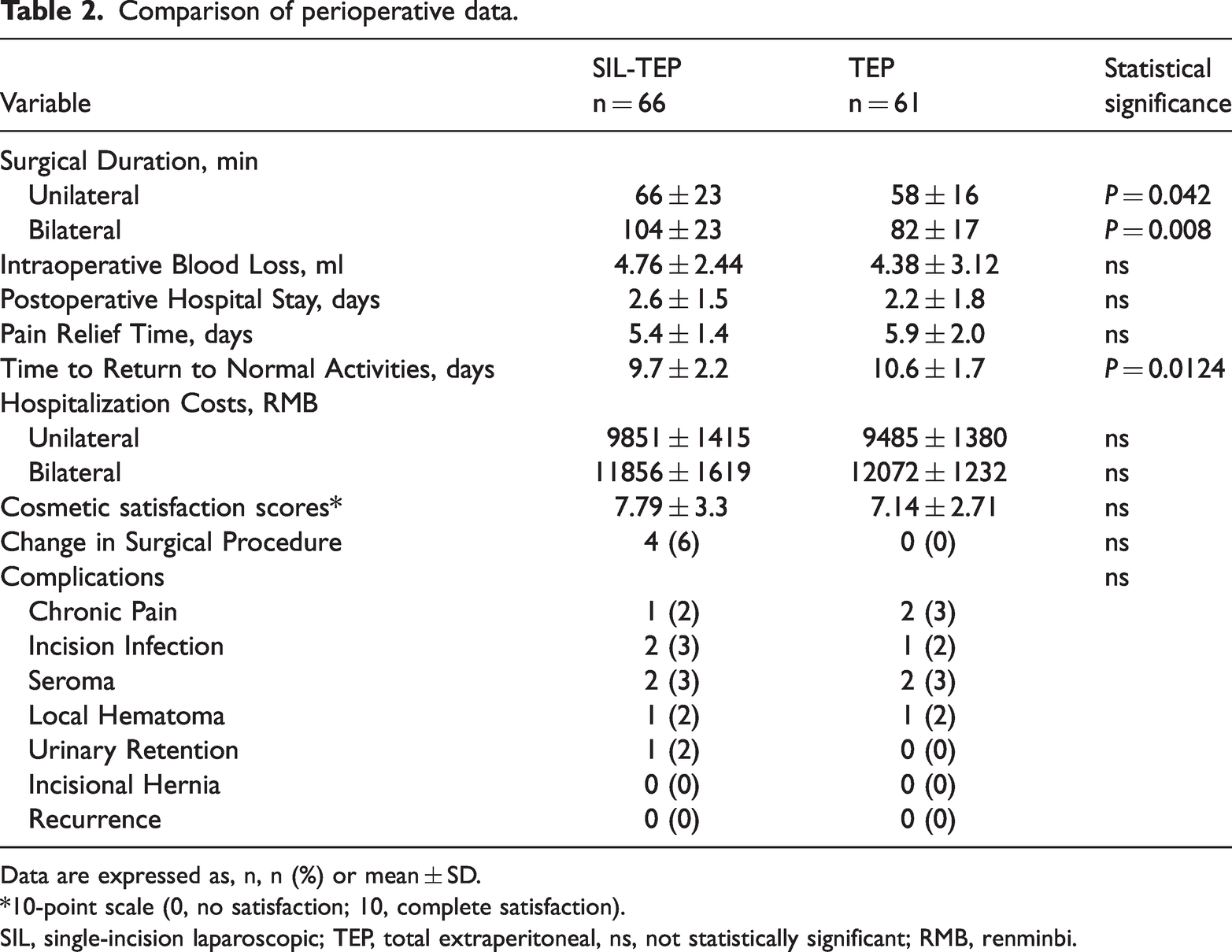
Data are expressed as, n, n (%) or mean ± SD.
*10-point scale (0, no satisfaction; 10, complete satisfaction).
SIL, single-incision laparoscopic; TEP, total extraperitoneal, ns, not statistically significant; RMB, renminbi.
All surgeries in the TEP group were completed successfully but in the SIL-TEP group, four cases (6%) were converted to a two-port operation due to increased operative difficulties. However, there were no statistically significant differences between the two groups in terms of complications, both short- or long-term (Table 2).
To assess the relationship between hernia diameter and operative time, we conducted a linear regression analysis. For the SIL-TEP group, the operative time in relation to hernia diameter was represented by the equation y = 3.17x + 47.30 with an 2 of 0.22, while for the conventional TEP group, it was = 1.59x; + 48.33 with an 2 of 0.26, (Figure 2). The difference in the rate of change of operative time with increasing hernia diameter between the two surgical techniques was statistically significant (P < 0.05) with surgery duration being more significantly influenced by hernia diameter in the SIL-TEP group compared with the TEP group.

Relationship between unilateral hernia diameter and operative time.
Postoperative pain scores on Day 1 were statistically significantly lower for SIL-TEP group (1.95 ± 0.41) compared with TEP group (2.35 ± 0.39) (P < 0.05). However, at follow-ups on Day 3, Day 7 and one month later, there were no significant differences in pain scores between the two groups (Table 3).
Comparison of postoperative pain intensity VAS scores.

Data are expressed as mean ± SD.
VAS, visual analogue scale; SIL, single-incision laparoscopic; TEP, total extraperitoneal, ns, not statistically significant.
Discussion
Single-incision laparoscopic surgery represents an evolution of traditional laparoscopic surgery by optimizing instruments and surgical technique. This minimally invasive approach has been used not only for inguinal hernia repairs, but also for cholecystectomies, myomectomies, and gastrointestinal surgeries.15–17 Despite its theoretically less invasive nature, the challenges and effectiveness of single-incision laparoscopic surgery in practical applications warrant further investigation. Accordingly, we designed this present study to explore differences in efficacy and safety between the SIL-TEP technique and the traditional three-port laparoscopic TEP technique for inguinal hernia repair at our centre.
We found that the operation time for the SIL-TEP group was significantly longer than for the TEP group for both unilateral and bilaterial hernia surgery. We attribute these differences to several factors. For example, the SIL-TEP technique involves placing three trocars through a single incision and demands a high requirement for air tightness. During surgery, as the camera and operating forceps are usually parallel, the surgical smoke, if not evacuated promptly, can quickly obscure the lens, which requires frequent wiping, and so can disrupt airtightness and prolong the operation. In addition, the movement of the forceps may inadvertently rotate the camera, and hinder the establishment of a stable tri-point operation platform. The proximity and parallel arrangement of the camera and forceps in a confined pneumoperitoneum space exacerbates instrument interference, particularly when reducing large hernia sacs, and can limit the visual field and operative angle. Furthermore, in our study we used a homemade glove port, which typically adds 3–5 minutes to the procedure. Although we found the glove port convenient and cost-effective, it can significantly restrict instrument mobility due to entanglement and resistance, especially at certain angles, and can lack a stable fulcrum in the suspended state. Therefore, it demands a high degree of skill from the operating surgeon and assistant. Other critical factors which may have affected the procedure, include our surgical team's experience, proficiency, and coordination, which may have differed from previous studies. 7 Our observation of a significant increase in surgical time of SIL-TEP compared to TEP in bilateral hernia surgery probably reflects the complexity and high demand for precision operation in SIL-TEP. Indeed, the more complex a procedure the more likely it will have an impact on surgeon fatigue which may affect surgical time. Operation time can also be influenced by hernia sac size; large sacs require more extensive dissection than smaller sacs and may increase the likelihood of hematoma formation. Importantly, we observed surgery duration was more significantly influenced by hernia diameter in the SIL-TEP group compared with the TEP group. However, only one hematoma complication occurred in both groups. This finding suggests that despite increased operation time in managing large hernias, the safety of the SIL-TEP procedure was maintained.
Previous studies have shown that for surgeons proficient in TEP, a significant reduction in operation time, without increasing the risk of complications or hernia recurrence, can be achieved after approximately 30–80 cases.18–21 However, the SIL-TEP procedure demands high surgical skills, anatomical knowledge, and spatial awareness from the surgeon, and so steepens the learning curve. Nevertheless, for an experienced laparoscopic surgeon, it has been estimated that the learning curve for SIL-TEP can be effectively overcome after approximately 60 cases, reducing the operation time to <60 minutes. 5 The same study showed that proficiency can be achieved after 85 cases, stabilizing the operation time to approximately 35 minutes. 5 These findings suggest that limitations of the SIL-TEP procedure can be effectively overcome by experienced surgeons, achieving efficiency comparable to TEP surgery.
Consistent with findings from a previous study, we found that the SIL-TEP group exhibited significantly lower postoperative pain scores on Day 1 and significantly shorter times to resume normal activities than the TEP group. 22 We suggest that this finding is due to the SIL-TEP procedure only involving only a 2.5-cm incision at the umbilicus, which provided an excellent field of vision for our surgeons. The manoeuvre allowed the surgeon to align the abdominal wall fascia and connective tissue during suturing. Importantly, the fewer and shorter total incisions contribute to less early postoperative pain and quicker recovery. However, in later follow-ups, we observed more patients complaining of groin rather than incisional pain, with no significant difference in pain intensity. This finding suggests that mesh type or fixation method may influence long-term pain more. Similarly, several studies have shown comparable pain scores for incisional pain after seven days and longer, leading us to conclude that SIL-TEP offers no significant advantage over TEP in postoperative pain.23–26
In assessing postoperative cosmetic outcomes, no significant difference in patient satisfaction was observed between the groups. This finding was surprising, but may reflect the prevalence of inguinal hernias in our population of mainly elderly men, who generally have low concerns about postoperative scar appearance and tend to prioritize clinical efficacy and complication rates as being more important. While some studies have found significant improvements in cosmetic satisfaction between single-port versus conventional laparoscopic TEP inguinal hernia repair, these results were achieved with relatively small sample sizes, and so the generalizability of their conclusions is limited.8,18,22 A systematic review and meta-analysis of 10 trials involving over 1000 patients, found SIL-TEP did not significantly outperform TEP with regard to postoperative cosmetic satisfaction. 27
In view of the acknowledged technical challenges and steep learning curve associated with SIL-TEP hernia repair, some surgeons have questioned its safety. 17 Nevertheless, our study found no significant differences in early or late perioperative complications, intraoperative blood loss, conversion rates, or postoperative hospital stay between the two surgical groups, and there were no significant incidents of severe complications such as excessive bleeding or hernia recurrence. These findings align with those from previous meta-analyses, suggesting similar surgical safety and clinical outcomes are achieved for both procedures, and reinforce the rationale of SIL-TEP as a minimally invasive surgical option.6,27,28
Although the SIL-TEP technique increases surgical difficulty and duration, we believe that these factors are within manageable limits and do not negatively impact surgical outcomes. Therefore, the SIL-TEP procedure could be used by patients who desire reduced abdominal wall trauma and request improved postoperative aesthetics. However, we acknowledge that a large incision at the umbilicus in single-port laparoscopy, might increase the risk of incisional hernias. Due to the short follow-up period, we could not draw definitive conclusions on this probability, and there is limited published literature that has addressed this issue, highlighting the need for further research. Importantly, an unavoidable drawback of SIL-TEP is its higher medical cost than TEP, because it requires single-port cannulas and specialized instruments. According one study, the use of the Triport single-port access device led to an additional cost of $480 per patient. 24 Therefore, some surgeons opt for homemade single-port devices to reduce costs.22,25,26 As mentioned earlier, we used a homemade glove port to mitigate costs, but this increased our surgical difficulties due to its material limitations.
Our study had several limitations, including a small number of cases, a short follow-up duration, and lack of investigation into the learning curve for the SIL-TEP procedure. Our findings that the operation times for the SIL-TEP group were longer than TEP group, suggests that our surgeons may have not fully mastered the technique and may have been in the early phase of the learning curve, potentially biasing the accuracy of our results. Moreover, we did not conduct an in-depth analysis of different types of hernias, including recurrent, incarcerated, or narrow. Therefore, further studies are required to investigate the efficacy and safety of the SIL-TEP technique in these specific types of hernias.
In conclusion, while the SIL-TEP procedure is more challenging than the TEP procedure for hernia repair, we found that at our centre it is comparable with regard to overall safety and feasibility. We also found that cosmetic outcomes and postoperative pain control were not superior to TEP. Further studies are needed to validate our findings.
Supplemental Material
sj-pdf-1-imr-10.1177_03000605241257418 - Supplemental material for Single-port versus traditional three-port laparoscopic total extraperitoneal inguinal hernia repair: A single-centre, prospective, randomised study
Supplemental material, sj-pdf-1-imr-10.1177_03000605241257418 for Single-port versus traditional three-port laparoscopic total extraperitoneal inguinal hernia repair: A single-centre, prospective, randomised study by Xuen Li, Xufeng Hu, Yue Hu and Yuan Jie in Journal of International Medical Research
Footnotes
Acknowledgment
We thank Dr. Kevin Li for editorial assistance.
Declaration of conflicting interests
The authors declare that there are no conflicts of interest.
Funding
The study was supported by Cixi Agricultural and Social Development Science and Technology Program (CN2022013) and Cixi Public Welfare Science and Technology Program (N2022013).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.