
Abstract
Objective
This study sought to examine the relationship between exposure to different types of workplace dust (mineral dust, organic dust, exhaust fumes, and other fumes) and the prevalence of asthma in a nationally representative sample of the population in the United States.
Methods
Using data from the National Health and Nutrition Examination Survey 2007–2012, we analyzed data of 16,841 participants after exclusions based on specific criteria. Logistic regression models were used to evaluate the association between dust exposure and asthma prevalence after adjusting for demographic and health-related covariates.
Results
Our findings indicate that exposure to various types of dust is positively associated with the prevalence of asthma. This association remained significant after adjusting for age, sex, race, and other covariates. Notably, subgroup analysis revealed that females are more susceptible to asthma from dust exposure than males. In addition, individuals with higher body mass index and older age are more likely to have asthma due to dust inhalation.
Conclusion
This study underscores the need for targeted occupational health interventions and policies, especially for high-risk groups such as females, those with higher body weight, and older individuals. Further longitudinal studies are recommended to establish causal relationships.
Keywords
Introduction
Occupational dust exposure is a significant public health issue in modern industrial societies, 1 and its effects on respiratory health have been a prominent focus of research. 2 Many types of workplace dust, including mineral dust, organic dust, exhaust fumes, and other fumes, have been recognized as potentially increasing the risk of respiratory disease.3–5 Asthma, a persistent respiratory condition that affects a significant portion of the global population, is characterized by airway inflammation and hyperresponsiveness, resulting in breathlessness, chest tightness, and coughing. 6
Although research has demonstrated a link between dust exposure and asthma in particular industries (e.g. mining, textiles, and construction), these studies have typically been limited to specific occupational settings and small sample sizes.3–5,7,8 As a result, a broadly representative sample is lacking to explore whether this association can be generalized to a broader variety of work settings. In addition, how sex, age, ethnicity, body mass index (BMI), presence of cancer, and presence of heart disease affect the increased risk of asthma due to occupational dust exposure remains understudied.
Drawing on data from the 2007–2012 National Health and Nutrition Examination Survey (NHANES), which included 16,841 adults in the United States, this study explored the correlation between the inhalation of different types of dust in the work environment and the prevalence of asthma. Through detailed statistical analysis, the study aimed to inform occupational health policy and support the creation of preventive strategies.
Methods
Description of the survey
Data were sourced from NHANES, a population-based, cross-sectional study designed by the National Center for Health Statistics to assess the health and nutritional status of individuals across the United States. NHANES uses a complex, multistage, stratified probability sampling method conducted biennially to yield a representative sample. 9
The study’s protocols were approved by the National Heart, Lung, and Blood Institute’s ethics review board. Informed consent was obtained from all adult participants or from parents or legal guardians of individuals aged ≤16 years. Comprehensive NHANES study protocols and data are publicly accessible at www.cdc.gov/nchs/nhanes.
Study population
This study focused on the 2007–2012 NHANES survey cycle because it included complete surveys of mineral dust, organic dust, exhaust fumes, and other fumes.
Initially, 30,442 participants were considered; however, 13,586 individuals were excluded due to providing a response of “Refused,” “Don’t know,” or “Missing” for the following four questions: 1. “Ever had work exposure to mineral dust?”; 2. “Ever had work exposure to organic dust?”; 3. “Ever exposed to exhaust fumes at work?”; or 4. “Ever had work exposure to other fumes?.” In addition, 15 participants who answered “Refused” or “Don't know” to the question “Ever been told you have asthma?” were also excluded. Participants excluded due to incomplete exposure or outcome information did not differ significantly from those included in terms of demographic characteristics. Finally, 16,841 participants were included in the analysis (Figure 1).
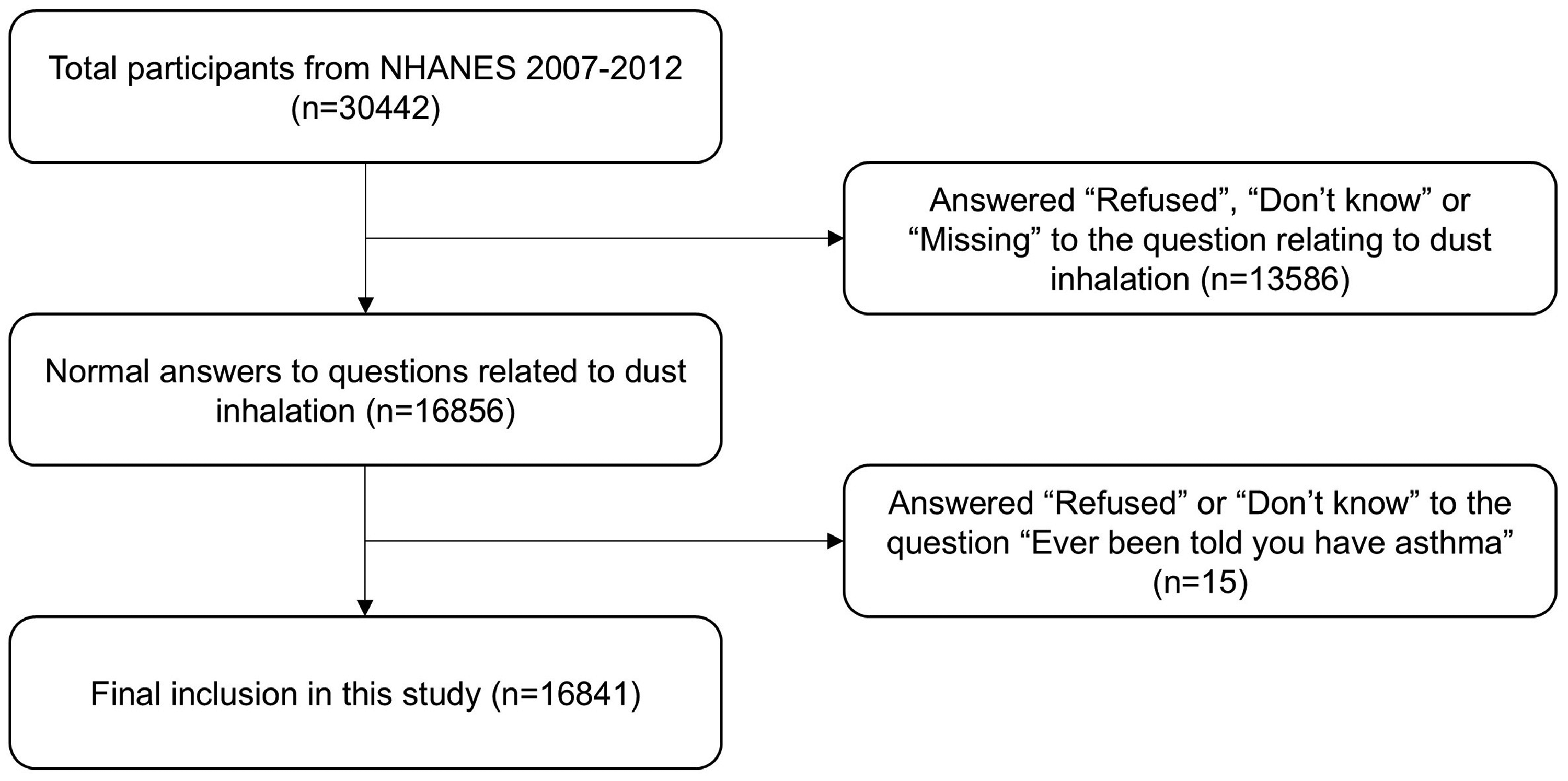
Flow chart. NHANES: National Health and Nutrition Examination Survey.
Definition of various types of dust inhalation and asthma
The authors defined the answer “Yes” to the questions “Ever had work exposure to mineral dust?,” “Ever had work exposure to organic dust?,” “Ever exposed to exhaust fumes at work?” and “Ever had work exposure to other fumes?” as having inhaled the corresponding dust/fumes and the answer “No” as not having inhaled the corresponding dust/fumes.
Answering “Ever been told you have asthma?,” with “Yes” was defined as having asthma and “No” was defined as not having asthma. 10 Inhalation of various types of dust was designated as the exposure variable, whereas the presence of asthma was designated as the outcome variable.
Selection of covariates
Covariates in this study included sex (male/female), age (year), race (Mexican–American/other, Hispanic/non-Hispanic, White/non-Hispanic, and Black/other race), educational attainment (Less than 9th grade, 9th–11th grade, 12th grade with no diploma, High school graduate, GED or equivalent, and some college or AA degree/college graduate or above), BMI (kg/m2), marital status (married/unmarried), poverty index ratio (PIR), the number of years of inhalation of various types of dust, presence of heart disease (yes/no), and presence of cancer (yes/no). Of these, “Married” and “Living with partner” were categorized as “Married.” “Widowed,” “Divorced,” “Separated,” and “Never married” were categorized as “Unmarried” based on the participant’s current marital status. Detailed procedures for measuring these variables are publicly accessible at www.cdc.gov/nchs/nhanes.
Statistical analyses
This study was conducted and reported in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines for cross-sectional studies.
Statistical analyses followed the Centers for Disease Control and Prevention guidelines, considering the complex, multistage cluster design of NHANES. Continuous variables are presented as means and standard deviations, whereas categorical variables are shown as proportions. Differences among age quartiles were evaluated using weighted Student’s t-tests for continuous variables and weighted chi-square tests for categorical variables. The association between asthma and workplace dust exposure was examined using multivariate logistic regression, treating dust exposure as a dichotomous variable across three models. Model 1 included no covariate adjustments. Model 2 was adjusted for sex, age, and race. Model 3 included adjustments for sex, age, race, duration of dust exposure, education level, marital status, BMI, and presence of heart disease and cancer, which may influence immune and inflammatory pathways relevant to asthma. Additionally, analyses were conducted within subgroups (sex, age, race, BMI, heart disease, and cancer) to explore potential heterogeneity in the associations. Missing values for continuous variables with skewed distributions, such as PIR, were imputed using the median. For categorical variables, including education level, marital status, race/ethnicity, and comorbidities (cancer and heart disease), multiple imputation by chained equations was performed to account for missingness, generating five imputed datasets. The primary exposure variables (types of dust) and the outcome variable (asthma status) were not imputed. Participants with missing data for these key variables were excluded from the analysis. Empower software (www.empowerstats.com; X&Y Solutions, Inc., Boston, Massachusetts, USA) was used for all analyses, with statistical significance set at P < 0.05. Each type of dust exposure was treated as an independent binary variable and included in separate models, followed by a joint model to account for potential coexposures.
Results
Baseline characteristics of participants
As shown in Table 1, the study included 16,841 participants (mean age, 45.6 ± 17.5 years), of whom 50.7% were male and 49.3% were female. The overall prevalence of asthma among all participants was 14.6%. Compared with individuals without asthma, those with asthma were more likely to be female, younger, and of Black or Mexican–American ethnicity (P < 0.001). Participants with asthma had higher exposure rates to mineral dust (32.0% vs. 30.7%), organic dust (23.8% vs. 21.5%), exhaust fumes (25.1% vs. 23.4%), and other fumes (33.8% vs. 30.5%) than those without asthma (P < 0.05). Additionally, asthma was significantly associated with shorter exposure durations for each dust type, higher BMI, lower PIR, lower education level, lower marriage rate, and higher prevalence of cancer and heart disease (P < 0.001 for all). No significant difference was observed in the proportion of participants with college education across asthma groups (P > 0.05).
Baseline characteristics of the study population according to asthma status.

BMI: body mass index; PIR: poverty income ratio.
The unadjusted, incompletely adjusted, and adjusted models for the inhalation of different dust types and prevalence of asthma are shown in Table 2. In the unadjusted model, the inhalation of metallic dust (odds ratio (OR) = 1.06; 95% confidence interval (CI): 0.97–1.17), organic dust (OR = 1.14; 95% CI: 1.03–1.26), exhaust fumes (OR = 1.09; 95% CI: 0.99–1.21), and other dust (OR = 1.17; 95% CI: 1.06–1.28) was positively associated with asthma prevalence. After adjusting for covariates, all four variables—metal dust (OR = 1.24; 95% CI: 1.12–1.37), organic dust (OR = 1.18; 95% CI: 1.06–1.31), exhaust gases (OR = 1.21; 95% CI: 1.09–1.35), and other dust (OR = 1.24; 95% CI: 1.12–1.36)—reached statistical significance in the fully adjusted model (P < 0.05).
Prevalence of asthma and dust inhalation.

Model 1: no covariates were adjusted. Model 2: adjusted for age, sex, and race. Model 3: adjusted for age, sex, race, years of inhalation of various types of dust, body mass index, poverty index ratio, education, marital status, cancer prevalence, and heart disease.
CI: confidence interval; OR: odds ratio.
Subgroup analysis
In subgroup analyses, we investigated the association between dust inhalation status and asthma prevalence in terms of sex, age, ethnicity, BMI, presence of cancer, and presence of heart disease. Interaction tests only showed the effect of sex (P for interaction = 0.0429, 0.0226, 0.0103, and 0.0003) and racial groups that inhaled exhaust fumes (P for interaction = 0.0080) on the relationship between various types of dust inhalation and asthma prevalence. However, these tests did not show the effect of BMI, age, racial groups with no inhalation of exhaust fumes, presence of cancer, and presence of heart disease on the relationship between various types of dust inhalation and asthma (all P for interaction >0.05) (Figure 2).

Subgroup analysis. BMI: body mass index.
Discussion
Based on data from the NHANES 2007–2012, which surveyed 16,841 participants, this study examined the relationship between the inhalation of various types of dust in the work environment and the prevalence of asthma. This study found that the inhalation of mineral dust, organic dust, exhaust fumes, and other fumes were positively associated with the prevalence of asthma. These associations remained significant, particularly after adjusting for covariates such as age, sex, and race. Notably, the subgroup analyses showed that women were more susceptible than men to asthma due to the inhalation of various types of dust. In addition, people with higher body weight and older age demonstrated a greater likelihood of having asthma due to the inhalation of dust. In the subgroup analyses on race, the prevalence of asthma after dust inhalation was higher for other races, 11 likely influenced by occupational exposure type and duration of dust inhalation. No significant interaction was observed in the cancer and heart disease subgroups, possibly due to limited statistical power from small sample sizes. The wide and overlapping CIs in these groups may have masked potential associations. Interestingly, the association between dust and fume inhalation and asthma remained significant only in individuals without cancer or heart disease. This may be because of immune dysregulation or altered airway physiology in individuals with chronic comorbid conditions, which could affect both asthma susceptibility and diagnostic patterns.
Previous studies have focused on the respiratory effects of dust exposure in specific industries (e.g. mining, textiles, and construction).12–16 For example, one study showed a significant increase in the prevalence of asthma among workers working near the Sohar industrial port in Oman 17 ; another study showed that the prevalence of quartz, asbestos, and dust inhalation was 3.7%, 5.0%, and 28.3%, respectively. 18 Although this study did not assess asthma or respiratory outcomes directly, it provides useful background information on the extent of exposure in industrial environments. A study published in 2022 by D’Antona et al. 12 points to a causal relationship between a dustier workplace and asthma. A 1999 population-based case-extrapolation study in Sweden found that occupational exposure to acrylate compounds and welding fumes was associated with an increased risk of asthma in adults. 19 Those studies corroborate the results of our statistical analysis of the relationship between the inhalation of various types of dust and asthma. Zhang et al. 20 conducted a nationally representative cross-sectional study showing that women were more susceptible to asthma than men. Additionally, a retrospective and cross-sectional study by Kim et al. 21 revealed that obese individuals were more likely to be diagnosed with persistent asthma than non-obese individuals (OR = 1.50; 95% CI: 1.10–2.05). Older individuals are generally expected to have longer cumulative exposure to dust, which may contribute to the higher prevalence of asthma observed in this group. These findings are consistent with the results of our subgroup analyses by sex, BMI, and age. However, contrary to expectations, participants with asthma in our sample had shorter average exposure durations. This inverse relationship may be explained by the fact that individuals who developed asthma earlier were more likely to change jobs or avoid further exposure. This phenomenon highlights the complexity of exposure–outcome relationships in occupational settings. Previous studies had relatively small sample sizes and focused on limited types of dust exposure.22–24 In contrast, our study covered more types of dust and had a larger sample size, making the results more representative and generalizable.
Increased asthma prevalence may be related to the inflammatory response in the airways following dust inhalation, in which dust particles stimulate the production of inflammatory mediators in the airways, leading to increased airway hyperresponsiveness. 25 Additionally, the sex differences observed in this study may be attributable to inherent biological variations, such as disparities in lung anatomy and immune response. 26 A survey on occupational asthma conducted in São Paulo from 1995–2000 showed that occupational exposure in both men and women may also be responsible for the higher probability of asthma in women. 27 Harvey et al. 28 suggested that estrogen exacerbates asthma in several ways. Previous research has shown that individuals with a higher body weight exhibit a greater prevalence of asthma than those with a lower body weight, which may be related to airway inflammation and airway hyperresponsiveness due to obesity. 29 A study by Mendes et al. 30 from Portugal demonstrated that varying degrees of immune response led to obesity as a significant risk factor for asthma and emphasized that obesity complicates the treatment of asthma, affecting its progression, clinical manifestations, and management. Jensen et al. 31 showed that children with a genetic predisposition to higher BMI had an increased risk of severe wheezing.
This study has several strengths. First, the authors used NHANES data, and all analyses incorporated the appropriate sampling weights to enhance the representativeness of the study sample. Multiple covariates were included to improve the accuracy and reliability of the findings, and subgroup analyses were performed to better understand population differences. In addition, the large sample size provides a nationally representative view of the United States and has a high degree of extrapolation of results. The first nationwide survey for this research topic was conducted to provide basic data and references for subsequent studies. This study also had the following shortcomings. The cross-sectional design restricts the ability to explore causal relationships between dust inhalation and asthma. Specifically, we could not determine whether dust or fume exposure preceded the onset of asthma or occurred afterward, limiting the ability to infer temporal directionality. Although multiple covariates were considered, it was not possible to rule out the effects of all the potential confounders. Additionally, because of limitations in the NHANES dataset, we were unable to classify asthma cases by phenotype (e.g. allergic vs. nonallergic), which may affect the interpretation of exposure–outcome associations. We also did not perform stratified analyses by years of dust exposure duration, which may influence the observed associations. Future studies should consider categorizing exposure duration to assess potential dose–response relationships.
Conclusions
This study revealed a significant association between inhalation of various types of dust in the work environment and an increased prevalence of asthma. Specifically, the inhalation of mineral dust, organic dust, exhaust fumes, and other fumes was positively correlated with a higher asthma prevalence, with adjusted ORs indicating a robust and statistically significant relationship. Notably, subgroup analysis indicated that women were more vulnerable to having asthma from dust inhalation than men, which may be attributed to differences in lung anatomy, immune response, estrogen levels, and patterns of occupational exposure. Additionally, individuals with high body weight were more susceptible to asthma than individuals with low body weight, which may be related to obesity-induced airway inflammation and airway hyperresponsiveness. Older people are more likely to have asthma after dust inhalation than younger people, probably because the average number of years of dust inhalation is higher in older age groups.
Footnotes
Acknowledgments
We would like to express our sincere gratitude to Prof. Yonghuai Li for his valuable guidance and expertise in the statistical analysis of this study. His insights and support greatly contributed to the rigor and accuracy of our data interpretation.
Author contributions
Conceived the study and provided funding: Yonghuai Li.
Collected and analyzed the data: Yi Dai.
Wrote the first draft of the manuscript: Yi Dai.
Made critical revisions and approved the final version: All authors.
Agreed with the manuscript results and conclusions: All authors.
All authors reviewed and approved the final manuscript.
Data availability statement
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Funding
This work was supported by the Anhui Natural Science Foundation (2108085QH315) as well as the National Natural Science Fund of China (81870519, 81870787, and 81800815).