
Abstract
Objective
The purpose of this retrospective observational study was to assess the feasibility of electrodiagnostic parameters, perioperatively, and to discover optimal values as prognostic factors for patients with brachial plexus injury undergoing nerve transfer operations.
Methods
We retrospectively reviewed the records of 11 patients who underwent nerve transfer surgery. The patients underwent perioperative electrodiagnosis (EDX) before and approximately 6 months after surgery. We evaluated the compound muscle action potential (CMAP) ratio, motor unit recruitment, and their interval changes. To evaluate motor strength, we used the Medical Research Council (MRC) grade, 6 and 12 months after surgery. We evaluated the relationships between improved CMAP ratio, and motor unit recruitment and MRC grade changes 6 and 12 months postoperatively.
Results
All parameters increased significantly after surgery. The CMAP ratio improvement 6 months after surgery correlated with the MRC grade change from baseline to 12 months, with a correlation coefficient of 0.813.
Conclusion
EDX parameters improved significantly postoperatively, and the CMAP ratio improvement 6 months after surgery correlated with the clinical outcomes at 1 year. The results of perioperative EDX might help establish long-term treatment plans for patients who undergo nerve transfer surgery.
Keywords
Introduction
Brachial plexus injury (BPI) is catastrophic regarding upper extremity motor function. Muscle strength for shoulder abduction or elbow flexion is important in activities of daily living (ADLs), and BPI makes ADLs difficult by weakening these muscles.1–4 Early and precise diagnosis, treatment, and rehabilitation are important for recovering movement.
Even with the various methods that are used to treat patients with BPI, including rehabilitation or a prosthesis, surgeries, such as nerve grafting and nerve transfer procedures, are the most effective and widely used treatments.1,5–9 Conventionally, after nerve exploration to evaluate the root stump, nerve repair with or without grafting is performed if the root is available, and nerve transfer is performed if a definite preganglionic lesion, such as root avulsion, is present. Recently, with the reported effectiveness of nerve transfer, there have been attempts to perform nerve transfer without exploration.6,10,11 Several donor and recipient nerves, such as the axillary, musculocutaneous, and suprascapular nerves, can be used in nerve transfer surgery and lead to functional recovery.7–9,12
A long-term follow-up of at least 12 months is needed to evaluate the clinical functional outcomes after nerve transfer surgery.6,11 Because of the long time interval between surgery and when measurable clinical outcomes can be observed, there is an emerging need to identify suitable tools that can be used to evaluate recovery in the early postoperative period. Age, body mass index, time from injury to surgery, and various electrodiagnostic parameters of the donor nerve have been identified as potential prognostic factors; however, further studies are needed to confirm these findings.3,13
Electrodiagnosis (EDX), involving nerve conduction study (NCS) and electromyography (EMG), can be used to evaluate nerve function. EDX can also be used to evaluate the degree of regeneration or clinical outcomes in peripheral nerve injuries. Several attempts have been made to evaluate the prognostic potential of EDX parameters in various peripheral nerve injuries, including BPI.3,13–16 To the best of our knowledge, previous studies performed EDX only once, and no study has attempted to correlate the preoperative and postoperative EDX findings with clinical outcomes.3,17 Considering these issues, this study aimed to first assess the feasibility of comparing preoperative and postoperative EDX findings and clinical function, and second, to evaluate the changes in the preoperative and early postoperative EDX parameters as potential prognostic factors in patients with BPI who have undergone nerve transfer surgery.
Materials and methods
Patient selection and surgical procedure
The Institutional Review Board of the Asan Medical Center approved the study protocol (approval number: 2020-1405). We retrospectively reviewed the medical records of 11 patients diagnosed with BPI at any level who underwent nerve transfer surgery involving at least one suprascapular, musculocutaneous, or axillary nerve between May 2017 and April 2019 at a single center. Only one patient underwent surgery targeting the median and ulnar nerves. All patients provided written informed consent before undergoing the surgery. The target nerves contributed to at least one movement involving shoulder abduction, elbow flexion, or pinch grip strength. Staged operations were performed in some patients at intervals of 1 to 2 weeks, and vascularized ulnar, dorsal cutaneous ulnar, or lateral antebrachial nerve grafts were used, if needed. The eligibility criteria were patients with BPI caused by trauma confirmed in both the clinical history and preoperative EDX who underwent nerve transfer in a single center, who underwent postoperative EDX and routine outpatient follow-up for at least 1 year, and who were not diagnosed with other diseases that could affect their functional status, such as peripheral neuropathies. We have de-identified all patient details. This study was performed in compliance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines.
EDX data
All patients underwent preoperative and postoperative NCS and EMG in a single center. The majority of the patients had undergone follow-up EDX once within 6 months after surgery. The radial, ulnar, median, musculocutaneous, axillary, and suprascapular nerves were tested in the NCS. One of the innervated muscles was selected to test each nerve as follows: extensor indicis proprius (EIP) for the radial nerve, abductor digiti minimi for the ulnar nerve, abductor pollicis brevis for the median nerve, biceps brachii for the musculocutaneous nerve, deltoid for the axillary nerve, and supraspinatus or infraspinatus for the suprascapular nerve. All patients underwent NCS with the same test protocol in a single laboratory. The compound muscle action potential (CMAP) ratio was defined as the target nerve CMAP to that of the same nerve on the contralateral side; this ratio was rounded to two decimal places. Both preoperative and postoperative CMAP ratios were calculated, and the postoperative ratio was subtracted from the preoperative ratio to estimate the improvement for each nerve. If two or more nerves were tested, we used average values to calculate the CMAP ratio. The suprascapular nerve was not routinely evaluated, even when it was the target nerve of the nerve transfer. In some cases, not every nerve that was transferred was tested; only tested nerve parameters were evaluated.
EMG was performed in the same muscles as for NCS, except for the extensor carpi radialis longus muscle, which was used to test the radial nerve instead of the EIP. We divided the motor unit recruitment patterns into four stages, with 0 implying no recruitment, 1 as single, 2 as decreased, and 3 as normal. 18 If two or more muscles were tested, we used the same protocol that we used to calculate the CMAP ratio. We evaluated the motor unit recruitment according to whether the recruitment pattern showed improvement between the preoperative and postoperative measurements to evaluate the relationship between the motor unit recruitment and Medical Research Council (MRC) grade changes.
Clinical data
In either the inpatient or outpatient orthopedic clinic, we tested the motor strength of shoulder abduction, elbow flexion, and pinch grip before the operation and again 6 and 12 months after surgery. All the tested muscles were evaluated by the MRC scale for muscle strength and were recorded in the electronic medical record (EMR) system. The motricity index was calculated afterward according to the EMR. 4 If two or more nerves were tested, an average MRC and motricity index for all nerves was calculated at each time point.
Statistical analyses
Owing to the small sample size, nonparametric tests were used for data analysis. The preoperative and postoperative changes in the CMAP ratio, motor unit recruitment, MRC grade, and motricity index were evaluated by the Wilcoxon signed-rank test. The MRC grade and motricity index changes were evaluated between preoperative, and 6- and 12-month postoperative scores. The correlations between the CMAP ratio difference, MRC grade change, and motricity index change were evaluated by Spearman’s correlation. Each correlation for CMAP ratio difference, MRC grade, and motricity index was also tested for changes at 6 and 12 months. Motor unit recruitment and MRC grade were divided into two groups by the presence or absence of improvement, and a 2 × 2 table was created. Fisher’s exact test was performed for comparisons between groups. Descriptive statistics were calculated for demographic variables, time from injury to surgery, time from injury to preoperative EDX, and time from surgery to postoperative EDX. A p-value <.05 was considered statistically significant. All statistical analyses were performed using PASW Statistics for Windows, Version 18.0 (SPSS Inc., Chicago, IL, USA).
Results
Patient characteristics
Between May 2017 and April 2019, a total of 25 patients with BPI underwent nerve transfer surgery. Fourteen patients did not meet the inclusion criteria, and 11 patients were included. The mean patient age was 37.5 years, and all patients were men (Table 1). The mean time interval from injury to surgery was 192 (range, 110–264) days. The mean time interval from surgery to postoperative EDX was 213 days. All patients underwent postoperative EDX within 200 days, except for two patients who underwent EDX at approximately 1 year.
Demographic characteristics of the patients.
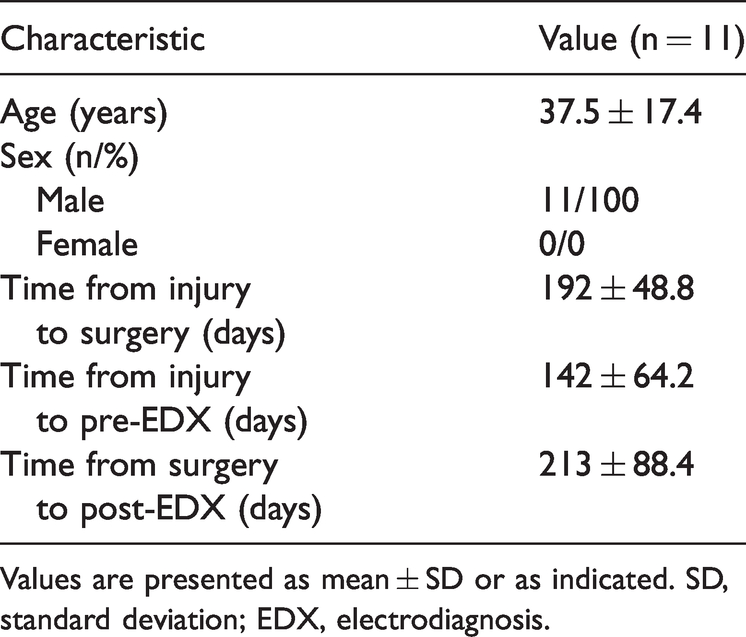
Values are presented as mean ± SD or as indicated. SD, standard deviation; EDX, electrodiagnosis.
The surgery details for individual patients are shown in Table 2. Nerve transfer surgery was performed in all patients, and five patients had additional surgery, such as sural nerve graft, neurolysis, or ulnar nerve anterior transposition. Ten patients underwent nerve transfer targeting more than one nerve.
Surgical characteristics of the patients.

*If multiple nerves were tested, the average value was used. Op., operation; SA, spinal accessory nerve; SS, suprascapular nerve; MC, musculocutaneous nerve; FCU, flexor carpi ulnaris; FCR, flexor carpi radialis; APB, abductor pollicis brevis; FDI, first dorsal interosseous; BB, biceps brachii; ECRL, extensor carpi radialis longus.
Changes after surgery
The CMAP ratio, motor unit recruitment, MRC grade, and motricity index increased significantly between the preoperative and postoperative measurements in all patients. Raw data for individual patients are described in Table 3, and the exact mean values are presented in Table 4. MRC grade and motricity index compared between baseline and 6 months postoperatively and between baseline and 12 months postoperatively increased significantly in all patients.
Raw data for the electrodiagnostic parameters, muscle strength, and time intervals.

*If multiple nerves were tested, the averaged value was used.
Op., operation; SA, spinal accessory nerve; SS, suprascapular nerve; MC, musculocutaneous nerve.
EDX parameters and clinical outcome changes pre- and postoperation.

Values are presented as mean±SD or as indicated.
*p<.05, by Wilcoxon’s signed rank test of pre- versus postoperative data.
Op., Operation; CMAP, compound muscle action potential; MRC, Medical Research Council; Preop, preoperative; Postop, postoperative; SD, standard deviation.
Correlation between EDX data and clinical outcome
The correlations between the CMAP ratio change, MRC grade change, and motricity index change are shown in Figures 1 and 2. Figure 1 shows the relationship between the CMAP ratio and MRC grade change from baseline to 6 months and 12 months postoperatively.

Relationship between CMAP ratio improvement and MRC grade change. The p-value by Spearman’s correlation between CMAP ratio improvement 6 months postoperatively and MRC grade changes 6 and 12 months postoperatively. The improvement in the CMAP ratio for early postoperative EDX and 12-month MRC grade change were significantly correlated (three points at 0,0 overlapped in the 6-month graph, and two points at 0,0 overlapped in the 12-month graph).

Relationship between CMAP ratio improvement and motricity index change. The p-value by Spearman’s correlation between CMAP ratio improvement 6 months postoperatively and motricity index changes 6 and 12 months postoperatively (two patients were excluded from the analysis at 6 months owing to missing data, and two points at 0,3 overlapped in the 12-month graph).
Two patients underwent postoperative EDX after 1 year; therefore, these patients were excluded from the 6-month evaluation. The CMAP ratio difference and 12-month MRC grade change were significantly correlated, with a Spearman’s correlation coefficient of 0.813. Figure 2 shows the correlation between the CMAP ratio difference and motricity index change; the correlation was not significant.
The relationship between recruitment pattern improvement and MRC grade change is shown in Table 5, and no statistically significant correlations were seen.
Relationship between MRC grade and motor unit recruitment change

MRC, Medical Research Council.
Discussion
To the best of our knowledge, this study was the first attempt to estimate the feasibility of using the CMAP ratio to predict postoperative clinical outcomes. All outcomes measured in our study improved significantly after surgery, and the CMAP ratio difference correlated with clinical improvement in MRC grade 1 year postoperatively. Motor unit recruitment, which was identified as a prognostic factor in other studies, was not statistically significant, in our study. 17
The MRC grade and motricity index measured 6 months and 1 year after nerve transfer operation improved significantly. The timing of clinically observable motor recovery after surgery varied depending on the surgical technique and which nerves were selected, in previous studies. Leechavengvongs et al. 11 reported that MRC grade 2 deltoid muscle recovery appeared 6 to 8 months after nerve transfer from the triceps long head branch to the target deltoid. Because of the axonal regeneration rate of 1 mm per day, up to 2 years are required to identify meaningful recovery after proximal nerve reconstruction. 6 The changes in MRC grade and motricity index 1 year postoperatively in our study corresponded with these findings, and clinical outcomes at 6 months improved significantly compared with findings at baseline. These findings likely resulted from additional neurolysis or transposition for a possible demyelinating component in injury, and natural recovery over time during the interval from trauma to surgery in some patients. 19
Various studies have demonstrated the potential of using EDX parameters as prognostic factors for peripheral neuropathies. In particular, attempts to use parameters, such as CMAP amplitude and ratio, as factors to predict clinical outcomes, have been reported for a variety of neuropathies.14,16,20,21 Heise et al. 22 concluded that the CMAP ratio measured in 25-day-old infants with obstetrical plexopathy could be used as a prognostic assessment to predict motor function at 6 months. Similarly, the current study identified a correlation between CMAP ratio improvement and the MRC grade change at 12 months. Considering that axonal regeneration occurs after nerve transfer surgery, the recovery timing and prognosis could also be estimated using the CMAP ratio, which is used to evaluate peripheral nerve injuries.8,23 Thus, improved EDX parameters at 6 months, especially the CMAP ratio, could suggest successful ongoing regeneration, and active rehabilitation should be encouraged to maximize the long-term outcomes of the procedure.24,25
We did not identify a meaningful relationship between the CMAP ratio difference and clinical outcomes change at 6 months. Some patients showed definite improvement in the CMAP ratio without observable motor strength at 6 months. In these cases, it is possible that the degree of muscle fiber reinnervation was insufficient to elicit clinical motor function, but was sufficient to show CMAP ratio improvement. However, one patient showed improved motor function compared with baseline without a CMAP ratio change. Considering the speed of axonal regeneration, motor strength could be overestimated owing to synergic patterns when patients are tested in an outpatient setting.
None of the motricity index changes measured at 6 and 12 months correlated with CMAP difference ratios, in this study. To promote critical motor functions in ADLs, additional procedures have been occasionally performed with nerve transfer in patients with BPI.6,26 We investigated whether we could predict a more comprehensive outcome for the entire operation by evaluating changes in partial nerves, and we found no significant associations. This might be attributed to the varying severity of injury and heterogeneity of donor and recipient nerves. Additionally, the limited evaluation of transferred nerves made it difficult to investigate outcomes.
EMG parameters are correlated with clinical function, and there have been several attempts to use EMG parameters as prognostic factors for peripheral nerve injuries.27–29 The grade of motor unit recruitment, an EMG parameter, reflects the severity of axonal loss and the degree of intact axon preservation. Impastato et al. 17 reported that the degree of motor unit recruitment correlated with spontaneous motor recovery in patients with BPI. In contrast, we did not identify a significant relationship between the improvement in motor unit recruitment and MRC grade. However, our findings may not reflect the true relationship between motor unit recruitment and motor recovery owing to the small sample size and the subjective nature of motor recovery evaluations. 30 Improvements in the MRC grade were observed in all patients with better postoperative motor unit recruitment patterns, which may indicate that some relationship between these events does exist. A larger study is needed to evaluate this relationship more closely.
There are limitations to this investigation. First, the recipient nerves were heterogenous and not fully evaluated, which could influence the reliability of this study. A follow-up study with a more precise subgroup analysis would be helpful. Second, although we tried to conduct postoperative studies at the same time, two patients underwent EDX approximately 1 year after surgery, and results could be overestimated owing to that time course. Third, although every effort was made to decrease variability between evaluators, interobserver variability is possible. Fourth, the outcome measure time was relatively short compared with that in other studies evaluating BPI, although we usually evaluated the biceps brachii and deltoid, which are proximal to the operation sites. Additional time points should be added in a follow-up study. Finally, a relatively small sample size made it difficult to control for variables, such as additional procedures or the exact timing of EDX.
In conclusion, EDX showed significant changes after surgery, and the differences in the CMAP ratio correlated with the clinical outcomes at 1 year of follow-up. The results of preoperative and early postoperative EDX might help establish long-term treatment plans for patients with BPI who undergo nerve transfer surgery. Further studies are required to confirm our results in a larger population.