
Abstract
Introduction
White blood cell count, a cost-effective blood test marker, is used extensively for the diagnosis and prognosis of diseases. Nevertheless, its association with the progression and prognosis of acute kidney injury remains unclear.
Methods
A retrospective analysis was conducted using data from a multicenter randomized trial on an acute kidney injury early warning system. Univariate analysis, multivariate logistic regression, and smooth curve fitting were used to evaluate the association between the white blood cell count and the progression and prognosis of acute kidney injury.
Results
A total of 5471 patients were included in the study. White blood cell counts were significantly associated with 14-day acute kidney injury progression (adjusted odds ratio: 1.04, 95% confidence interval: 1.02–1.06, P < 0.01) and 14-day mortality (adjusted odds ratio: 1.06, 95% confidence interval: 1.04–1.09, P < 0.01). However, white blood cell counts were not associated with 14-day dialysis (adjusted odds ratio: 1.01, 95% confidence interval: 0.97–1.05, P = 0.77). Further curve fitting analysis found a linear correlation between white blood cell counts and 14-day acute kidney injury progression and 14-day mortality.
Conclusion
White blood cell counts had a significant linear correlation with 14-day acute kidney injury progression and 14-day mortality, but not with 14-day dialysis.
Introduction
White blood cell (WBC) count indicates the quantity of white blood cells present in the blood, usually measured as the number of WBCs per microliter.1,2 This measure is known for its simplicity, speed, practicality, repeatability, and cost-effectiveness. 3 WBC counts are included in standard blood tests and have significant clinical implications. WBC counts aid in diagnosing and monitoring infections and blood disorders, identifying inflammatory reactions, and assessing immunological function.4,5 WBC counts are also often used for evaluating the response to treatment and assessing prognosis.6–8 Acute kidney injury (AKI), defined as a rapid loss in kidney function, is a prevalent clinical condition with high mortality that affects millions of people worldwide.9,10 The severity of AKI varies; mild injuries can potentially self-resolve, whereas severe AKI may require dialysis treatment and dramatically increase the risk of patient mortality.11,12 Hence, apart from timely identification, it is crucial to prioritize monitoring the progression and prognosis of AKI. In recent years, there has been growing interest in the association between WBC counts and AKI. Studies such as a retrospective analysis of sepsis-induced AKI in emergency departments have explored using parameters related to WBC counts (e.g. delta neutrophil index and neutrophil‑to‑lymphocyte ratio (NLR)) to predict AKI risk.13,14 Although most studies have primarily focused on predicting the risk of AKI using multiple factors,15–17 a few have investigated the progression and prognosis of AKI, with more attention to critically ill patients. 18 Moreover, nearly all previous studies have used admission WBC counts, restricting the applicability of the findings to the prognosis of patients with AKI.15,17–19 Therefore, it is essential to determine the association between WBC counts at the onset of AKI and the progression and prognosis of AKI.
Objective
To investigate the association between WBC counts at the onset of AKI and the progression and prognosis of AKI.
Methods
Study design
A retrospective analysis was conducted using data from a multicenter randomized trial on an AKI early warning system.
Data source
The data source for this study was derived from a multicenter randomized controlled trial investigating the impact of electronic health record alerts on AKI outcomes (ClinicalTrials.gov NCT02753751). The trial involved 6030 adult inpatients across 6 hospitals, with results showing no significant reduction in mortality, dialysis, or kidney injury progression. 20 The raw data were publicly archived in Dryad (doi:10.5061/dryad.4f4qrfj95), an open-access repository of archived research data for free public access and citation (https://datadryad.org/stash/dataset/doi:10.5061/dryad.4f4qrfj95).
Setting
The research cohort consisted of adult inpatients from six hospitals in the Yale New Haven Health System.
Ethics approval and consent to participate
Data were anonymized by removing or generalizing all direct identifiers (e.g. names, IDs, dates, and locations) and indirect identifiers (e.g. rare diagnoses and unique combinations of traits) to prevent reidentification. The investigations involving human participants received approval from the Research Ethics Committee of the Yale School of Medicine institutional review board (ID 1604017596) and the Bridgeport Hospital institutional review board (IDs 051802, 041801, 071808) under a waiver of informed consent. Approval was also obtained from the Ethics Committee of the Second Affiliated Hospital of Xi’an Jiaotong University. The study was performed in accordance with the Helsinki Declaration of 1975, as revised in 2024, and the study involved retrospective data analysis.
Inclusion and exclusion criteria
The inclusion criteria were as follows: (a) age ≥18 years; (b) patients diagnosed with AKI based on the KDIGO (Kidney Disease: Improving Global Outcomes) AKI criteria.
The exclusion criteria were as follows: (a) dialysis in the past year; (b) end-stage renal disease; (c) baseline serum creatinine level ≥4.0 mg/L; (d) hospice care; (e) kidney transplantation within the past 6 months; (f) extreme value of WBC counts above the 97.5th percentile and below the 2.5th percentile (the range of WBC counts is particularly wide, ranging from 0.1 to 180 × 1000/μL); (g) WBC counts measured after a time period beyond 6 h after the identification of AKI.
Participants
From 29 March 2018 to 14 December 2019, this study enrolled 5471 individuals with AKI who satisfied the inclusion and exclusion criteria.
Measurement of WBC count
To ensure the reliability of the study results, WBC counts were measured within 6 h of AKI diagnosis. This criterion was implemented to capture values most relevant to the immediate post-diagnosis phase, minimizing potential confounding factors related to delayed measurement. As stated in the exclusion criteria, WBC counts obtained beyond this 6-h window were excluded from the analysis to maintain data consistency and focus on early-phase AKI dynamics.
Outcome indicators
The study included the following three outcomes: 14-day AKI progression, 14-day dialysis, and 14-day mortality. Fourteen-day AKI progression was defined as an increase in the stage of AKI for 14 days based on KDIGO criteria. Fourteen-day dialysis was defined as the requirement for renal replacement therapy initiation within 14 days following the AKI diagnosis according to KDIGO criteria. Fourteen-day mortality was defined as death from any cause occurring within 14 days of AKI diagnosis.
Statistical analysis
Continuous variables were presented as the median and range (minimum to maximum). Categorical variables were presented using counts and percentages. Univariate analysis, multivariate logistic regression, and smooth curve fitting (generalized additive modeling) were used to evaluate the association between WBC counts and the progression and prognosis of AKI. As the Elixhauser score includes related comorbidities and the Sequential Organ Failure Assessment (SOFA) score includes platelets and blood creatinine, to avoid collinearity, variables related to comorbidities, platelets, and blood creatinine were excluded after including the Elixhauser and SOFA scores in multivariate analysis. The statistical software EmpowerStats was used, and the two-sided significance level was set at P < 0.05.
Results
Clinical characteristics of the patients
A total of 6030 patients were initially included in the primary study. Extreme values of WBC counts above the 97.5th percentile and below the 2.5th percentile were excluded, removing 397 patients. A further exclusion criterion was applied to remove measurements of WBCs taken >6 h after the detection of AKI, thereby excluding an additional 162 patients. Finally, a total of 5471 patients were included in the study. The median age of the patients was 69.52 years, with a range of 18.14–89.99 years. The study included 2851 male and 2620 female patients. Of these patients, 15.9% were categorized as Black. Most patients were admitted to urban teaching hospitals (77.85%), with fewer admissions in suburban teaching (9.67%) and suburban nonteaching hospitals (12.48%). A significant proportion of patients showed medical admission (75.16%), and nearly one-third required intensive care unit (ICU) admission (31.82%). Several comorbidities were prevalent among the patients, including chronic kidney disease (38.66%), chronic obstructive pulmonary disease (34.67%), diabetes (41.93%), and hypertension (82.58%), and nearly half of the patients had a history of congestive heart failure (45.22%). The patients’ laboratory values showed a median anion gap of 12.00 mmol/L, bicarbonate level of 24.00 mmol/L, blood urea nitrogen (BUN) level of 28.00 mg/dL, hemoglobin level of 10.70 g/dL, estimated glomerular filtration rate (eGFR) of 55.34 mL/min/1.73 m2, potassium level of 4.20 mmol/L, sodium level of 138.00 mmol/L, and WBC count of 9.80 × 1000/μL. In terms of AKI, most patients had a disease duration of <2 days (72.42%), with fewer patients experiencing AKI for 2–7 days (23.47%) or >7 days (4.11%). At 14 days, AKI progression was observed in 15.21% of patients, 3.00% required dialysis, and the mortality rate was 8.41% (Figure 1 and Table 1)
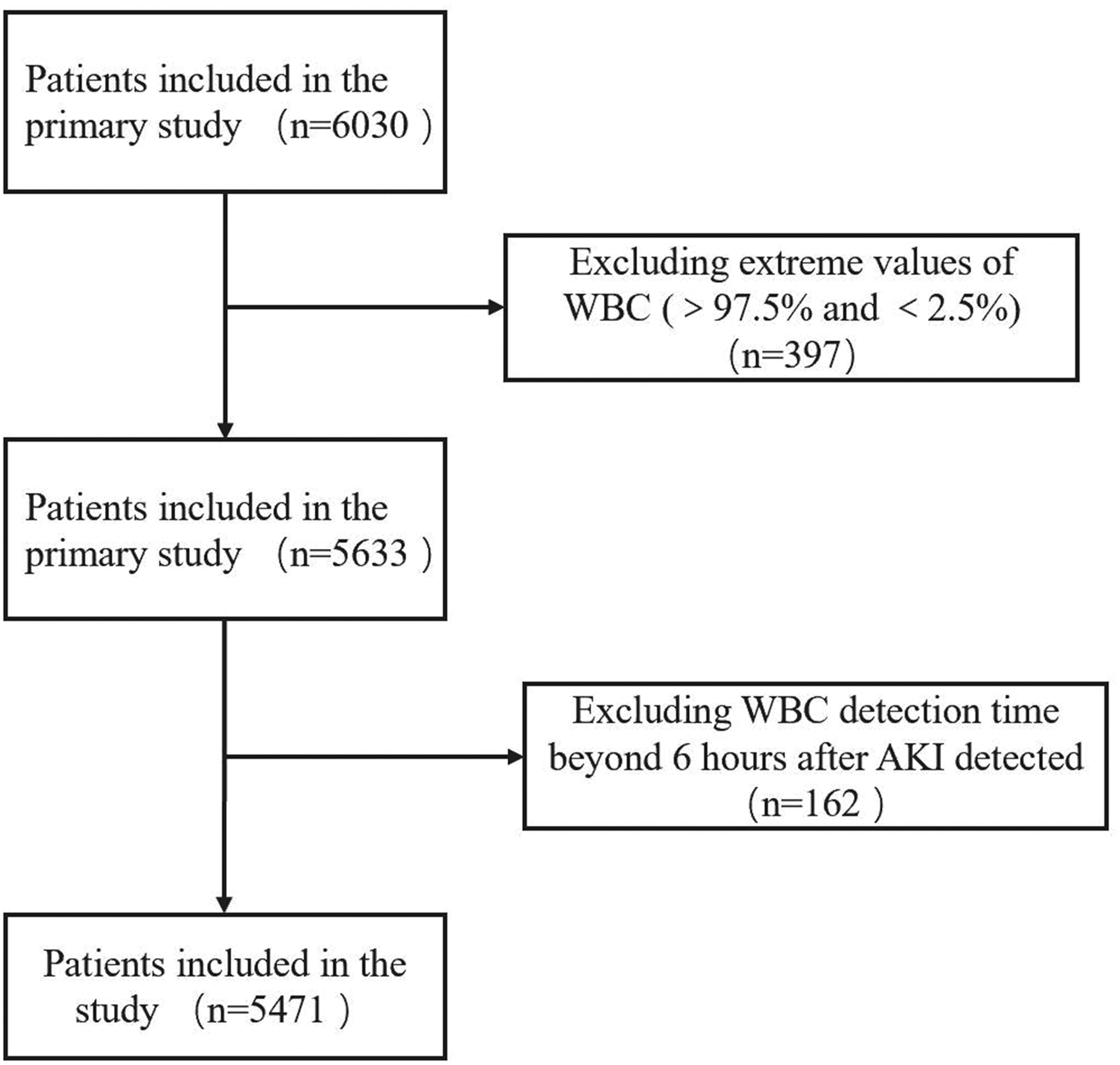
The diagram outlines the exclusion process for the study cohort. From an initial cohort of 6030 patients, exclusions for extreme WBC values (>97.5% or <2.5%; n = 397) and delayed WBC detection (>6 h post-AKI; n = 162) yielded a final cohort of 5471 patients. AKI: acute kidney injury; WBC: white blood cell.
Clinical characteristic of the patients.

Composite outcomes include AKI progression, dialysis, or mortality at 14 days.
AKI: acute kidney injury; BUN: blood urea nitrogen; CKD: chronic kidney disease; COPD: chronic obstructive pulmonary disease; eGFR: estimated glomerular filtration rate; ICU: intensive care unit; SOFA: Sequential Organ Failure Assessment; WBC: white blood cell.
Results of multivariate logistic regression analysis examining the association between various exposures and the progression and prognosis of AKI
An increase in WBC counts by 1 × 1000/μL was associated with a 4% increase in the odds of 14-day AKI progression (odds ratio (OR) = 1.04, 95% confidence interval (CI): 1.02–1.06, P < 0.01) and a 6% increase in the odds of 14-day mortality (OR = 1.06, 95% CI: 1.04–1.09, P < 0.01). However, there was no significant association with 14-day dialysis (OR = 1.01, 95% CI: 0.97–1.04, P = 0.78). Age did not significantly affect 14-day AKI progression and 14-day dialysis, but each additional year of age was associated with a 3% increase in the odds of 14-day mortality. Sex-stratified analyses demonstrated no statistically significant differences in clinical outcomes between male and female patients. Compared with other races, Black individuals showed no significant difference in the three outcomes. Alerts showed no significant difference in the three outcomes, compared with usual care. Admitted patients showed a significantly increased risk of 14-day mortality. The results also indicated that being admitted to a suburban teaching hospital or a suburban nonteaching hospital, compared with admission to an urban teaching hospital, significantly increased the odds of 14-day mortality. Being admitted to the ICU was associated with significantly higher odds of all three outcomes. The duration of AKI was strongly associated with all outcomes. An increase of 1 mmol/L in the anion gap was associated with a 6% increase in the odds of 14-day AKI progression and a 9% increase in the odds of 14-day mortality. However, the anion gap showed no significant association with 14-day dialysis. Conversely, a decrease of 1 mmol/L in bicarbonate level was associated with a 7% decrease in the odds of 14-day dialysis and a 3% decrease in the odds of 14-day mortality. However, bicarbonate level showed no significant association with 14-day AKI progression. Furthermore, hemoglobin and potassium levels were not associated with AKI progression and prognosis. For each increase of 1 mg/dL in BUN level, there was a significant decrease in the risk of 14-day AKI progression and a significant increase in the risk of 14-day mortality. For each increase of 1 mL/min/1.73 m2 in eGFR, there was a significant increase in the risk of AKI progression and mortality within 14 days. For each increase of 1 mmol/L in sodium level, there was a significant increase in the risk of 14-day mortality. For each increase of 1 point in the SOFA score, there was a significant increase in the risk of all outcomes. For each increase of 1 point in the Elixhauser score, there was a significant increase in the risk of 14-day AKI progression and 14-day dialysis, but it was not associated with 14-day mortality. Compared with patients without a nephrology consult, those who received a consult within 14 days of admission showed a significantly increased risk of the three outcomes, especially the risk of dialysis within 14 days. Compared with AKI duration <2 days, AKI duration ≥7 days significantly increased the risk of all outcomes (Table 2).
Results of multivariate logistic regression analysis examining the association between various exposures and the progression and prognosis of AKI.

AKI: acute kidney injury; BUN: blood urea nitrogen; eGFR: estimated glomerular filtration rate; ICU: intensive care unit; SOFA: Sequential Organ Failure Assessment; WBC: white blood cell; OR: odds ratio; CI: confidence interval.
Results of multivariate logistic regression analysis of the relationship between WBC counts and the progression and prognosis of AKI
In the multivariate logistic regression analysis, we found a significant association between WBC counts and 14-day AKI progression and 14-day mortality, but it was not associated with 14-day dialysis. For 14-day AKI progression, each unit increase in WBC count was associated with 7% (OR = 1.07, 95% CI: 1.05–1.08, P < 0.01), 5% (OR = 1.05, 95% CI: 1.04–1.07, P < 0.01), and 4% (OR = 1.04, 95% CI: 1.02–1.06, P < 0.01) increased risks in the crude model, model 1, and model 2, respectively. For 14-day dialysis, each unit increase in WBC count was associated with 6% (OR = 1.06, 95% CI: 1.03–1.09, P < 0.01), 4% (OR = 1.04, 95% CI: 1.01–1.07, P = 0.02), and 1% (OR = 1.01, 95% CI: 0.97–1.05, P = 0.77) increased risks in the crude model, model 1, and model 2, respectively. For 14-day mortality, each unit increase in WBC count was associated with 11% (OR = 1.11, 95% CI: 1.09–1.13, P < 0.01), 8% (OR = 1.08, 95% CI: 1.06–1.11, P < 0.01), and 6% (OR = 1.06, 95% CI: 1.04–1.09, P < 0.01) increased risks in the crude model, model 1, and model 2, respectively. The adjusted variables in model 1 included age, race, sex, medical admission status, Elixhauser score, hospital type, and ICU admission. The adjusted variables in model 2 included the variables in model 1 as well as alert, anion gap, bicarbonate, BUN, hemoglobin, eGFR, potassium, sodium, SOFA score, and contrast within the past 72 h (Table 3).
Multivariate logistic regression analysis of the relationship between WBC counts and the progression and prognosis of AKI.

Adjusted variables: Model 1 includes age, race, sex, medical admission status, Elixhauser score, hospital type, intensive care unit admission; Model 2 includes Model 1 variables as well as alert, anion gap, bicarbonate, blood urea nitrogen, hemoglobin, estimated glomerular filtration rate, potassium, sodium, Sequential Organ Failure Assessment score, and contrast within the past 72 h.
AKI: acute kidney injury; WBC: white blood cell; OR: odds ratio; CI: confidence interval.
Results of curve fitting
After adjusting for age, race, sex, medical admission status, Elixhauser score, hospital type, ICU admission, alert, anion gap, bicarbonate, BUN, hemoglobin, eGFR, potassium, sodium, SOFA score, and contrast within the past 72 h, a positive linear relationship was found between WBC counts and 14-day AKI progression and 14-day mortality. However, the correlation between WBC counts and 14-day dialysis was poor (Figure 2).

After adjusting for age, race, sex, medical admission status, Elixhauser score, hospital type, ICU admission, alert, anion gap, bicarbonate, BUN, hemoglobin, eGFR, potassium, sodium, SOFA score, and contrast within the past 72 h, a linear positive relationship was found between WBC counts and 14-day AKI progression and 14-day mortality (a, c, and d). However, the correlation between WBC counts and 14-day dialysis was poor (b). AKI: acute kidney injury; BUN: blood urea nitrogen; eGFR: estimated glomerular filtration rate; ICU: intensive care unit; SOFA: Sequential Organ Failure Assessment; WBC: white blood cell.
Results of subgroup analysis of the relationship between WBC counts and the progression and prognosis of AKI
A comprehensive subgroup analysis was conducted to ascertain the relationship between WBC counts and the progression and prognosis of AKI (14-day AKI progression, 14-day dialysis, and 14-day mortality). The subgroup analysis revealed that, with the exception of certain conditions (suburban teaching hospitals, suburban nonteaching hospitals, alert patients, AKI duration ≥7 days, Elixhauser score ≥10 and without malignancy, and WBC count ≥4 × 1000/μL but <20 × 1000/μL), an elevated WBC count was associated with an increased risk of 14-day AKI progression and 14-day mortality. Regarding 14-day dialysis, a higher WBC count was associated with an increased risk only in women, while no significant correlation was found in other circumstances. The analysis adjusted for confounding factors, excluding the variables under subgroup analysis, which included age, race, sex, medical admission status, Elixhauser comorbidity score, hospital type, ICU admission, alert, anion gap, bicarbonate levels, BUN, hemoglobin, eGFR, potassium, sodium, SOFA score, and contrast within the past 72 h (Table 4).
Subgroup analysis of the relationship between WBC counts and the progression and prognosis of AKI.

Adjusted variables (without the subgroup analysis variables): age, race, sex, medical admission status, Elixhauser score, hospital type, ICU admission, alert, anion gap, bicarbonate, blood urea nitrogen, hemoglobin, estimated glomerular filtration rate, potassium, sodium, Sequential Organ Failure Assessment score, and contrast within the past 72 h.
AKI: acute kidney injury; WBC: white blood cell; OR: odds ratio; CI: confidence interval; inf: infinity.
Discussion
In this study, both multivariate logistic regression analysis and subgroup analysis revealed a significant association between WBC count at the onset of AKI and 14-day AKI progression and 14-day mortality. However, there was no significant association identified between WBC count at the onset of AKI and 14-day dialysis. Additional curve fitting analysis revealed a linear correlation between WBC count at the onset of AKI and 14-day AKI progression and 14-day mortality.
Previous studies have established a correlation between WBC count, a conventional indicator of inflammation, and detrimental consequences across a range of diseases. 19 However, its role in the progression of AKI remains unknown, and the majority of recent studies have concentrated on investigating the correlation between WBC count and the risk of AKI.18,21 Investigations in animal and cell models constitute the majority of research on WBC counts and AKI progression, 22 which have shown that neutrophils, macrophages, natural killer cells, and lymphocytes play an essential role in the pathophysiological process of AKI. 22 For example, the aggregation and activation of inflammatory cells may worsen kidney damage through the facilitation of endothelial dysfunction, elevation of vascular permeability, and direct impairment of renal tubular epithelial cells.23–25 In addition, WBCs, particularly neutrophils, might exacerbate tissue injury and local inflammatory responses via the release of reactive oxygen species and proteases.26,27 Therefore, an increase in WBC count indicates a more active inflammatory state, which may contribute to the onset and progression of AKI. 28
This study discovered a significant correlation between WBC counts and the prognosis of AKI. Although research on the correlation between WBC counts and AKI prognosis is limited, the findings are consistent with those from previous research revealing a strong correlation between elevated WBC counts and a poor prognosis in patients with AKI. Some studies involving ICU patients with AKI have revealed that the mortality rate increases with rising baseline WBC counts.14,18,21,29,30 The association between WBC counts and mortality has been extensively studied across various diseases.31–33 Consequently, this study further broadens the value of WBC counts in an even more extensive cohort of patients with AKI.
A correlation of WBC counts was observed with the progression and mortality rate of AKI, but not with 14-day dialysis. The possible causes included the following. 1. Dialysis initiation timing: The initiation of dialysis was conventionally determined by a range of clinical indicators, encompassing fluid excess, electrolyte imbalance (e.g. hyperkalemia), diminished urine output, and blood toxin concentrations (e.g. creatinine and urea nitrogen). 34 Although WBC counts indicate an inflammatory state, they do not provide direct information regarding renal function or the indications for dialysis. 2. The relationship between inflammation and kidney injury: Although inflammation can potentially contribute to the development or worsening of AKI, it does not consistently result in the necessity for dialysis treatment. The need for dialysis is primarily determined by the kidney’s filtration function, which is not always directly correlated with the inflammatory state.35,36 3. Temporal fluctuations in inflammation: The time span of 14 days was comparatively brief, and the fluctuations in WBC counts can potentially be associated with a transient inflammatory reaction. Furthermore, this transient response might not be substantial enough to warrant dialysis during this period. 4. Influence of additional complications: Patients with AKI might experience a range of complications, some of which might influence the decision to undergo dialysis. 37 For example, in the case of a patient presenting with severe heart failure, fluid restriction and dialysis were considered necessary despite the absence of conventional dialysis thresholds. 38
The pathophysiological process of AKI might be effectively characterized by AKI progression, dialysis, and mortality. However, relying on a single indicator has the following limitations. 1. A single indicator might not fully reflect the severity of the disease: The severity of AKI might not only be reflected by the decline in renal function but might also include the patient’s overall condition, occurrence of complications, and degree of response to treatment. 10 2. Diversity of disease progression: The pathophysiological process of AKI is complex and variable, and the disease progression path of individual patients might differ. 39 Some patients might progress rapidly to the need for dialysis, while others might die without reaching the dialysis standard. A single indicator cannot capture the diversity of disease progression. 3. Impact of treatment decisions: The decision to undergo dialysis often depends on a variety of factors, including patient preferences, availability of medical resources, and different treatment plans. 34 Therefore, dialysis itself might not fully reflect the natural course of the disease. 4. Multifactorial impacts on mortality: The mortality of patients with AKI may be impacted by numerous variables, such as renal function loss, organ function failure, infection, and cardiovascular events. 40 5. Interplay of indicators: There might be interactions between AKI progression, dialysis, and mortality. For example, although timely dialysis might improve prognosis and decrease mortality, it might also increase the risk of complications, influencing the outcome. Therefore, to effectively estimate the progression and prognosis of AKI, it was crucial to consider the composite of indicators rather than a single indicator.
WBC count, NLR, and prognostic nutritional index (PNI) are biomarkers for assessing AKI, each with distinct advantages and limitations. WBC count is a simple, rapid, cost-effective test and is widely used in clinical practice. It shows a significant linear correlation with AKI progression and prognosis, making it valuable for early risk identification. NLR offers high sensitivity by reflecting the balance between inflammation and immune regulation, particularly in critically ill patients; however, its complexity and susceptibility to confounding factors restrict its application.41,42 PNI provides a comprehensive evaluation of nutritional and immune status, with greater accuracy in nonchronic kidney disease patients, although its reliance on stable albumin levels and variability across studies pose challenges. 43 Overall, WBC counts excel in accessibility and affordability, particularly in resource-limited settings, while NLR and PNI provide detailed assessments for optimizing AKI management. Future research should focus on dynamic changes and combined application of these biomarkers to improve diagnostic and prognostic accuracy.
Strength of the study
This study had certain strengths. First, this study employed WBC counts at AKI onset, which clearly defined the detection time of WBC counts, compensating for the fact that prior studies frequently measured outcomes at admission or did not define the timing of assessments. Second, the use of composite endpoint indicators might more comprehensively reflect the impact of AKI on patients. Third, WBC count was found to be linearly correlated with the progression and prognosis of AKI, increasing its value for AKI management. Fourth, this study expanded the value of WBC counts in AKI in a wider population outside of ICU patients, providing a new inflammation-related biomarker for AKI progression and prognosis. The research population was large and representative, with high clinical applicability of the results.
Limitations of the study
This study had several limitations. First, this study only focused on the WBC counts at the onset of AKI, which might not indicate changes in the inflammatory state throughout the course of AKI. Second, although the study adjusted for multiple confounding factors, there might still be variables that were not identified or could not be measured that would have affected the results. Third, the decision to initiate dialysis might be influenced by multiple factors, such as hospital resources, physician preferences, and patient conditions, which were not fully accounted for in this study. Fourth, the 14-day follow-up period limited our analysis due to data constraints. Future studies should explore longer follow-up periods (e.g. 28 days) to further validate our findings. Fifth, WBC counts can be impacted by several variables (e.g. hormone exposure, chemotherapy history, infections, malignancies, and hematologic malignancies); however, due to insufficient data, this study did not adjust for these variables, which should be addressed in future research. Sixth, a critical limitation was our inability to analyze leukocyte subtype (e.g. neutrophils and lymphocytes), precluding mechanistic insights into their distinct roles in AKI progression. Seventh, the variability and fluctuation of WBC counts are influenced by factors such as steroid therapy and sepsis; therefore, cautious and appropriate application of our findings is necessary in clinical practice.
Conclusion
In this study, we systematically evaluated the relationship between WBC counts at the onset of AKI and the progression and prognosis of AKI. Our analysis showed that, after adjusting for related potential confounding factors, WBC counts at the onset of AKI had a significant linear correlation with 14-day AKI progression and 14-day mortality, but not with 14-day dialysis. These findings highlight the possible value of WBC counts at the onset of AKI in assessing the short-term progression and prognosis of AKI.
Supplemental Material
sj-pdf-1-imr-10.1177_03000605251369843 - Supplemental material for Linear correlation between white blood cell counts and the progression and prognosis of acute kidney injury
Supplemental material, sj-pdf-1-imr-10.1177_03000605251369843 for Linear correlation between white blood cell counts and the progression and prognosis of acute kidney injury by Honghua Liu, Qiao Gu, Yuhe Zhao, Hai Wang and Feng Liu in Journal of International Medical Research
Footnotes
Acknowledgments
We would like to express our gratitude to Wilson Francis for making the data available in the Dryad repository.
Authors’ contributions
Honghua Liu and Qiao Gu participated in the research design and the writing of the manuscript; Yuhe Zhao conducted data analysis; Hai Wang and Feng Liu provided substantial advice on designing the study and assisted in writing and revising the paper. All authors reviewed the manuscript.
Consent to participate declaration
Not applicable.
Clinical trial number
Not applicable.
Declaration of conflicting interests
The authors have no conflicts of interest to disclose.
Funding
No funding.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.