
Abstract
Objective
This study was performed to introduce posterior laminectomy and pedicle screw fixation for the treatment of upper cervical spinal cord tumors and investigate the curative effects.
Methods
Eighteen patients (11 men, 7 women) who underwent surgical treatment of an upper cervical intraspinal tumor from January 2008 to June 2013 were reviewed. Clinical parameters including age, sex, affected spinal levels, lesion location, duration and type of symptoms, and pathological features were retrospectively investigated.
Results
The mean operation time was 181.9 ± 25.5 minutes (range, 135–240 minutes), and the mean blood loss volume was 1038.9 ± 284.2 mL (range, 750–1530 mL). The Frankel grade, Japanese Orthopaedic Association score, and Karnofsky performance status score were significantly better postoperatively than preoperatively. The radiographic examination revealed good bone graft fusion. Two patients developed tumor recurrence, while four patients developed intraoperative or postoperative complications.
Conclusions
Management of upper cervical intraspinal tumors by posterior laminectomy and pedicle screw fixation can relieve compression of the cervical cord and nerve root, thoroughly remove the tumor lesion, reconstruct the stability of the upper cervical spine, and improve patients’ quality of life.
Keywords
Introduction
Upper cervical intraspinal tumors are rare tumors located from level C1 to C3. They are considered difficult to treat by spinal surgery and neurosurgery because of the specific anatomical characteristics of the upper cervical spine. 1 Continuous compression of the upper cervical cord or the medulla oblongata by tumors can cause respiratory and circulatory disorders, high paraplegia, and even death. 2 However, the early symptoms of upper cervical intraspinal tumors are nonspecific; the most frequently reported initial symptoms are occipital and posterior neck pain, neck tilting, and limited range of motion. 3 Neurological signs may be absent if the early symptoms do not include pyramidal signs of spinal cord compression; thus, upper cervical spine tumors are often misdiagnosed or diagnosed late.
Surgical relief of spinal cord, nerve root, and vertebral artery compression along with reconstruction and stabilization of the cervical spine by fixation is currently the most effective and important therapy for upper cervical intraspinal tumors.4–7 However, the best operative approach for such tumors, especially those located in the ventral part of the cervical cord, is controversial. Critical respiratory and circulatory functions may be affected intraoperatively depending on the location of the tumor, and such functional disruptions can be life-threatening. According to our own experience and the findings of other studies, intraspinal tumors of the upper cervical spine can be successfully removed using a posterior approach without interfering with the spinal cord. However, this requires a good command of the surgical anatomy, accurate identification of the relationship between the tumor and spinal cord, and a careful operative technique.
In this study, we evaluated the effects of posterior laminectomy and fixation with pedicle screws to treat upper cervical intraspinal tumors. Preoperative, postoperative, and mid-term follow-up results were analyzed and evaluated by the Frankel grade, Japanese Orthopaedic Association (JOA) score, and Karnofsky performance status (KPS) score.
Materials and methods
Clinical data
This clinical and retrospective study was approved by the Institutional Review Board of Xiamen University. Written informed consent was obtained from all patients preoperatively. Eighteen patients (11 men and 7 women) who underwent surgery for an upper cervical intraspinal tumor from January 2008 to June 2013 were enrolled in the study. The patients’ average age was 47.7 years (range, 37–65 years). Pathological reports confirmed 11 neurinomas, 3 meningiomas, 2 lipomas, 1 ependymoma, and 1 case of neurofibromatosis. The Peking University Third Hospital (PUTH) classification of the 18 tumors was type A in 11 cases, type II in 5 cases, and type III in 2 cases. Three of the 18 tumors occurred at C1, 9 occurred at C1/2, 1 occurred at C2, 3 occurred at C2/3, and 2 occurred at C1 to 3. The locations of the tumors included 4 epidural tumors, 13 intradural extramedullary tumors, and 1 intramedullary tumor. Four tumors were located in the ventral cervical cord (Table 1).
Patients’ general characteristics.
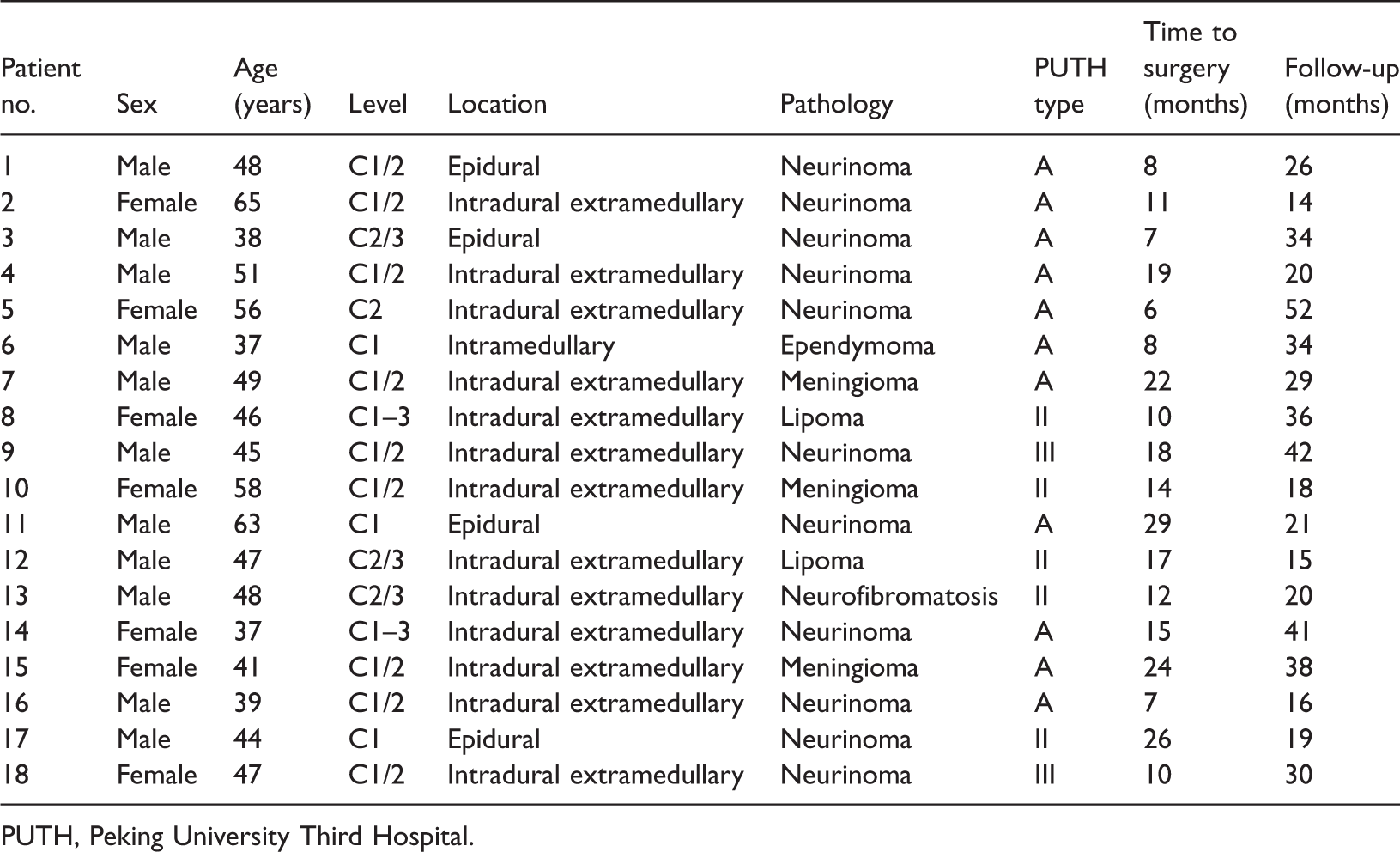
PUTH, Peking University Third Hospital.
The average duration from symptom onset to surgery was 14.6 months (range, 6–29 months). Of the 18 patients, 9 experienced occipital and posterior neck pain as the initial symptom. In addition, 7 of the 18 patients had symptoms of nerve root compression such as unilateral or bilateral upper extremity numbness, pain, or clumsiness; 6 had biceps jerk and triceps reflex activities; 7 had a positive trepidation sign and ankle clonus; 11 had positive Hoffmann signs and Babinski signs; and 2 had loss of sphincter control at diagnosis. The mean preoperative JOA score was 9.7 ± 2.9 (range, 6–17), and the mean preoperative KPS score was 71.7 ± 11.5 (range, 50–90). Three patients had Frankel grade C spinal cord injury, 13 had grade D, and 2 had grade E (Table 2).
Clinical assessment results.

JOA, Japanese Orthopaedic Association; KPS, Karnofsky performance status; Pre, preoperative; Post, postoperative; CSF, cerebrospinal leakage; SD, standard deviation.
Imaging examination
Preoperative imaging is important to determine the tumor boundaries, course of the vertebral arteries, and relationship between the tumor and spinal nerves. Thus, all 18 patients underwent cervical X-ray examinations (anteroposterior and lateral views), computed tomography scans, and magnetic resonance imaging (MRI). Six patients were found to have a deformation of the pedicle of the vertebral arch and widened interpedicular distances, three patients had intervertebral foraminal dilatation, and two patients had a comma-shaped impression in the posterior centrum and vertebral bone absorption (Figure 1). Four patients had tumors that were dumbbell-shaped, showed isointensity in T1-weighted imaging (T1WI), and showed high intensity in T2-weighted imaging (T2WI). Fourteen patients had round or oval intradural tumors with distinct boundaries (11 neurinomas, 1 meningioma, and 2 lipomas). Some of the lesions that were accompanied by bleeding had uniform or uneven low-intensity signals in T2WI with upper cervical spine compression and displacement. Enhanced MRI showed signal enhancement and clear circumscription in two patients (Patients 6 and 15). In one patient (Patient 13, who had neurofibromatosis), the lesion showed isointensity in T1WI, uneven high intensity in T2WI, and indistinct boundaries.

Computed tomography showing a comma-shaped impression in the centrum and vertebral bone absorption at the left margin of C2, which is indicated by arrows (→) (Patient 2).
Operation
All patients underwent general anesthesia with endotracheal insufflation. The patients were placed in the prone position with a “U”-shaped pillow under the chest and abdomen and the head in a spindle stock. A posterior approach was used, and a longitudinal medial skin incision was made. The posterior aspect of the occiput, acanthae of the atlantoaxial vertebrae, and vertebral laminae and facets were revealed. To maintain cervical stability of the atlantoaxial vertebrae after tumor resection, pedicle screws were inserted and fixed to a rod on the side away from the tumor prior to resection. Laminectomy was performed to expose the upper and lower poles of the tumor. In the four patients with epidural tumors, the tumors were removed within its false membrane as completely as possible. In the 14 patients with intradural or intramedullary neoplasms, the dura was incised and tagged with silk. The arachnoid outside the spinal cord was dissected to expose the spinal cord and nerve roots. One nerve dissector was used to hold the tumor while another was used to cautiously resect the tumor from the spinal cord. Tumors located in the ventral cervical cord were first fixed to silk and then dissected. Close attention was paid to stabilization during disassociation of the tumor from the spinal cord to avoid over-stretching the spinal cord. The second rod was then inserted and the screws tightened. Intraoperative radiographs were taken to ensure that the screws and bone were appropriately fixed. Finally, autogenous iliac bone was grafted, the wound was rinsed, and the incision was closed.
Postoperative treatment
Tracheotomy instruments and a breathing machine were routinely prepared and made available at the bedside postoperatively. Blood gas analysis and electrolyte measurements were performed to prevent internal metabolic disorders. All patients received intravenous antibiotics for 24 hours postoperatively. Patients without cerebrospinal fluid (CSF) leakage were placed on strict bed rest for at least 1 week and were then allowed to walk with a neck collar. Use of a neck collar was continued for an average of 3 months postoperatively. Radiological examination was used to identify the fixation position and bone fusion status.
Statistical analysis
All data are presented as mean ± standard deviation. The paired t-test was performed to compare the scores before and after surgery using SPSS Statistics for Windows, Version 17.0 (SPSS Inc., Chicago, IL, USA). A P value of <0.05 was considered statistically significant.
Results
Seventeen of the 18 patients’ tumors were completely excised. One tumor (Patient 8) that was located in the ventral cervical cord and intervertebral foramina was partially resected. All cases of neck pain or dizziness following surgery resolved 3 to 4 weeks after surgery. However, a longer period was required for resolution of limb anesthesia. The mean duration of surgery was 181.9 ± 25.5 minutes (range, 135–240 minutes). The mean blood loss volume was 1038.9 ± 284.2 mL (range, 750–1530 mL).
Table 2 summarizes the patients’ preoperative and postoperative clinical findings. The Frankel grade had improved by 0 to 2 grades by the 3-month follow-up. Among the three patients with preoperative Frankel grade C, one had recovered to Frankel grade D and two had recovered to Frankel grade E by the 3-month follow-up. Eleven patients with preoperative Frankel grade D had recovered to Frankel grade E by their 3-month follow-up visit, while two patients with preoperative Frankel grade D had no change in their Frankel grade at the 3-month follow-up. Furthermore, a significant improvement in the JOA scores in patients with neurological defects was observed at the 3-month follow-up (14.2 ± 2.3) compared with their preoperative scores (9.7 ± 2.9). A significant improvement in the KPS score at the 3-month follow-up (85.0 ± 7.9) compared with the preoperative score (71.7 ± 11.5) was also observed. Bone fusion was evident at a mean of 4.3 ± 2.2 months (range, 3–7 months) after treatment.
No patients developed neurological deterioration or vertebral artery injury. Two patients developed tumor recurrence (Patients 3 and 11) and required additional surgical treatment. Four patients developed minor complications: CSF leakage in two, superficial infection in one, and malpositioning of the pedicle screws in one. The patients with CSF leakage and superficial infection healed well with conservative treatment. In the patient with pedicle screw malpositioning, the two screws penetrated approximately 3 mm beyond the front edge of the vertebral body. Representative cases are shown in Figure 2 (Patient 10) and Figure 3 (Patient 14).

Preoperative, postoperative, and 3-month follow-up radiographs of the patient who underwent treatment of a meningioma by posterior laminectomy and C1–3 pedicle screw fixation (Patient 10). (a–c) Magnetic resonance imaging before the posterior laminectomy and C1–3 pedicle screw fixation. (d–g) Radiographic examination and magnetic resonance imaging 3 days after the operation. (h, i) Radiographic examination at the 3-month follow-up. (j) Postoperative pathological examination.

Preoperative, postoperative, 1-year follow-up, and 3-year follow-up radiographs of the patient who underwent treatment of a meningioma by posterior laminectomy and C1–4 pedicle screw fixation (Patient 14). (a–d) Magnetic resonance imaging before the posterior laminectomy and C1–4 pedicle screw fixation. (e–h) Radiographic examination and magnetic resonance imaging 7 days after the operation. (i, j) Magnetic resonance imaging at the 1-year follow-up. (k, l) Radiographic examination at the 3-year follow-up. (m) Postoperative pathological examination.
Discussion
Diagnosis
Upper cervical intraspinal tumors are rare, and few cases exist in the clinical literature. Upper cervical spinal tumors account for 18.0% to 39.5% of all cervical intraspinal tumors and only 5.0% to 14.4% of all intraspinal tumors.8,9 Early diagnosis of upper cervical intraspinal tumors is generally difficult because of the mild and nonspecific symptoms that patients experience in the early phase of disease. Nonspecific posterior neck pain and slight neck tilt are the most frequent initial symptoms. 3 In our study, 50% (9/18) of patients had occipital and/or posterior neck pain as their initial symptom, and 39% (7/18) had symptoms of nerve root compression. Thus, patients should be diagnosed not only based on clinical symptoms but also using various imaging modalities. Characteristic X-ray features of cervical intraspinal tumors are dilatation of the intervertebral foramina and broadening of the vertebral arch; however, these characteristics rarely occur because of the wide ventral intradural space. Computed tomography and MRI offer higher diagnostic accuracy because they can sufficiently delineate a cervical intraspinal tumor and better display the integrity of the spinal canal, the degree of spinal cord compression, and the invasion of the tumor into the paraspinal soft tissue.8,10 In particular, MRI can clearly exhibit the relationship between the tumor and surrounding structures, including whether the vertebral artery is compressed or displaced. 11 Furthermore, pinpointing the exact location of the tumor through MRI is crucial prior to surgery. Most intramedullary tumors are malignant and confer a poor prognosis. However, epidural and intradural extramedullary tumors often have good clinical outcomes when treated surgically because most are benign and easier to completely resect.
Approach
The purpose of surgical management of upper cervical intraspinal tumors is to resect the tumor, relieve spinal cord compression, and restore spinal stability.3,12 Various surgical approaches have been described for the treatment of upper cervical intraspinal tumors, including an extreme lateral approach,13,14 an anterior approach,15,16 and a posterior approach.17,18 However, the ideal surgical approach for upper cervical intraspinal tumors located in the ventral cervical cord is still controversial because of the complicated anatomic structure. Some scholars favor the anterior approach, which involves first performing a cervical corpectomy and then resecting the tumor. However, the anterior approach provides a smaller surgical field and leads to higher probability of anterior vertebral plexus bleeding and postoperative infection because of the need to traverse through the oral cavity. 19 The extreme lateral approach offers the advantage of direct visualization of the cervicomedullary junction and cord–tumor interface from a lateral aspect, and it prevents vertebral injury. 13 However, its clinical application is limited by the wide range of bone and soft tissue removal, complex anatomical structures, and higher risk of intraoperative trauma. Despite the controversies in clinical decision-making, it is generally accepted that a posterior approach is superior to both the anterior and extreme lateral approaches. The posterior approach has achieved considerable success in the management of posteriorly situated tumors. Furthermore, the posterior approach provides adequate access to ventral tumors through unilateral removal of part of the small joint, resection of the dentate ligament, and cutting of the C1/2 nerve roots.4,18,19 Acosta et al. 17 used the posterior paramedian transpedicle approach to dissociate the vertebral artery and nerve root, a method that could also safely remove tumors in the ventral aspect of the cervical cord. In the present study, selection of the surgical approach was strictly based on the PUTH classification. 20 Four ventral tumors were successfully managed with the posterior approach. A review of the literature, combined with our experience, shows that tumors in the upper cervical spinal canal can be resected through a posterior approach without interfering with the spinal cord. With full mastery of the anatomical structure and relationship between the tumor and spinal cord, most of these tumors can be completely resected.18,21
Reconstruction
Upper cervical instability after en bloc resection is a main cause of cervical swan-neck deformity and delayed injury of the cervical spinal cord.22,23 Thus, restabilization of the upper cervical spine is an important part of treating upper cervical intraspinal tumors. A polyaxial screw–rod system must be used to avoid atlantoaxial subluxation or dislocation after removing tumors from the C1 posterior arch and occipital bone. 3 Posterior pedicle screw fixation is a method of reconstruction that has been widely used in recent years because it offers immediate and superior stabilization and fusion.24,25 Furthermore, biomechanical studies have demonstrated superior rotational stability at facets when using posterior pedicle screw fixation than when using wiring because of its three-column fixation approach. 25 In the present study, reconstruction with the screw–titanium rod fixation technique was needed for total facetectomy to achieve ideal visualization in all patients. No patient developed spinal cord injury or vertebral artery injury.
Conclusion
We have herein present our results of treating upper cervical intraspinal tumors by posterior laminectomy and a fixation screw–rod system. Our findings indicate that satisfactory results can be obtained through a posterior approach. However, future studies with longer outcome measures and higher numbers of patients are still needed.
Footnotes
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This study was supported by the Medical Science and Technology Innovation Foundation of Nanjing Military Region (No. 12Z24), the Natural Science Foundation of Fujian Province (No. 2017J01163), and the Double Creation Star Foundation of Zhangzhou (No. ZZ201917).