
Abstract
Objective
This study was performed to assess the efficacy of a novel tool to assist transpedicular bone grafting in short-segment pedicle screw fixation combined with pedicle fixation at the level of the fractured vertebra (six-screw fixation).
Methods
We retrospectively analyzed 80 patients (40 in the control group and 40 in the tool-aided group) with single-level thoracolumbar fractures. Patients in the control group underwent traditional six-screw fixation combined with transpedicular bone grafting. In the tool-aided group, we introduced a novel vertebroplasty tool to assist transpedicular bone grafting. Basic information and related indicators were recorded.
Results
There were no significant differences in the patients’ baseline characteristics or surgical outcomes between the control group and tool-aided group. Both traditional surgery and tool-aided surgery restored the height of the fractured vertebrae and decreased the Cobb angle, visual analog scale score, and Oswestry Disability Index. However, tool-aided surgery more effectively restored the height of the fractured vertebrae and reduced the visual analog scale score and Oswestry Disability Index than did traditional surgery.
Conclusion
Vertebroplasty tool-aided surgery facilitated more precise and successful grafting of bone into damaged vertebrae than did traditional surgery and therefore might be recommended for treating single-level thoracolumbar fractures.
Keywords
Introduction
Spinal fractures are uncommon, accounting for only 0.7% of all fractures. About 90% of all spinal fractures occur in the thoracolumbar region, especially at the site of transition from the thoracic to lumbar spine (T11–L2); such fractures account for more than half of all thoracolumbar fractures.1,2 Despite the low incidence of thoracolumbar fractures, primary treatment is vitally important because these fractures can have serious consequences such as low back pain, spinal stenosis, spinal cord injury, and delayed neurologic compromise.
Posterior pedicle screw fixation is often used to treat thoracolumbar fractures, especially compression fractures and some burst fractures. Pedicle screws are placed in the pedicles of the vertebrae adjacent to the damaged vertebrae and are then connected by rods to hold the bones in place and stabilize the fracture while it heals. 3 Pedicle screw fixation can be divided into short-segment pedicle screw instrumentation (SSPI), long-segment pedicle screw instrumentation, and monosegmental pedicle screw instrumentation. 3 Posterior SSPI is the most widely used technique for spinal fractures; it involves bilateral insertion of pedicle screws into one level above and one level below the fractured vertebra with longitudinal rods connecting the tail ends of the pedicle screws, summarily involving four screws and two rods (four-screw fixation).4,5 Nevertheless, many studies have shown that SSPI cannot adequately achieve and maintain fracture reduction.5,6 For this reason, SSPI with pedicle fixation at the level of the fractured vertebra (six screws and two rods; six-screw fixation) was introduced to stabilize fractures and prevent loosening or breakage of screws.3,5 –9 Moreover, SSPI with transpedicular bone grafting was also introduced to promote vertebral fracture healing and maintain vertebral height. 10 However, how to precisely and successfully graft bone into damaged vertebrae has not been well established.
While providing additional fixation points in the fractured vertebra, six-screw fixation also provides a transpedicular channel for bone grafting. Traditional surgery involves the grafting of bone or bone substitute into the fractured vertebral body through this channel without the help of any tools. However, the grafting of bone or bone substitute into a fractured vertebral body is often inefficient and unsuccessful. In the current study, we introduced a novel tool to assist transpedicular bone grafting in posterior six-screw fixation for treating single-level thoracolumbar fractures.
Patients and methods
Patients
This retrospective study involved 80 patients with single-level thoracolumbar fractures who underwent posterior 6-screw fixation combined with transpedicular bone grafting in Jiangjin Central Hospital of Chongqing, China from January 2014 to January 2019. This study was conducted with approval from the Ethics Committee of Jiangjin Central Hospital and in accordance with the Declaration of Helsinki. All patients provided written informed consent to undergo treatment and for the use and publication of their data for research purposes. The reporting of this study conforms to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines. 11
The inclusion criteria were a single-level thoracolumbar fracture (T11–L2), vertebral height loss of >50%, age of 18 to 70 years, computed tomography (CT) finding of type A fracture according to the AO Spine classification, magnetic resonance imaging (MRI) finding of a fracture without definite discontinuation of the posterior ligament complex (PLC), a Thoracolumbar Injury Classification and Severity Score of ≥4, 12 duration of <1 week from injury to operation, and follow-up of >2 years after posterior six-screw fixation.
The exclusion criteria were multisegmental vertebral fractures; open vertebral fractures; CT finding of type B and C fractures according to the AO Spine classification; multiple other injuries, such as head, chest, or abdominal injuries; no need for surgical treatment; and ongoing cancer, infection, cardiac disease, coagulation disorders, serious osteoporosis, or other severe disease.
Vertebroplasty tool
In the present study, several components of a vertebroplasty tool (Qingdao Joyearn Medical Technology Co., Qingdao, China), which is shown in Figure 1(a), were used to guide the allograft bone (Shanghai Yapeng Biological Technology Co., Shanghai, China) into the fractured vertebra. These components were a push rod (Figure 1(b)), hollow vertebral drill (Figure 1(c)), work string (Figure 1(d)), and puncture needle (Figure 1(e)). A combination of the work string and puncture needle (Figure 1(f)) was used to embed the work string into the pedicle. Moreover, a combination of the push rod and hollow vertebral drill (Figure 1(g)) was used to push the allograft bone into the fractured vertebra through the work string (Figure 1(h)).

Bone grafting tool. (a) Vertebroplasty tool. (b) Push rod. (c) Hollow vertebral drill. (d) Work string. (e) Puncture needle. (f) Combination of work string and puncture needle. (g) Combination of push rod and hollow vertebral drill. (h) Combination of push rod, hollow vertebral drill, and work string.
Surgical procedure
All surgical procedures were performed under general anesthesia. All patients underwent posterior six-screw fixation combined with transpedicular bone grafting. In addition, patients in the tool-aided group underwent transpedicular allograft bone grafting with the aid of the above-described tool. The surgical procedure of posterior six-screw fixation with vertebroplasty tool-assisted transpedicular bone grafting was performed as follows.
The patient was placed in the hyperextended prone position to adequately expose the thoracolumbar and lumbar levels of the spine. Gel pads were used to support the chest, abdomen, and pelvis. Two Kirschner pins were placed on the patient’s back (Figure 2(a)). A C-arm X-ray machine was then used to determine the relationship between the Kirschner pins and fractured vertebra (Figure 2(b)). According to this relationship, the operative incision site was accurately identified and the incision was performed (Figure 2(c)).
Surgical procedure of posterior six-screw fixation combined with transpedicular bone grafting. (a) Two Kirschner pins. (b) X-ray image to determine the relationship between the Kirschner pins and fractured vertebra. (c) Operative incision. (d) X-ray image to determine whether the locating pins had been appropriately inserted. (e) X-ray image to determine whether the height of the compressed vertebra had been restored. (f) X-ray image to determine whether the work string had entered the hole in the pedicle of the fractured vertebra. (g)–(j) Allograft bone was put into the work string and pushed into the fractured vertebra using a push rod and hollow vertebral drill. (k) X-ray image was acquired after the connecting rods and screws were re-locked. (l) The caps of the screws were removed. After six vertebral pedicles were exposed, the surgeon drilled six 4-cm-deep holes through the pedicles and inserted locating pins into those holes. After the locating pins were determined to be adequately placed in the pedicles by C-arm X-ray examination (Figure 2(d)), the six locating pins were replaced by six pedicle screws. The connecting rods and screws were locked, and the C-arm X-ray machine was used to identify whether the height of the compressed vertebra had been restored (Figure 2(e)). The surgeon then removed the unilateral connecting rod and withdrew the screw from the pedicle of fractured vertebra, and the work string was entered into the hole in the pedicle of the fractured vertebra with the help of the puncture needle as guided by C-arm X-ray examination (Figure 2(f)). Allograft bone was put into the work string (Figure 2(g)) and pushed into the fractured vertebra using a push rod and hollow vertebral drill (Figure 2(h)–2(j)). Upon completion of the bone grafting, the connecting rods and screws were re-locked, and this was confirmed by C-arm X-ray examination (Figure 2(k)). Finally, the caps of the screws were removed (Figure 2(l)), a drainage tube was placed, and the incision was sutured.

Follow-up and observation measures
Follow-up continued for more than 2 years after posterior six-screw fixation. The follow-up schedule is shown in Figure 3. Preoperative, postoperative, and follow-up radiographs were evaluated to determine operative success, assess the presence of “empty” space due to bone loss, and detect potential loosening and breakage of the pedicle screws and rods. The surgical outcomes were recorded, including the incision size, blood loss, operative time, postoperative drainage, hospitalization cost, and postoperative hospital stay. Additionally, the relative height of the fractured vertebra, Cobb angle, visual analog scale (VAS) score, and Oswestry Disability Index (ODI) were assessed preoperatively, postoperatively, and at the last follow-up. The relative height of the fractured vertebra was defined as the percentage of the height of the fractured vertebra relative to that of the normal height of the fractured vertebra, which was calculated according to a formula presented in a previous study. 10 The Cobb angle was measured between the superior endplate of the upper vertebra and the inferior endplate of the lower vertebra. 13 The VAS score (range of 1–10) was used to evaluate low back pain, 14 and the ODI (range of 0%–100%) was used for functional assessment. 14
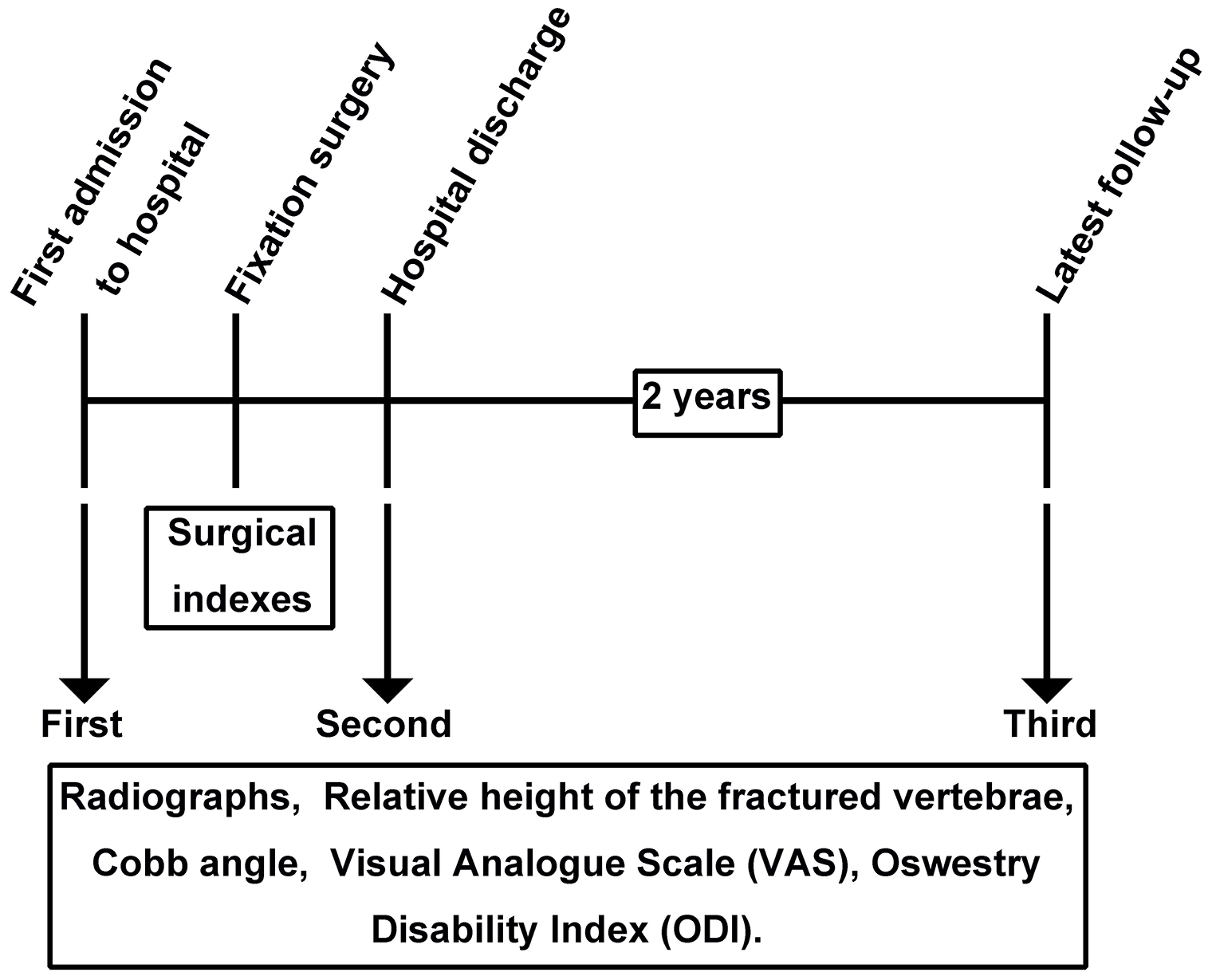
Follow-up schedule.
Statistical analysis
All values are presented as mean and standard deviation, and statistical analyses were performed using SPSS software, version 19.0 (IBM Corp., Armonk, NY, USA). Differences in measurement data between the control group and tool-aided group were evaluated by Student’s t-test, and differences in categorical data between the control group and tool-aided group were evaluated by the chi-square test or Fisher’s exact test. A P value of <0.05 was considered statistically significant.
Results
Baseline patient characteristics
Eighty patients were included at the beginning of the study (40 in the control group and 40 in the tool-aided group). Eight patients in the control group and four patients in the tool-aided group were lost to follow-up; therefore, 68 patients were included in the final analysis (32 in the control group and 36 in the tool-aided group). The control group comprised 14 men and 18 women with a mean age of 49.44 ± 8.94 years. Their fracture levels were T11 (n = 5), T12 (n = 11), L1 (n = 9), and L2 (n = 7), and their AO Spine classifications were A3 (n = 29) and A4 (n = 3). The tool-aided group comprised 20 men and 16 women with a mean age of 51.21 ± 7.97 years. Their fracture levels were T11 (n = 5), T12 (n = 13), L1 (n = 14), and L2 (n = 4), and their AO Spine classifications were A3 (n = 32) and A4 (n = 4). The time from injury to operation, follow-up period, relative heights of the fractured vertebrae, Cobb angle, VAS score, and ODI in the control group and bone grafting group are shown in Table 1. Statistical analyses revealed no significant differences in any of these indices between the two groups.
Baseline patient characteristics.

Data are presented as n or mean ± standard deviation.
TLICS, Thoracolumbar Injury Classification and Severity Score; VAS, visual analog scale; ODI, Oswestry Disability Index.
Surgical outcomes
In the present study, we recorded the incision size, blood loss, operative time, postoperative drainage, hospitalization cost, and postoperative hospital stay. As shown in Table 2, there were no significant differences in the incision size, blood loss, operative time, postoperative drainage, hospitalization cost, or postoperative hospital stay between the two groups.
Surgical outcomes in control group and bone grafting group.

Data are presented as mean ± standard deviation.
CNY, Chinese Yuan.
Radiological results
We collected the preoperative, postoperative, and latest follow-up radiological images in the control group and tool-aided group. In the control group, the lateral X-ray images (Figure 4(a1)), sagittal MRI images (Figure 4(b1)), and sagittal CT images (Figure 4(c1)) indicated an obvious compressed or/and burst fracture. Moreover, the axial CT scan (Figure 4(d1)) revealed obvious bone loss. After traditional surgery, the height of the fractured vertebra was recovered (Figure 4(e1)). However, “empty space” was found after six-screw fixation (Figure 4(e1), 4(f1)), even at the last follow-up (Figure 4(g1), 4(h1)). In the tool-aided group, preoperative bone loss was also observed by lateral X-ray examination (Figure 4(a2)), sagittal MRI examination (Figure 4(b2)), sagittal CT examination (Figure 4(c2)), and axial CT examination (Figure 4(d2)) before six-screw fixation. After these patients underwent tool-aided surgery, the height of the fractured vertebra was recovered (Figure 4(e2)), and the grafted bone was detected (Figure 4(e2), 4(f2)). “Empty space” was rarely found at the latest follow-up (Figure 4(g2), 4(h2)).

Radiological images of control group and bone grafting group. (a) X-ray images, (b) sagittal magnetic resonance images, (c) sagittal CT images, and (d) axial CT images before six-screw fixation. (e) Sagittal CT images and (f) axial CT images after six-screw fixation. (g) Sagittal CT images and (h) axial CT images at the latest follow-up. White arrows indicate “empty space”; red arrows indicate allograft bone. CT, computed tomography.
At the latest follow-up, we found “empty space” in 20 (62.5%) patients in the control group and 8 (22.22%) patients in the bone grafting group, indicating that tool-aided surgery can decrease the formation of “empty space.” We calculated the relative height of the fractured vertebrae and Cobb angle preoperatively, postoperatively, and at the latest follow-up. The relative height of the fractured vertebrae in the control group was 48.09 ± 5.58%, 91.41 ± 3.06%, and 86.16 ± 2.29%, respectively, and that in the tool-aided group was 47.03 ± 5.08%, 92.18 ± 2.28%, and 90.68 ± 2.35%, respectively. Moreover, at the latest follow-up, the relative height of the fractured vertebrae in the tool-aided group was significantly higher than that in the control group (P < 0.05) (Figure 5(a)). These data indicated that tool-aided surgery could better restore the height of the fractured vertebrae. The mean Cobb angle in the control group was 14.69 ± 1.15°, 7.97 ± 0.82°, and 7.66 ± 1.13°, respectively. The mean Cobb angle in the tool-aided group was 14.85 ± 0.82°, 8.00 ± 0.85°, and 7.62 ± 0.60°, respectively. A statistically significant decrease in the Cobb angle after traditional surgery and tool-aided surgery was detected; at each follow-up, however, there was no significant difference in the Cobb angle between the control group and the tool-aided group (Figure 5(b)).
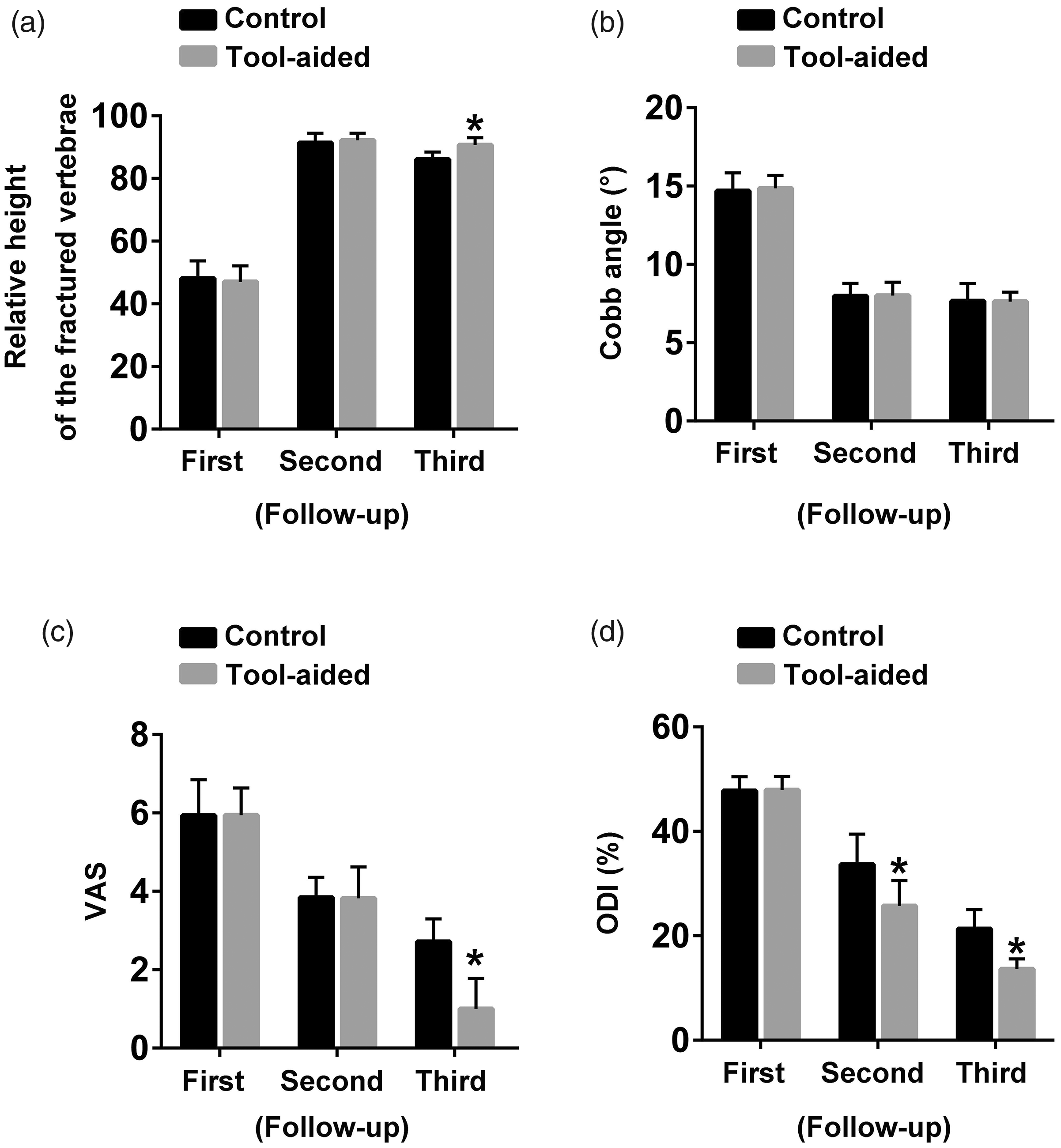
Statistical charts of (a) the relative height of the fractured vertebrae, (b) Cobb angle, (c) VAS score, and (d) ODI. *P < 0.05 vs. control group. VAS, visual analog scale; ODI, Oswestry Disability Index.
Pain and function evaluation
We evaluated the VAS score and ODI preoperatively, postoperatively, and at the latest follow-up. In the control group, we observed a gradual reduction in the VAS score at the first evaluation (5.94 ± 0.91), second evaluation (3.84 ± 0.51), and third evaluation (2.72 ± 0.58). Similarly, in the tool-aided group, we observed a gradual reduction in the VAS score in the first evaluation (5.94 ± 0.69), second evaluation (3.82 ± 0.80), and third evaluation (0.35 ± 0.49). These data indicated that both traditional surgery and tool-aided surgery could improve back pain. Moreover, in the third evaluation, the VAS score was significantly lower in the tool-aided group than in the control group (P < 0.05) (Figure 5(c)), suggesting that tool-aided surgery can better relieve the back pain than traditional surgery. In both groups, we observed a gradual reduction in the ODI in the first evaluation (47.78 ± 2.69% and 47.94 ± 2.57%), second evaluation (33.68 ± 5.82% and 25.71 ± 4.89%), and third evaluation (21.34 ± 3.68% and 13.65 ± 1.94%), indicating that both traditional surgery and tool-aided surgery could improve function. However, in the second and third evaluations, the ODI in the tool-aided group was lower than that in the control group (P < 0.05) (Figure 5(d)), suggesting that tool-aided surgery can better improve function than traditional surgery.
Discussion
The treatment of thoracolumbar fracture is mainly based on its stability and classification. Fracture stability comprises both mechanical stability and neurological stability, and the former depends on whether the PLC is damaged.15,16 Conservative treatment is applied to stable fractures, whereas operative treatment is recommended for unstable fractures. Fractures with neurologic deficits, PLC injury, vertebral height loss of >50%, traumatic kyphosis of >30º, canal compression of >50%, facet fracture, subluxation, or dislocation are regarded as unstable fractures. 15
In patients undergoing operative treatment, internal fixation is often chosen to restore the vertebral body height, correct kyphotic deformity, restore spinal stability, and clear a compromised spinal canal.17 –19 Internal fixation mainly involves a simple anterior approach alone, posterior approach alone, or combined anterior–posterior approach.15,20 An anterior approach can restore the mechanical integrity of the anterior column, remove torn or damaged discs, decompress the spinal canal, and fuse fewer levels of the spine. 15 A posterior approach is well established and has many advantages: simplicity of the posterior midline approach; the lack of pulmonary, visceral, and vascular structures; and clear exposure of the surgical site. 21 Moreover, a combined anterior–posterior approach is recommend when PLC injury is accompanied by incomplete neurological injury, when neurological symptoms persist after posterior approach surgery, or when kyphosis occurs more than 2 weeks after the injury.15,22 The fixation materials include a Gallie wire, Brooks wire, interlaminar clamps, and pedicle screws. 23
During the past few decades, posterior pedicle screw fixation, particularly posterior four-screw fixation, has been one of the most common surgical strategies for treating unstable thoracolumbar fractures.24,25 With the development of posterior four-screw fixation to posterior six-screw fixation, the incidence of screw loosening or breakage has been markedly reduced because in most thoracolumbar fractures, the posterior column at the fracture level remains unbroken and can provide additional points of fixation for posterior six-screw fixation.10,13,26 –28 In addition, placement of pedicle screws in the fractured vertebra can correct kyphosis or horizontal displacement and can share stress from other internal fixations during spinal lateral flexion or rotation. 10 Similarly, in the present study, all enrolled patients with thoracolumbar fractures underwent posterior six-screw fixation. According to the radiological analyses, the relative height of the fractured vertebrae and Cobb angle were corrected after posterior six-screw fixation. Moreover, the patients’ back pain was relieved, the function was restored, and no screw loosening or breakage or rod breakage was detected after posterior six-screw fixation.
Although posterior six-screw fixation provided more adequate anterior column support and sufficient fixation points than posterior four-screw fixation, vertebral body collapse secondary to bone loss, “empty space” formation, and osteoporosis also takes place after screw removal. Hence, many surgeons have attempted to fill the “empty space” of the fractured vertebral body with various grafts or substitutes to restore the stability of the collapsed anterior and central column and even promote bone healing.10,25,29 For example, Van Herck et al. 30 suggested that posterior pedicle screw fixation combined with transpedicular bone grafting efficiently restored the anterior column and preserved the postoperative correction of kyphosis until healing of the fracture. Liao et al. 31 found that transpedicular cancellous bone grafting after posterior short-segment instrumentation remained a reliable surgical method for correcting and maintaining sagittal alignment and vertebral body height in thoracolumbar burst fractures. Moreover, a finite element analysis indicated that additional grafting of calcium sulfate cement after posterior six-screw fixation provided a stiffer construct and less von Mises stress of the pedicle screws and rods as compared with other types of short-segment fixation. 32 In the current study, all patients underwent posterior six-screw fixation combined with transpedicular bone grafting, and a portion of the patients underwent transpedicular bone grafting with the help of the vertebroplasty tool. Before transpedicular bone grafting, we restored the height of the fractured vertebrae and removed the unilateral screw in the level of the fractured vertebrae and unilateral rod. Transpedicular bone grafting was then performed with the aid of the vertebroplasty tool. After completion of bilateral transpedicular bone grafting, the rods were re-installed.
When the height of the compressed vertebrae was restored after posterior six-screw fixation, the fractured vertebrae became loose, and “empty space” even appeared. If this “empty space” is not filled with new bone or bone substitute, the vertebral body may collapse again after screw removal. Many researchers have considered that transpedicular grafting into fractured vertebrae can fill the “empty space” and provide a framework for bone regeneration. However, how to precisely and successfully graft bone substitutes into damaged vertebrae has not been well established. In the present study, we assessed the efficacy of a novel tool to assist transpedicular bone grafting into fractured vertebrae. This novel tool does not contribute much to the effectiveness of six-screw fixation with transpedicular bone grafting, but it facilitates effective and precise grafting of bone into fractured vertebrae, allowing for better restoration of the height of the fractured vertebrae, relief of back pain, and improvement of function. A good postoperative radiological view might not always show that everything is going well. The patient’s clinical condition, such as postoperative chronic pain, disability, and ability to return to his or her previous job, is also important. 33 Although we followed the patients’ postoperative chronic pain and performed function evaluations for 2 years, this is often not enough. Future studies should incorporate more clinical conditions, especially the clinical conditions of patients after screw removal.
Conclusion
We have herein introduced a novel vertebroplasty tool to assist transpedicular bone grafting in posterior six-screw fixation. This tool can effectively restore the vertebral height, relieve back pain, and improve function. Nevertheless, further high-quality studies are warranted to validate the advantages and disadvantages of this method.
Footnotes
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Natural Science Foundation of Chongqing, which funded the first author (Yuetao Wen) (No. cstc2020jcyj-msxmX1005).