
Abstract
Objective
To investigate the clinical efficacy of uni-portal non-coaxial spinal endoscopic surgery combined with Polysorb 4-0 absorbable sutures for repairing ruptured annulus fibrosus in the treatment of lumbar disc herniation.
Methods
We conducted a retrospective study involving 201 patients who underwent uni-portal non-coaxial spinal endoscopic surgery from May 2023 to August 2024 at our institution. Among these patients, 22 were treated using ligamentum flavum suspension surgery while preserving the ligamentum flavum, combined with the annulus fibrosus suture technique. We analyzed the demographic information, preoperative and postoperative imaging data, and clinical outcomes of these 22 patients.
Results
These 22 patients were followed for 6–15 months; at the last follow-up, the improvement in postoperative functional evaluations, such as the Oswestry Disability Index, was statistically significant (P < 0.05). There were two cases of epidural fibrosis at grade 1 and one case of epidural fibrosis at grade 2. There was a slight decrease in disk height. There were no instances of postoperative recurrence, although one patient exhibited postoperative dysesthesia.
Conclusion
Uni-portal non-coaxial spinal endoscopic surgery is straightforward, versatile, and flexible. Preservation of the ligamentum flavum significantly helps prevent epidural fibrosis. Employing Polysorb 4-0 absorbable sutures to repair the annulus fibrosus reduces early recurrence risk, providing satisfactory outcomes for patients with herniated discs. This technique offers a novel and effective treatment alternative for lumbar disc herniation.
Keywords
Introduction
Endoscopic discectomy has become the preferred treatment for lumbar disc herniation (LDH).1–3 However, it still faces complications such as residual nucleus pulposus, herniation recurrence, discitis, and epidural fibrosis, considerably reducing postoperative patient satisfaction. Epidural fibrosis and postoperative recurrence are particularly concerning as they are major contributors to lumbar disc failure.3–5 Currently, there is no established method to prevent epidural fibrosis symptoms post-surgery. Moreover, although various repair techniques aim to reduce the recurrence rate after discectomy, they generally entail high costs and operational risks.6,7 Therefore, we utilized a combination of uni-portal non-coaxial spinal endoscopic surgery (UNSES), also known as arthroscopic-assisted uni-portal spinal surgery, and ligamentum flavum (LF) suspension surgery with preservation of the annulus fibrosus of the LF to treat LDH. We conducted comprehensive clinical assessments before, during, and after surgery to compare pain relief, functional recovery, and other critical indicators, thereby objectively evaluating the efficacy and safety of this technique. In addition, LF suspension preservation combined with the annulus fibrosus suture technique may facilitate the patient’s early return to work after surgery.8,9 This study aimed to explore a safer and more effective minimally invasive surgical pathway for patients with LDH, providing a robust theoretical basis for reducing epidural fibrosis and postoperative recurrence rates, ultimately improving recovery outcomes and enhancing patient quality of life.
Materials and methods
Inclusion and exclusion criteria
A retrospective study was conducted among 201 patients with LDH treated with UNSES from May 2023 to August 2024, of whom 22 were managed using LF suspension surgery while preserving the LF, combined with the annulus fibrosus suture technique. This study received approval from the Ethics Committee of the Second People’s Hospital of Qujing City (NO.2023-010-01), and the need for informed consent was waived for all participants. We have de-identified all patient details, and the reporting of this study conforms to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines. 10
The inclusion criteria were as follows: (a) patients aged ≤60 years without LF hypertrophy or calcification; (b) those requiring surgical treatment after 3–6 months of unsuccessful conservative treatment; (c) those with protruded disc herniation; (d) those with adequate annulus fibrosus attachment and good toughness on both sides of the rupture; (e) those with preoperative lumbar spine positional films showing no lumbar instability; and (f) fibrous annular rupture of ≥5 mm and a rupture margin from the edge of the endplate of ≥2 mm.
The exclusion criteria were as follows: (a) patients with vertebral rim rupture type of disc herniation; (b) those with lumbar spine instability requiring fusion; (c) those with calcified type of disc herniation; and (d) those suffering from severe underlying diseases that preclude surgical tolerance or those with a history of lumbar spine surgery. All procedures were performed by the same operator. Variables recorded included operation time; intraoperative bleeding; incision length; number of intraoperative fluoroscopies; body mass index (BMI); hospitalization duration; preoperative, 1 week postoperative, 3-month follow-up, 6-month follow-up, and final follow-up lumbar and leg pain visual analog scale (VAS) scores; Oswestry Disability Index (ODI); EuroQol-5 Dimension (EQ-5D); epidural fibrosis grade (EFG) 11 ; intervertebral space height; facet preservation rate 12 ; modified Pfirrmann grading 13 ; postoperative complications; and recurrence rates.
Apparatus and equipment
A 4-mm 30° arthroscope, power system, and radiofrequency plasma surgery electrode (Machinery Note Quasi 20172010683, Shanghai Langmai Medical Devices Technology Co. Ltd., Shanghai, China) were utilized for intravertebral canal soft tissue hemostasis and dissection. A bipolar radiofrequency ablation electrode (Guomao Note Quasi 20183010162, Shanghai Langmai Medical Devices Technology Co. Ltd., Shanghai, China) was used for extravertebral canal soft tissue dissection and hemostasis. Suturing was performed using braided absorbable suture Polysorb 4-0.
Surgical techniques
Step 1: Preoperative preparation involved placing the patient in the prone position after satisfactory general anesthesia, abdominal suspension, hip and knee flexion, preoperative C-arm fluoroscopy to determine the responsible segment, skin marking, disinfection, and draping.
Step 2: For exposure, a longitudinal incision (approximately 18 mm in length) was made along the medial edge of the pedicle at the targeted segment (Figure 1(a)), extending to the fascial layer. A “T” type periosteal glass apparatus facilitated subperiosteal dissection at the intersection of the spinous process and centrum. The soft tissue was progressively expanded using a cannula, with subsequent connection of a light source, power system, electrodes, and radiofrequency electrodes. Instruments were inserted through a single incision for the operation (Figure 1(b)). Bipolar radiofrequency was used to excise the root of the spinous process of the superior centrum, intervertebral plate junction, vertebral plate, inferior articular process, and superior articular process. A 4-mm grinder drill was used to remove bone to fully expose the starting and ending points of the LF and articular process.
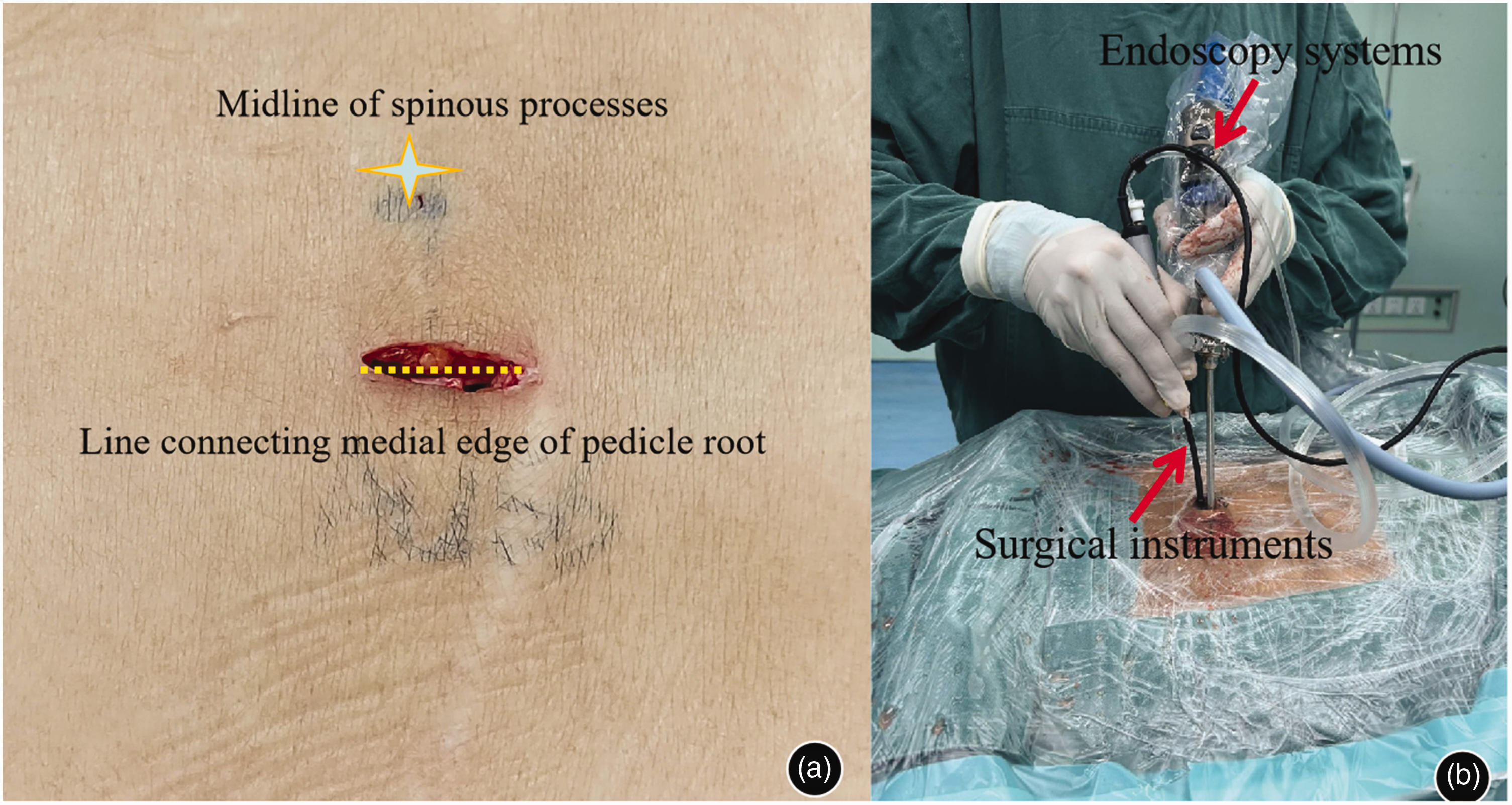
Uni-portal non-coaxial spinal endoscopic surgery (UNSES) incision size and operation diagram. (a) A 18-mm longitudinal incision was made at the midpoint of the vertebral pedicle connection, parallel to the superior vertebral body endplate and (b) Endoscopic and surgical instruments were synergized to complete surgery through a single incision.
Step 3: LF suspension surgery involved using a 2-mm vertebral plate biting bone clamp along the LF starting and stopping points to free the LF, with a needle 4-0 absorbable suture placed on the LF without tying the knot. The suture line was clamped with a vascular clamp to maintain tension, effectively lifting the LF (Figure 2).

Illustration of ligamentum flavum (LF) suspension surgery performed under uni-portal non-coaxial spinal endoscopic surgery (UNSES). First, the original and caudal LF and the attachment site of the zygapophyseal joint were thoroughly exposed. The LF was carefully freed using a 1-mm vertebral plate biting forceps, and the LF was subsequently suspended using a 4-0 absorbable suture.
Step 4: Pre-hemostasis and loosening of adhesions were performed using radiofrequency plasma surgical electrodes to maintain a clear surgical view.
Step 5: Evaluation of the annulus fibrosus breach involved fully exposing the head and tail sides of the annulus fibrosus, assessing the distance from the endplates, and evaluating the strength of the annulus fibrosus. A longitudinal incision was made along the weak point with a 15-gauge sharp knife to remove the diseased nucleus pulposus (Figure 3).

Illustration of an incision of the annulus fibrosus. For patients with inclusive disc herniation, the annulus fibrosus was incised longitudinally at its weak point.
Step 6: Closing the annulus fibrosus breach with a 4-0 absorbable suture: After excision of the diseased nucleus pulposus tissue and radiofrequency ablation of the disc, the size of the annulus fibrosus breach, the distance from the upper and lower endplates, and the strength of the annulus fibrosus were reassessed. A nerve stripper was used to loosen the adhesive band on the ventral side of the nerve root, which was then retracted to the contralateral side using a 2.0 Gram’s needle or a nerve-pulling hook. A choice of single-needle, parallel double-needle, crossed double-needle, or multiple-needle sutures was made to close the annulus fibrosus, positioning the knot on the dural sac or the lateral side of the nerve root to prevent irritation (Figure 4).

Surgical illustration of suturing the annulus fibrosus rupture, which can be performed with one or two or more sutures. (a) One-needle suture and (b) double-needle suture.
Step 7: The LF was trimmed with 3-mm 130° laminar bite forceps to create a “flap” and then retracted, after which a drain placed to conclude the procedure (Figure 5).

Illustration of a surgical procedure for retracting the ligamentum flavum (LF), which may be closed with one or two or more sutures. (a) Double-needle suture and (b) the LF was returned in situ.
Statistical methods
Statistical analysis was performed using GraphPrism 10.0 (GraphPad Software, Inc., USA). Data were tested for normality; non-normally distributed data were expressed as medians and normally distributed data as mean ± standard deviation (SD). Categorical variables were presented as frequencies and percentages. The Wilcoxon test was used to compare differences between two time points before and after surgery, with P < 0.05 considered to indicate statistical significance.
Results
Patient characteristics
Among the 201 patients undergoing endoscopic surgery, 22 were treated with UNSES LF suspension surgery while preserving the LF as well as the annulus fibrosus suture technique. This group comprised 11 males and 11 females, with 16 patients treated at L4–L5 and 6 at L5–S1. Patient ages ranged from 26 to 60 years, with the mean age of 52.3 years and BMI of 24.3 ± 3.7 kg/m2 (Table 1).
Patient demographic and clinical characteristics.

Values are presented as mean ± standard deviation or number (%).
BMI: body mass index.
Intraoperative data and postoperative evaluation
The 22 patients underwent single-level discectomy, with an operation time of 84.2 ± 15.8 min, bleeding volume of 59.1 ± 11.4 mL, and hospital stay of 4–8 (average: 6.2) days. The follow-up period was 6–15 (average: 11.3) months. The incision length was 18.2 ± 1.8 mm, and the number of intraoperative fluoroscopies was 4.3 ± 0.9. Suture techniques included nine single-needle, seven parallel double-needle, four crossed double-needle, and two multiple-needle cases. No recurrences or reoperations were reported during follow-up. The facet preservation rate on the access side was 83.7% ± 6.1%. No significant difference was observed between the modified Pfirrmann grades preoperatively and those at the last follow-up (P = 0.157). However, the difference in disk height from preoperative measurements was statistically significant (P < 0.0001). EFG grades were distributed as follows: grade 0, 81.8% (18/22); grade 1, 9.1% (2/22); and grade 2, 4.5% (1/22) (Table 2). Compared with preoperative scores, the postoperative VAS score, ODI, and EQ-5D scores for low back and leg pain showed significant improvements at each time point, with statistically significant differences in pairwise comparisons (P < 0.05) (Table 3, Figure 6). One patient developed postoperative dysesthesia, which was alleviated after 6 months following nutritional neurotherapy. Treatment efficacy, evaluated using the modified MacNab criteria, was rated as excellent in 19 cases, good in 1 case, and moderate in 1 case, with an excellent rate of 90.9%.
Intraoperative data and postoperative imaging evaluation.

Values are presented as mean ± standard deviation or number (%).
DH: disc height.
Preoperative and postoperative evaluation.

Values are presented as mean ± standard deviation.
EQ-5D: EuroQol-5 Dimension; ODI: Oswestry Disability Index; VAS: visual analog scale.
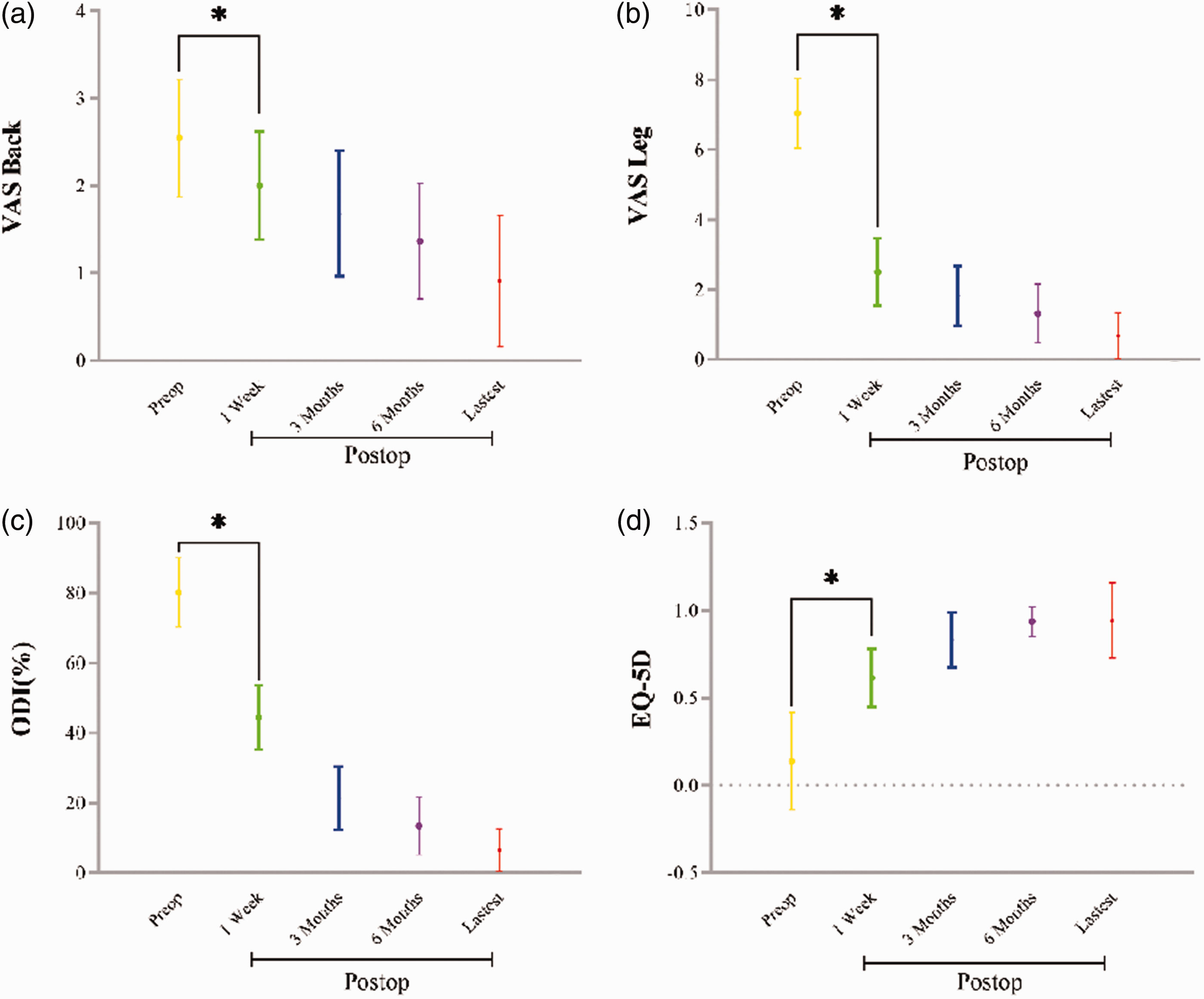
Evaluation of the postoperative outcome of the combination of uni-portal non-coaxial spinal endoscopic surgery (UNSES) ligamentum flavum (LF) suspension surgery with LF preservation and fiber ring annulus fibrosus suturing. (a) Visual analog scale (VAS) score for back pain. (b) VAS score for leg pain. (c) Results of the Oswestry Dysfunction Index (ODI) and (d) results of the EuroQol-5 (EQ-5D) self-reported questionnaires. *P < 0.05 indicated a statistically significant difference.
Discussion
The preservation of the LF is clinically significant in the surgical treatment of LDH. Serving as a natural anatomical barrier, the LF, when preserved, reverts to its original position more effectively after surgery. This ensures the complete separation of the vertebral canal from the extraspinal scar tissue, maintaining the anatomical integrity of the vertebral canal and effectively preventing the invasion of extraspinal scar tissue. The smooth LF, adhering to the intact epidural fat, shows no signs of traumatic inflammatory reactions, necrotic tissue, or foreign matter, which significantly reduces epidural scar adhesion.14–16 In this study, the retention of the LF contributed to a reduction in postoperative complications and enhanced the success rate of surgical treatments. Furthermore, LF preservation positively affected postoperative disc conditions, improving patient outcomes after subsequent interventions. 17 At the final follow-up, the EFG grades were distributed as follows: grade 0, 81.8% (18/22); grade 1, 9.1% (2/22); and grade 2, 4.5% (1/22), demonstrating the positive role of the LF in preventing epidural fibrosis (Figure 7).

Combination of uni-portal non-coaxial spinal endoscopic surgery (UNSES) and ligamentum flavum (LF) suspension surgery with preservation of the LF syndesmosum annulus fibrosus and suture closure. Comparison of preoperative and 1-year postoperative magnetic resonance imaging showed the following results: (a) no hypertrophy of the LF was seen preoperatively and (b) at 1 year postoperatively, the epidural fibrosis was graded as grade 0.
The annulus fibrosus suture technique effectively repairs ruptures in the intervertebral disc, promotes the healing of the annulus fibrosus, and reduces the re-protrusion of disc content, thereby lowering the recurrence rate of herniated disc. This method preserves the structural integrity of the intervertebral disc and maintains its physiological function. Yasargil et al. 18 employed a 7-0 suture under microscopic guidance as early as 1977, with no recurrence of disc herniation postoperatively. Cauthen et al. 19 observed that without annulus fibrosus sutures, the 2-year postoperative recurrence rate was 21%; however, a single suture reduced the rate to 10%, and a double suture further reduced it to 5%. Bailey et al. 20 implemented the “X-close” technique after lumbar disc removal, which significantly decreased the recurrence rate. Additionally, the “Barricade”21,22 annulus fibrosus occluder has been used by some scholars to maintain disc height and physiological function while reducing the incidence of postoperative low back and radicular pain. In this study, a 4-0 absorbable suture was employed, with nine cases of single-needle, seven of parallel double-needle, four of crossed double-needle, and two of multiple-needle sutures, and no recurrences were noted over an average follow-up period of 11.3 months. At the final follow-up, a significant decrease was observed in the intervertebral space height compared with preoperative measurements (P < 0.05); however, this did not adversely affect the clinical outcomes of the patients, aligning with the existing literature. 23 The change in modified Pfirrmann grading was not significant (P > 0.05).
UNSES has increasingly demonstrated its broad application potential in spinal disorder treatments since its introduction by Prof. En Song in 2021.24–26 The technique has garnered attention from the industry owing to its inclusivity, versatility, and significant reduction potential in intraoperative fluoroscopies. Within the same surgical incision, UNSES not only facilitates the suspension preservation of the LF but also closes the annulus fibrosus breach in cases of lumbar disc herniation using a 4-0 absorbable suture, either through single or multiple sutures, effectively reducing the recurrence rate. In addition, the technological learning curve of this method is shorter than that of uni-portal spinal endoscopy 27 and relatively longer than that of unilateral biportal endoscopy. 28 Surgeons with experience in both endoscopic and open surgery learn UNSES more quickly.
Furthermore, the UNSES technique maintains a high facet preservation rate on the access side, which was 83.7% ± 6.1% in this study, without compromising iatrogenic stability. The technique’s minimally invasive nature accelerates the rehabilitation process, substantially enhancing patient satisfaction. Although no control group was established in this study, the UNSES technique has proven to be safe, reliable, and effective. This finding provides a solid basis for future multicenter, prospective, randomized controlled trials, which are anticipated to offer higher levels of evidence for the safety and efficacy of the UNSES technique.
Conclusion
UNSES is easy to perform, offering flexibility and effectively reducing the need for intraoperative fluoroscopy. LF suspension surgery is effective in preventing dural cystic fibrosis and reducing the formation of dural cystic scars through LF preservation. The use of Polysorb 4-0 absorbable sutures to close the annulus fibrosus not only proves feasible but also minimizes the risk of recurrence and mitigates early-stage nerve root irritation by inhibiting the release of inflammatory mediators, yielding satisfactory results for patients with disc herniation. This technique may offer a novel and effective treatment alternative for patients with LDH.
Footnotes
Acknowledgements
We are obliged to En Song for conducting discussions and providing technical guidance.
Authors’ contributions
Yongneng Li wrote the manuscript and interpreted the data. Lihui Fu proposed the study’s design, obtained data, and performed analysis and interpretation. Yongqiang Yang measured and analyzed radiological outcomes, and Shuwen Kan constructed the schematic diagram. En Song provided technical guidance. Yongneng Li and En Song assisted with the revision and preparation of the manuscript for publication. All authors read and approved the final manuscript.
Data availability statement
All data are available within this article.
Declaration of conflicting interests
The authors declare that there are no conflicts of interest.
Funding
This work was supported by Yunnan Health Training Project of High Level Talents (H-2024084) and Yunnan Revitalization Talent Support Program; DCMST.NHC Clinical Research Project (WKZX2024JZ0122).