
Abstract
Objective
This study aimed to evaluate the perceived stress and anxiety levels of patients undergoing coronary angiography and examine the impact of the procedure area on these psychological factors.
Methods
A total of 144 patients were included, and data were collected using the Personal Information Form, State–Trait Anxiety Scale, and Perceived Stress Scale. Statistical analyses were performed using IBM SPSS Statistics 23, along with independent sample t-tests, one-way analysis of variance, Levene’s test, post-hoc tests, Pearson correlation, and Cronbach’s alpha for reliability.
Results
The mean patient age was 54.31 ± 12.50 years; 63.2% of them were male. Overall, 58.3% of the patients underwent coronary angiography for diagnostic purposes, and 61.8% were aware of the procedure area. State anxiety, trait anxiety, and perceived stress scores were 46.78 ± 11.81, 41.35 ± 9.98, and 16.74 ± 5.32, respectively. Higher anxiety was observed among patients unaware of their diagnosis and those undergoing repeat coronary angiography. Patients who were undergoing femoral angiography had higher perceived stress than those undergoing angiography through the radial route.
Conclusion
Uncertainty about diagnosis and the procedure increases stress and anxiety. Providing preprocedural education during coronary angiography and exploring alternative anxiety management strategies, such as mindfulness, could enhance patient experience and recovery.
Introduction
The coronary arteries are the main vessels that supply the heart with blood. Because of the narrowing or blockage of these vessels, the heart cannot be adequately nourished and cannot fully fulfill its function. This condition is known as coronary artery disease (CAD). 1
CAD is the most important morbidity problem in developed societies. For example, it accounts for 42% of all deaths in the US adult population. 2 In Turkey, according to the “Heart Health and Risk Factors in Turkish Adults (TEKHARF)” study, 400,000–420,000 patients are newly diagnosed with CAD within 1 year, and 340,000 adults die within 1 year. 3 Coronary angiography (CAG) is the most commonly used and reliable diagnostic test for CAD. 4 According to the Turkish Society of Cardiology, CAG is the most accurate diagnostic method. In another study, CAG was clinically accepted as the gold standard for diagnosing CAD, which has an important place in terms of individual and public health. 5
Stress negatively affects a person’s normal functions, and prolonged exposure to stress can also cause various health problems and even negatively affect a person’s functioning and quality of life. 6 Perceived stress refers to the feelings and thoughts of an individual regarding how stressed they are at a certain time or in a certain situation. Perceived stress involves how much control a person has over their life, how they can cope with difficulties, and their self-confidence in this regard. 7
Conversely, anxiety refers to a feeling of being overwhelmed with the fear of the unknown and the worry that something bad will happen. By definition, it refers to a feeling of distress and sadness. Anxiety can be categorized into mild, moderate, severe, and panic levels. Moreover, it is categorized as trait anxiety and state anxiety. State anxiety determines how individuals feel at a given moment; trait anxiety determines how individuals feel independent of the current situation.8–11
Individuals undergoing CAG may experience anxiety due to the following reasons: (a) insufficient information about the procedure; (b) the fact that it is an interventional procedure; (c) the possibility of a new diagnosis that may be life-threatening; and (d) the risk of developing complications related to the procedure. In addition, the presence of pressurized dressing and sandbags in the intervention area may cause pain in this area.3,12,13
Therefore, this study aimed to determine the perceived stress and anxiety levels of patients undergoing CAG, with the research question focusing on whether the procedure area and patient awareness of the diagnosis influence these psychological factors.
Methods
This study was designed as a prospective observational, cross-sectional single-center study. The reporting of this study conforms to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines. 14 The study protocol was approved by the Health Sciences University Derince Training and Research Hospital Clinical Research Ethics Committee (approval no: 2022-129). The study population consisted of patients admitted to the coronary intensive care units of Derince Training and Research Hospital between 1 December 2022 and 1 December 2023. The study sample consisted of 144 patients (91 men and 53 women) who consented to participate in the study and who met the research criteria (i.e. patients over 18 years of age and those who were fully oriented to person, place, and time and were willing to participate in the study). Patients signed an informed consent form before participating in the study. The questionnaires were administered to patients admitted to the coronary intensive care unit prior to undergoing CAG. Patients aged <18 years and those with incomplete data on orientation to person, place, and time were excluded from the study.
Study protocol
Personal Information Form, Perceived Stress Scale (PSS), and State–Trait Anxiety Scale were used by the researchers after reviewing the relevant literature.
Personal Information Form
The Personal Information Form was used to obtain information such as age, sex, education level, height/weight, marital status, duration of hospitalization, any chronic disease status, smoking/alcohol habits, history of CAG, and current knowledge of CAG.
PSS
PSS was developed by Cohen et al. 15 in 1983, with a Cronbach’s alpha value of 0.86. It was adapted into Turkish by Bilge et al. 16 in 2009, with a Cronbach’s alpha value of 0.81. The scale has two subscales: perceived stress (1st, 2nd, 3rd, 7th, and 8th items) and perceived coping (4th, 5th, and 6th items). The 1st, 2nd, 3rd, 7th, and 8th items are straight items, whereas the 4th, 5th, and 6th items are reverse items. The evaluation is conducted based on the total score and subscale score. Individuals are given five options to answer (0 (not at all) to 4 (very often)), and scores between 0 and 32 are obtained. If the total score is high, the perceived stress level is also high. High scores on the subscales indicate a negative situation. A total score of 0–32 is obtained from the scale. A high total score indicates a high perceived stress level. A high score in the subscales indicates a negative situation. 15
State–Trait Anxiety Scale
State–Trait Anxiety Scale is an assessment scale developed by Spielberger et al. 11 to measure both dimensions of anxiety. The scale aims to assess state and trait anxiety separately. State anxiety determines how individuals feel at a given moment; trait anxiety determines how individuals feel independent of the current situation. 16 The Turkish validity and reliability study was conducted by Oner and Compte, 9 and Cronbach’s alpha coefficients were found to be 0.83–0.92 for the state anxiety scale and 0.86–0.92 for the trait anxiety scale. There are two separate scales for the two states in the scale. The STAI-I scale measures state anxiety, while the STAI-II scale measures trait anxiety. Each item in the scale is evaluated by individuals by providing scores between 1 and 4. Response options are categorized into four classes. In the state anxiety scale, the grades are as follows: not at all (1), a little (2), a lot (3), and completely (4). The options in the trait anxiety scale are as follows: almost never (1), sometimes (2), very often (3), and almost always (4). When scoring, responses with a value of 4 in direct statements indicate high anxiety, whereas responses with a value of 1 in reverse statements indicate high anxiety. There are 10 reversed statements in the state anxiety scale (items 1, 2, 5, 8, 10, 11, 15, 16, 19, and 20). The number of reversed statements in the trait anxiety scale (items 21, 26, 27, 30, 33, 36, and 39) is seven. During the evaluation, two keys are created for direct and reversed statements, and their total weights are found. From the total weighted score obtained for the direct statements, the total weighted score of the reversed statements is subtracted, after which 50 points for the state anxiety scale and 35 points for the trait anxiety scale are added to this number. These values are predetermined and unchangeable. The higher the sum of the scores, the higher the level of state and trait anxiety. The average score level determined in the applications is between 36 and 41. 9
Ethical aspects of research
Ethics Committee Approval (No: 2022-129) was obtained from the Health Sciences University Derince Training and Research Hospital Clinical Research Ethics Committee, and institutional permissions were obtained from the hospital where the study was conducted.
Statistical analysis
Data analysis was performed using IBM SPSS Statistics 23 program. Frequency distribution (number, percentage) for categorical variables and descriptive statistics (mean, standard deviation, minimum, and maximum) for numerical variables were used to evaluate the data. The difference between the two groups was analyzed via independent sample t-test, and the difference between more than two groups was analyzed via one-way analysis of variance (ANOVA). Because of one-way ANOVA, Levene’s test was performed for homogeneity of variance, after which the group or groups from which the difference originated were checked by a multiple comparison test (Bonferroni or Tamhane’s T2). Bonferroni test was used to examine the difference between groups in variables that provided homogeneity of variance, and Tamhane’s T2 test was used to examine the difference between groups in variables that did not provide homogeneity of variance. Pearson correlation analysis was used to examine the relationship between the scales, and Cronbach alpha value was used for scale reliability.
Results
Participants’ demographic characteristics, health history characteristics, and characteristics of angiography status (N = 144)
Table 1 presents patient demographic, health, and angiography characteristics.
Participants’ health demographic characteristics, health history characteristics, and characteristics of angiography status (N = 144).

HT: hypertension; DM: diabetes mellitus; CAD: coronary artery disease; CAG: coronary angiography.
Descriptive statistics of participants’ State–Trait Anxiety Scale scores and PSS and its subscale scores
The state anxiety scale score was 46.78 ± 11.81, the trait anxiety scale score was 41.35 ± 9.98, and the PSS score was 16.74 ± 5.32. The perceived stress subscale score was 11.24 + 4.08, and the perceived coping subscale score was 5.51 + 1.84. Participants had a moderate level of anxiety according to their mean scores. They were compatible with a moderate level of perceived stress and could not use effective stress management.
State–Trait Anxiety Scale scores as well as PSS and its subscale scores were higher in women than in men. Therefore, women had higher anxiety and worry. Trait anxiety scores were statistically significantly higher in patients with a lower education level than in those with higher education levels. The state anxiety scale score was higher in patients whose income was more than their expenses than in those whose income was less than their expenses. Individuals with better income had higher anxiety about angiography. The perceived coping subscale score was higher in patients living with their children than in patients living alone. Accordingly, patients living with their children tended to cope less with anxiety. The trait anxiety scale score was higher in nonworking individuals than in working individuals. In this case, nonworking individuals were more anxious than working individuals. The state anxiety scale score was higher in smokers than in nonsmokers, and the trait anxiety scale score was higher in nonsmokers than in smokers. According to these results, patients who smoked had higher state anxiety about angiography, whereas patients who consumed alcohol had lower anxiety levels than those who did not consume alcohol. There was a statistically significant difference in these results (p < 0.05; Table 2).
Examination of the relationship between the State–Trait Anxiety Scale, Perceived Stress Scale and its subscales, and demographic characteristics of the participants.

F: one-way analysis of variance; t: independent sample t-test; *: p < 0.05.
a, b: mean differences between groups (a: highest mean).
There was a statistically significant difference between the status of knowing the diagnosis and the reasons for CAG in terms of state anxiety scale score (p < 0.05). Accordingly, the state anxiety scale score was higher in patients who did not know the diagnosis than in those who did. In addition, the state anxiety scale score was higher in patients whose reason for CAG was control purposes than in those whose reason for CAG was interventional purposes. Accordingly, patients who did not know their diagnosis had higher anxiety about angiography. Patients who underwent angiography for control purposes had higher anxiety than those who underwent interventional angiography. There was no statistically significant difference between diagnoses, history of other diseases, medication use, number of medications used, history of CAD diagnosis in the family, place of admission, hospitalization due to CAD, number of hospitalizations due to CAD, history of CAD in the family, and number of CAD procedures in terms of all scale and subscale scores (p > 0.05). Accordingly, family history of CAD did not affect the level of anxiety and perceived stress (Table 3).
Examination of the relationship between the State–Trait Anxiety Scale, Perceived Stress Scale and its subscales, and health history characteristics of the participants.

F: one-way analysis of variance; t: independent sample t-test; *: p < 0.05
a, b: mean differences between groups (a: highest mean).
CAD: coronary artery disease; CAG: coronary angiography.
There was a statistically significant difference in the PSS and its subscale scores between the site of angiography and the site preferred for angiography (p < 0.05). Specifically, patients who underwent angiography through the femoral route exhibited higher PSS and its subscale scores than those who underwent angiography through the radial route. Similarly, patients who preferred the femoral route for angiography had higher PSS and its subscale scores than those who preferred the radial route. These results indicate that patients who underwent angiography through the femoral route as well as those who preferred the femoral site experienced higher levels of stress.
However, there was no statistically significant difference in PSS and its subscale scores or State–Trait Anxiety Scale scores between the region of previous angiography and the knowledge of the angiography site (p > 0.05).
A statistically significant difference (p < 0.05) was found in state anxiety scale scores based on the conditions of receiving information about the angiography procedure, the timing of receiving this information, and the source of information. Specifically, patients who did not receive information about the angiography procedure had higher state anxiety scores than those who did. Furthermore, patients who received information about the angiography while on their way to the procedure had higher anxiety scores than those who were informed earlier, before knowing how the exact procedure would take place. Additionally, patients who received information from friends, neighbors, or relatives had higher anxiety scores than those who received information from a physician.
These findings suggest that the anxiety levels of patients who were not informed or received late or less reliable information were higher. Moreover, there was a significant difference (p < 0.05) between patients who knew the time of their angiography and those who did not, with the latter group showing higher State–Trait Anxiety Scale scores. This indicates that the uncertainty regarding the timing of the angiography procedure contributes to increased anxiety (Table 4).
Examination of the relationship between the State–Trait Anxiety Scale, Perceived Stress Scale and its subscales, and participants' characteristics regarding angiography conditions.
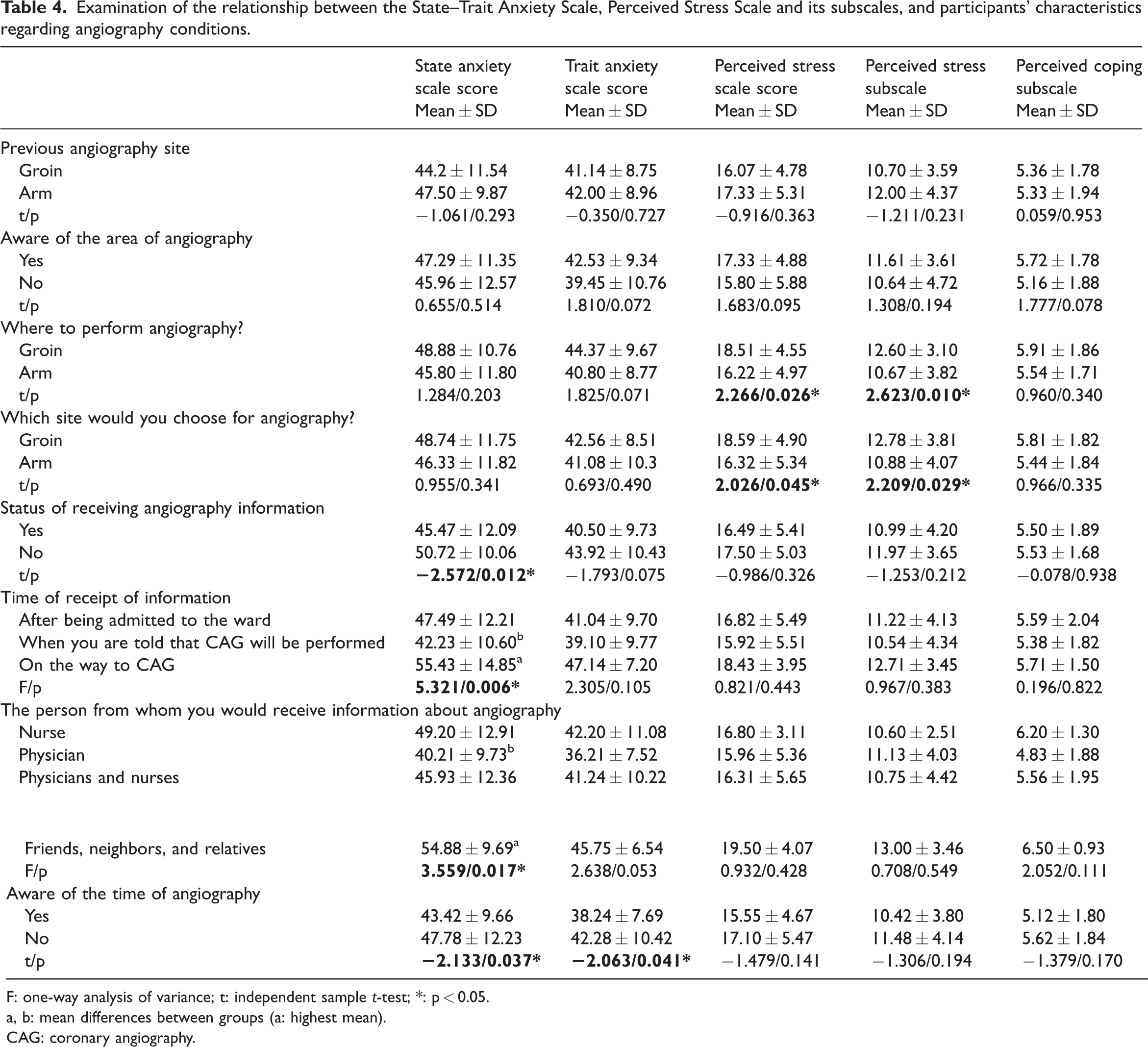
F: one-way analysis of variance; t: independent sample t-test; *: p < 0.05.
a, b: mean differences between groups (a: highest mean).
CAG: coronary angiography.
There is a statistically significant positive correlation between State–Trait Anxiety Scale scores and PSS and its subscale scores (p < 0.05). In this context, if state and trait anxiety increases, perceived stress also increases (Table 5).
Examination of the relationship between the State–Trait Anxiety Scale and Perceived Stress Scale and its subscales.

r: Pearson correlation coefficient; *: p < 0.05.
Discussion
Our study found that patients who underwent CAG through the femoral route experienced significantly higher perceived stress levels than those who underwent the procedure via the radial route. Additionally, patients who were not informed about the procedure experienced higher anxiety levels, especially those who received information at the time of angiography or from nonmedical sources. We also observed that smoking was associated with higher anxiety levels, and patients who were unaware of the time of their angiography had elevated anxiety levels.
CAG enables the identification and simultaneous treatment of CADs. Therefore, it has become a frequently used method worldwide, and the number of studies on this subject is increasing.5,17
It has been reported that men are more likely to develop CAD than women, but the prognosis is worse and morbidity is higher in women.18,19 In this study, the majority (63.2%) of the patients undergoing CAG were male. However, in the study conducted by Özdemir et al., 20 the majority of patients were female. When the literature was examined, it was concluded that the number of male individuals was higher in most studies similar to this study.3,21–24
In this study, anxiety levels and anxiety scores in all scales were found to be higher in women than in men. In the study of Yel and Ünsar, 3 the trait anxiety score of women and the anxiety score of women in the study of Atik et al. 24 were found to be higher compared with men. These results are in parallel with the study. In contrast to these findings, there are studies in which men’s state–trait anxiety scores were found to be higher than women’s.5,25 It is thought that the reason for the higher anxiety and anxiety levels of women in the study may be that women have a more sensitive structure, have a greater sense of responsibility, and think in more detail.
In this study, which aimed to determine the anxiety status and anxiety level of the patients before angiography, the State–Trait Anxiety Scale scores were found to be moderate, and the PSS score was also found to be moderate. Although these results are close to the results of other studies, differences are likely to occur due to factors such as patient profile and sample size.3,26,27
In this study, the trait anxiety score was found to be higher in the group with an educational level of primary school and below than in the group with an educational level of university and above. In studies investigating the effect of education level on anxiety level before CAG in the literature, Ali 23 found that anxiety levels decreased as the education level increased, consistent with the finding of Yel and Ünsar. 3 It is believed that this result is related to knowing the methods of coping with stress through increasing education level and health literacy, performing good disease management, enhancing adherence to treatment, and making conscious decisions in lifestyle planning.
When the anxiety levels of the patients were examined according to their income status, it was found that the state anxiety score was higher in those whose income status was higher than the expense status. In the study by Bural Aydın, 28 the state anxiety of patients whose income was equal to their expenses was found to be lower than that of patients whose income was less than their expenses. The disease, the process of hospitalization and surgery, and the fear of the unknown caused by this process increase both the information and counseling needs of patients. Although this is especially important for patients with low levels of education and income, patients with high levels of education and good income can also experience the same anxiety and fear.
In our study, when cohabitants and anxiety were analyzed, it was found that people living with their children were less capable of coping with anxiety than people living alone. It was believed that although children provide life support to individuals, these individuals could not cope with anxiety due to the sense of responsibility felt toward them. In the study conducted by Karabiber and Dığın, 29 no significant association was found between cohabitants and anxiety. These distinct results may be related to sample diversity across studies.
In this study, the trait anxiety scale score of patients who were not working was higher than that of working patients, whereas in the study conducted by Atik et al., 24 the anxiety score was higher in working patients. Accordingly, the trait anxiety scale score of patients who were not working was higher; this may be due to the lack of social support received away from their working life or their financial needs.
When the relationship between smoking and CAG was analyzed in terms of anxiety level, it was found that the state anxiety score was higher in smokers than in nonsmokers. Similarly, in the literature, it was found that the anxiety score of smokers was higher than that of nonsmokers. 30 Smoking, which is a risk factor for CAD,31,32 also causes stress. Moreover, we can attribute the high anxiety of smokers about angiography to the fact that patients are aware that smoking negatively affects their health and therefore feel anxiety.
When the relationship between alcohol use and CAG was examined in terms of anxiety level, it was found that the level of trait anxiety was higher in nonalcohol users than in alcohol users. In this case, the anxiety level of alcohol users was lower than that of nonalcohol users. The reason for the low level of anxiety in alcohol users may be related to the demographic and personality characteristics of the patients.
Most of the participants in the study were aware of their diagnosis, but those who did not know about their diagnosis had higher state anxiety scale scores than those who did. Unawareness of their diagnosis, fear of the unknown, and having no idea about the angiography procedure may have contributed to this result by causing tension.
When the site of angiography and anxiety status were examined, it was found that patients who underwent angiography through the femoral route had higher scores on PSS and its subscales than those who underwent angiography through the radial route. In the study by Çiraci 33 investigating the comfort levels of patients who underwent angiography through the radial and femoral routes, it was found that the comfort level of those who underwent angiography through the radial route was higher than that of patients who underwent angiography through the femoral route, and the relaxation and spaciousness scores were also higher in those who underwent angiography through the radial route. Based on this, it was believed that increasing the comfort level of the patients would contribute to a decrease in anxiety. In addition, when the literature was examined, it was found that angiography through the femoral route is frequently performed; however, after the procedure, sandbags should be placed for compression, patients should be lying flat for a long time, and occurrence of too much lying flat on the bed should be low; prolonged bed rest may cause back pain, procedure site pain, and leg pain. Pain and anxiety are interactive sources of stress. 24 In the study conducted by Cihan, 34 the comfort level of patients who underwent angiography through the radial route and patients with shorter bed rest were found to have a higher comfort level. This explains the higher anxiety of patients who underwent angiography through the femoral route.
In the study, patients who preferred the femoral region as the site of angiography had higher PSS and subscale scores than those who preferred the radial region. It is known that manual and sandbag compression is very common in the literature, but this practice greatly impairs patient comfort. 35 For this reason, it can be said that the PSS and its subgroups are high in patients whose angiography preference is femoral. Conversely, it can be said that the reason why these patients do not prefer the radial route is that the pain sensation is felt more in this region, because the radial vessel diameters are smaller and superficial.
In the study conducted by Fındık and Yıldızeli Topçu, 36 it was observed that the information given before surgery reduced anxiety. In the literature, there are studies showing that the anxiety level of people who did not receive information about CAG was higher than those who did.21,23 In our study, the results parallel to this information were obtained. According to the results, it was determined that the state anxiety scale score of people who did not receive information about CAG was higher than those who received information. This result shows that patients who were not informed were more anxious. When individuals think that there will be a procedure related to the heart, which is a very important organ for life, and when this is accompanied by the fear of death, their anxiety may be high. Increased anxiety can negatively affect the cardiovascular system. Patients are confused by misinformation and bad experiences heard from others. Not knowing how the procedure will be performed, where it will be performed and the environment causes fear. For all these reasons, patients should be given timely and complete information about the procedure.
In the study, when the patients were informed also affected the level of anxiety; the state anxiety scale score of those who received information on the way to angiography was higher than those who received information when they were told that angiography would be performed. In the study by Gören, 25 the state–trait scale score of those who received information after being admitted to the ward was higher than those who received information when they were told that angiography would be performed. As the information given to patients reduces anxiety, the time of giving information is also important for the patient to prepare himself/herself for the process. It is thought that timely information for patients to feel physically and emotionally ready will reduce the level of anxiety.
The anxiety level in patients who did not know what time they would be admitted to angiography was found to be higher than those who knew. In parallel with this in Gören 25 study, the state–trait anxiety score of patients who knew the procedure time was found to be lower than those who did not know. It was observed that fear of the unknown increased anxiety in patients. In addition, studies have found that patients experience significant anxiety before angiography and that having angiography increases fear and anxiety.27,36,37 It is known that the anxiety experienced by patients before CAG also causes hemodynamic changes. 38 In this case, patient’s knowledge of the time of angiography was found to be an important factor affecting the level of anxiety, and it was seen that informing the patient before angiography is important.
In the study conducted by Cihan, 34 it was found that the comfort level of people who received information from the physician was higher, and it was determined that patients felt better when they received information from the physician. Among people who received information in the study, those who received information from friends, neighbors, and relatives had higher state anxiety scale scores than those who received information from physicians. The reason for this may be interpreted as not providing objective information, giving wrong information, or having bad experiences. In addition, the fact that nurses spend less time giving information creates the perception that they have less information on patients. Therefore, nurses, who have the closest communication with patients, should provide information to create a bond of trust and complete the lack of information of patients.
This study provides valuable insights into the psychological well-being of patients undergoing CAG, highlighting the influence of both the procedural approach (femoral vs. radial) and the timing of information delivery on anxiety levels. The findings emphasize the practical importance of early and accurate patient education, which appears to play a significant role in reducing preprocedural anxiety. This underlines the need for healthcare professionals to integrate psychological considerations into patient care and adopt communication strategies that foster trust and emotional preparedness before medical procedures.
Nevertheless, this study had limitations. The relatively small sample size may limit the generalizability of the findings to a broader patient population. Expanding the sample and including a more diverse demographic would strengthen the conclusions and enhance their applicability across different patient groups. Additionally, the cross-sectional design restricts the ability to establish causal relationships between the studied variables. Future longitudinal research would be particularly useful in examining the long-term effects of anxiety reduction on patient recovery and procedural outcomes. Another limitation is the reliance on self-reported data to assess anxiety, which can introduce subjective bias or inaccuracies. Incorporating objective measurements or physiological markers in future studies could provide a more comprehensive and reliable assessment of patient anxiety.
Although this study sheds light on the underexplored psychological dimensions of CAG, it also underscores the need for further research involving larger samples, longitudinal approaches, and multimethod anxiety assessments. Such research would not only deepen the understanding of patient experiences but also guide the development of effective educational and clinical practices aimed at reducing anxiety and improving patient care outcomes.
Recommendations for future research and clinical practice
Although this study provided valuable information, further research is needed to explore the long-term effects of preprocedural anxiety reduction on recovery and overall health outcomes. Additionally, developing standardized educational interventions tailored to individual patient needs could further improve anxiety management. Clinical guidelines should incorporate these findings to enhance preprocedural patient care and address the psychological aspects of undergoing CAG.
Conclusion
Based on the results, it is evident that the site of angiography (femoral vs. radial) significantly impacts perceived stress levels, with patients undergoing angiography through the femoral route experiencing higher levels of anxiety. Moreover, the timing and source of information provided to patients play a critical role in alleviating anxiety, with patients who were informed earlier and by healthcare professionals demonstrating lower anxiety scores.
The findings also underscore the importance of providing timely and accurate information to patients regarding their procedure as well as addressing factors such as smoking and alcohol use that may contribute to elevated anxiety levels. This study’s results provide valuable insights into patient care and highlight areas for further research, particularly in refining preprocedural education strategies and investigating the long-term effects of anxiety reduction on postprocedural outcomes.
Footnotes
Acknowledgements
We extend our sincere gratitude to all the patients who participated in this study.
Author contributions
Conception: AK and HCA
Design: AK and HCA
Supervision: HCA
Resource: AK and HCA
Materials: AK and HCA
Data collection and/or processing: AK and HCA
Analysis and/or interpretation: AK and HCA
Literature review: AK and HCA
Writing: AK and HCA
Critical review: HCA
Data availability statement
All data generated or analyzed during this study are included in this published article. Further inquiries may be directed to the corresponding author.
Declaration of conflicting interest
The authors declare that there are no conflicts of interest.
Funding
None.