
Abstract
Niemeier type II gallbladder perforation (GBP) is caused by inflammation and necrosis of the gallbladder wall followed by bile spilling into the abdominal cavity after perforation. The gallbladder then becomes adhered to the surrounding inflammatory tissue to form a purulent envelope, which communicates with the gallbladder. At present, the clinical characteristics and treatment of type II GBP are not well understood and management of GBP remains controversial. Type II GBP with gastric outlet obstruction is rare and prone to misdiagnosis and delayed treatment. Recent systematic reviews report that percutaneous drainage does not influence outcomes. In this current case, due to the high risk of bleeding and accidental injury, as well as a lack of access to safely visualize the Calot’s triangle, the patient could not undergo laparoscopic cholecystectomy, which would have been the ideal option. This current case report presents the use of percutaneous laparoscopic drainage combined with percutaneous transhepatic gallbladder drainage in a patient with type II GBP associated with gastric outlet obstruction. A review of the relevant literature has been provided in addition to a summary of the clinical manifestations and treatments for type II GBP.
Introduction
Gallbladder perforation (GBP) is a rare complication of acute cholecystitis. It often occurs because acute cholecystitis is not treated in a timely manner. Timely diagnosis and treatment can significantly lower the mortality associated with GBP. It may also be caused by trauma and tumours. GBP is classified into three types: acute, subacute, and chronic; and these three types are reflected in the Niemeier classification system. 1 Type III perforations are of acute onset and are often accompanied by acute peritonitis that requires emergency surgery. Type I perforations have a relatively longer course and are associated with fistula formation, which allows for sufficient time for treatment planning. Notably, inappropriate management of type III perforations without surgery may lead to the development of type II perforations. The condition may be temporarily controlled because the perforation site is wrapped by omentum. However, at present, the early diagnosis of type II GBP is difficult; and the timing and manner of surgical treatment for type II GBP remains controversial. This case report describes the diagnosis and treatment of an unusual case of type II GBP and discusses the evidence from previous studies.
Case report
A female patient in her late 50s with upper abdominal pain and abdominal distension for 7 days was referred to the Department of Hepatobiliary Surgery, Xiaolan People’s Hospital of Zhongshan (The Fifth People’s Hospital of Zhongshan), Zhongshan, Guangdong Province, China. She was diagnosed with unexplained stomach ache, hypertension and type 2 diabetes mellitus. Her body mass index was approximately 22 kg/m2. She had received irregular treatment for hypertension and type 2 diabetes for several years. There was no history of surgery, allergies or relevant genetic abnormalities. She had been admitted to another hospital 1 week previously for upper abdominal pain, sudden chills and high fever. Despite receiving antibiotics and intravenous fluids in that hospital, she had persistent abdominal pain and gradually increasing abdominal distension. Upon arrival at our hospital, a physical examination revealed mild abdominal tenderness and a bulge in the upper abdomen with a suspected mass. An abdominal contrast-enhanced computed tomography (CT) scan following admission showed pericholecystic encapsulated effusion (Figures 1a and 1b). Ultrasonography showed gallbladder distension and pericholecystic liquid. Liver function testing showed normal levels of total and direct bilirubin with no evidence of liver dysfunction (Table 1). The gallbladder was not clearly visualized; however, imaging showed no evidence of gallstones. The testing of tumour marks indicated the following: CA-199, 29.77 U/ml; CEA, 3.85 ng/ml. A tumour could not be excluded. Despite receiving antibiotics following admission, she continued to experience slight worsening of distension and poor appetite, which demonstrated that the conservative treatment had failed. Repeat contrast-enhanced CT 8 days after transfer demonstrated an increase in the encapsulated pericholecystic effusion volume (Figures 1c and 1d), so laparoscopic exploration was considered. Due to the high risk of bleeding and accidental injury, as well as a lack of access to safely visualize the Calot’s triangle, the patient could not undergo laparoscopic cholecystectomy. Percutaneous laparoscopic drainage was performed 11 days after transfer following discussion with the patient and her family and after obtaining written informed consent. During the operation, a large pericholecystic abscess compressing the gastric outlet was observed in the Calot’s triangle (Figure 1e). Free bile was removed from the abdominal cavity by suction and an indwelling T-tube was placed in the abscess. The abdominal pain and distension improved significantly on the first day after surgery and the patient was allowed liquid food. However, she complained of abdominal distension and discomfort on the third postoperative day and had anorexia and vomiting after eating. The sense of fullness after meals had been significantly aggravated and there was also a significant reduction in the T-tube drainage volume. Repeat CT revealed a recurrent pericholecystic abscess (Figure 1f) and gastric outlet obstruction. The T-tube was therefore removed. Ultrasound-guided peritoneal puncture was performed and an indwelling drainage tube was placed in the abscess. The distension improved and the patient gradually reverted to a normal diet. She was then discharged from hospital with the tube in place. Except for local mild tenderness, she had no positive signs such as fever, chill or peritoneal irritation during her hospitalization. Her ECOG score was 1. Culture of the drainage fluid showed no bacteria growth.
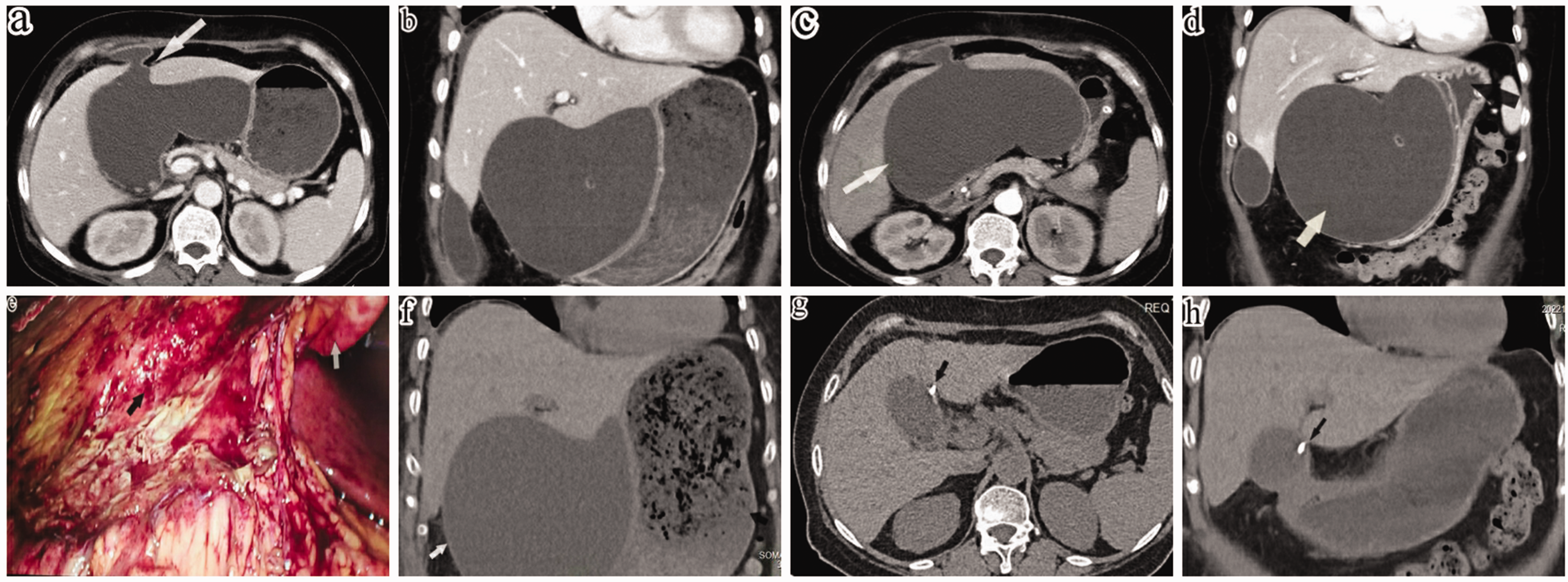
Representative images of a female patient who presented with upper abdominal pain and abdominal distension for 7 days: (a, b) contrast-enhanced computed tomography (CT) images showing pericholecystic encapsulated effusion and the ‘barrier lake’ sign (white arrow); (c, d) CT images showing increased pericholecystic encapsulated effusion (white arrow) and gastric outlet compression (black arrow); (e) pericholecystic abscess observed intraoperatively (the black arrow shows the abscess and the white arrow shows the ligamentum teres hepatis); (f) recurrence of the pericholecystic abscess (white arrow) resulted in gastric outlet obstruction and retention of gastric contents (black arrow) on the fourth day after surgery and (g, h) CT performed after discharge showing normal gallbladder outline and indwelling drainage tube (black arrow). a, c, g: axial image; b, d, h: coronal image. The colour version of this figure is available at: http://imr.sagepub.com.
Clinical data and symptoms during hospitalization of a female patient who presented with upper abdominal pain and abdominal distension for 7 days.

ALT, alanine transaminase; AST, aspartate transaminase; WBC, white blood cells; TLC, total lymphocyte count; TBIL, total bilirubin; DBIL, direct bilirubin; IL-6, interleukin-6; PCT, procalcitonin.
A follow-up CT scan performed 2 weeks after hospital discharge showed that the pericholecystic abscess had disappeared (Figures 1g and 1h), so the drainage tube was removed. The patient reported no discomfort at her 3-month follow-up appointment.
The reporting of the study conforms to CARE guidelines. 2 The details have been de-identified so that the identity of the patient may not be ascertained in any way. The images and data in the study have obtained with the written consent of the patient and her family. The patient and her family agreed and approved of the treatment offered. There were no treatment-related adverse reactions and discomfort during treatment. The publication of the case report was approved by the Medical Ethics Committee of the Xiaolan People’s Hospital of Zhongshan (The Fifth People’s Hospital of Zhongshan) (no. ZSXL-LL2023-001).
Discussion
Type II GBPs are the most common type of GBP. For example, the incidence and mortality of type II GBP from acute and chronic cholecystitis is approximately 1.6% and 4.0%, respectively. 3 The incidence of type II GBP has shown a downward trend in recent years; this may be partly attributed to the revision of indications for cholecystectomy in the Tokyo guidelines, 4 which has led to more aggressive treatment of certain patients with acute cholecystitis. Risk factors for GBP include cholelithiasis, obesity, being elderly, malignancy and immunosuppressive status. 5 Gallstones impacted in the neck of the gallbladder can cause inflammation, ischaemia and necrosis of the gallbladder wall. 6 In this current patient, no stones were observed in her biliary tract or abdominal cavity after abdominal examination, so she was considered to have acalculous GBP. The possible mechanisms of acalculous GBP are as follows: (i) under the condition of gallbladder inflammation, increased intraluminal pressure combined with the external pressure produced by the pericholecystic encapsulated effusion, jointly acts on the gallbladder blood vessels, resulting in wall ischaemia; (ii) and poorly controlled type 2 diabetes mellitus and hypertension could lead to hyaline degeneration, a thickened lumen and stenosis, and thrombosis in the blood vessels of the gallbladder. To the best of our knowledge, this is the first single report of type II GBP with gastric outlet obstruction.
The preoperative diagnosis of type II perforations is difficult. Most cases are diagnosed intraoperatively. In previous studies, the clinical manifestations mainly included right upper quadrant pain, jaundice, nausea, vomiting, leucocytosis, pericholecystic effusion and peritoneal abscess on imaging, and other symptoms similar to those of acute cholecystitis.3,7 Uncommon manifestations included right lower abdominal pain, high fever, abdominal discomfort, anorexia, normal white blood cell counts and diarrhoea.6,8,9 Type II GBP may be misdiagnosed as acute appendicitis or gastrointestinal perforation; 8 and few patients present with septic shock as the first symptom. A previous study suggested that high fever, right upper quadrant pain and leucocytosis were not diagnostic of GBP, as high fever and leucocytosis only occur in a subset of patients. 10 Notably, this current patient had three synchronous clinical manifestations, but only in the early stages. To some extent, the typical clinical manifestations of patients at the onset of this disease were not observed in the current patient. Distension and vague pain in the upper abdomen were the only symptoms that this patient had after hospital transfer. In addition, the current patient presented with rare symptoms of gastric outlet obstruction. These symptoms also led to the delay in the diagnosis of GBP. After admission, the patient only demonstrated leucocytosis and vague pain in the upper abdomen, which might have been attributed to a large number of inflammatory factors in the abdominal cavity. The maximum absorptive capacity of the peritoneum might have been overwhelmed in the early stage of GBP and pericholecystic encapsulation had developed later in the course of the disease. This limited the spread of pyrogens in the abdominal cavity and maintained a balance between the pro-inflammatory and anti-inflammatory factors in the blood.
Owing to the limited number of cases and heterogeneity of clinical manifestations, there is currently no consensus or guidelines on the treatment of type II GBP. Surgical treatment for such cases may be categorized as radical and bridging operations. The former includes cholecystectomy, whether open or laparoscopic, and the latter includes various drainage procedures. Cholecystostomy, percutaneous gallbladder drainage11,12 and radiological drainage 13 are indicated for patients with severe sepsis, advanced age and those who cannot tolerate general anaesthesia. When anatomical and percutaneous hepatic puncture drainage are contraindications, endoscopic ultrasound-guided gallbladder drainage (EUS-GBD) with stenting drainage are also feasible. EUS-GBD has advantages for patients with ascites, shorter life expectancy and poor radiological windows, but there are risks of gastrointestinal bleeding, perforation and bile leakage. 14 Studies have reported that EUS-GBD and percutaneous drainage can provide a comparable effect for patients with acute cholecystitis and surgical contraindications.14,15 Subtotal cholecystectomy represents a crucial rescue operation in cases where cholecystectomy is difficult; it offers similar safety to cholecystectomy and prevents bile duct injury.11,16,17 It may therefore offer an alternative to emergency cholecystectomy in cases of type II GBP.
Cholecystectomy, whether open or laparoscopic, appears to be the best treatment for type II GBP based on the critical view of safety for the Calot’s triangle. The paradox lies in the fact that the condition is often not diagnosed early when it is clinically suitable for surgery and cholecystectomy is often not immediately suitable on obtaining a clear diagnosis. In the present case, percutaneous laparoscopic drainage was performed up to 3 weeks after the onset of the condition and the Calot’s triangle could not be visualized at the time. Most guidelines currently recommend minimally invasive surgery owing to recent developments in minimally invasive techniques and equipment. A previous single-centre study found that laparoscopic cholecystectomy can shorten the length of hospital stay in patients with type II GBP. 17 Reports suggest no significant differences in postoperative complications between open and laparoscopic drainage and early and delayed surgery for type II GBP. 18 The poor drainage after percutaneous laparoscopic drainage in the current case may have been related to the position of the T-tube, T-tube displacement and thicker bile. Subsequent abdominal catheterization improved the patient’s condition and she was discharged from hospital.
In the current case, the pericholecystic effusion associated with gastric outlet obstruction would not provide sufficient space for EUS-GBD. As our centre has insufficient experience in EUS-GBD, this method was not undertaken in the current case. It was not possible to make an early and timely diagnosis of the current patient prior to her surgery. Her diagnosis only became clear during the operation, which might have been related to the atypical clinical manifestations of type II GBP. Therefore, it was also not possible to perform an ultrasound-guided pericholecystic abscess puncture before surgery.
In conclusion, type II GBP is mostly treated based on evidence from case reports because high-level clinical evidence is lacking. In our opinion, percutaneous cholangial drainage is a safe option for patients with type II GBP and severe symptoms of gastrointestinal compression when cholecystectomy is not possible. The diagnosis and treatment of type II GBP needs to be individualized.
Supplemental Material
sj-pdf-1-imr-10.1177_03000605241257452 - Supplemental material for Unusual case of Niemeier type II gallbladder perforation: case report and literature review
Supplemental material, sj-pdf-1-imr-10.1177_03000605241257452 for Unusual case of Niemeier type II gallbladder perforation: case report and literature review by Jiang Liu, Linquan Song, Kailin Guan, Xiangwen Zhao and Zhihong Liang in Journal of International Medical Research
Footnotes
Acknowledgements
We sincerely would like to thank our nursing team for the quality of the patient care and the patient and her family for providing the data presented in this case report.
Author contributions
Jiang Liu and Zhihong Liang were responsible for manuscript writing. Xiangwen Zhao provided suggestions for revision of the manuscript. Kailin Guan and Linquan Song assisted in the treatment of the patient. All authors have read and approved the article content.
Declaration of conflicting interest
The authors declare that there are no conflicts of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.