
Abstract
Objective
Inflammation has a crucial role in several metabolic diseases, such as obesity. The author aimed to investigate the relationship between the system inflammation response index (SIRI) and android fat composition and distribution.
Methods
Data for individuals aged 8–59 years, SIRI, android percent fat, and android-to-gynoid ratio from the 2017 to 2018 National Health and Nutrition Examination Survey were used. Weighted multiple linear regression and smooth curve fitting were used to test for linear and nonlinear associations. Additional subgroup analyses were performed. Threshold effect analysis was performed using a two-linear regression model.
Results
Multiple linear regression showed a positive correlation between SIRI and android percent fat (β 0.92, 95% confidence interval [CI] 0.25–1.59) and between SIRI and the android-to-gynoid ratio (β 0.01, 95% CI 0.00–0.03) in 3783 Americans aged 8–59 years. The results showed that the effect of factors, other than smoking status, on the relationship between SIRI and android percent fat and android-to-gynoid ratio was not significant. There was a nonlinear relationship between SIRI and both android percent fat and android-to-gynoid ratio.
Conclusions
Elevated SIRI levels were associated with an increased android percent fat and android-to-gynoid ratio. Larger prospective studies are needed to validate the findings.
Keywords
Introduction
Obesity is associated with a variety of comorbidities and has become a global health problem. 1 Obesity can be categorized into central and peripheral obesity, depending on the site of fat deposition. The classic android body shape is highly associated with metabolic disorders and is also an important cardiovascular risk factor. 2 Dual-energy X-ray absorptiometry (DXA) is widely used for body composition analysis owing to its high accuracy and non-invasiveness. 3 DXA is used to measure android percent fat and the android-to-gynoid ratio to assess the android regional fat percentage and fat distribution, which reflects abdominal obesity.
The systemic inflammatory response index (SIRI) is a novel composite index used to reflect systemic inflammation and immune response. SIRI has been used in past studies to predict and assess the prognosis of diseases such as pneumonia, rheumatoid arthritis, and acute pancreatitis.4–6 SIRI has also been applied to determine the incidence of cardiovascular disease and has a high predictive value for cardiovascular disease.7–9 Inflammation is directly associated with insulin resistance and chronic metabolic disorders as well as increased cardiovascular risk.10–12 The adverse combined and superimposed effects of different inflammatory mediators and cytokines on metabolic homeostasis is a critical but difficult issue to address. Obesity is closely related to the inflammatory effects of adipocytes. However, the relationship between the body's inflammation levels and fat-deposition tendency is currently unknown owing to the limited number of studies. It is particularly important to understand whether and how the android percent fat and android-to-gynoid ratio are affected.
The National Health and Nutrition Examination Survey (NHANES) database is a nationally representative cohort comprising diverse races and ethnicities. 13 In this study, the NHANES database was used to explore the relationship between SIRI and the android percent fat and android-to-gynoid ratio.
Methods
Study population
The NHANES is a nationally representative survey of the United States population designed to assess the health and nutritional status of the general population in that country. 14 In this study, the NHANES dataset for the United States from 2017 to 2018 and the SIRI composite index were used. Calculation of the SIRI requires use of three indices from a complete blood test: neutrophil count, monocyte count, and lymphocyte count.
The study protocol was reviewed and approved by the Research Ethics Review Board of the National Research Ethics Committee: Continuation of Protocol #2011-17 (effective through October 26, 2017) and Protocol #2018-01 (effective beginning October 26, 2017). All patients/participants provided their written informed consent to participate in this study.
Study variables
The dependent variable in this study was the SIRI, with the android percent fat and android-to-gynoid ratio being the independent variables. Blood cell data were measured using a Beckman Coulter DxH 800 (Beckman Coulter, Inc., Brea, CA, USA) in an NHANES mobile examination center. The android area comprises the lower part of the trunk above the pelvic line and 20% of the length between this line and the neck cut line. The gynoid area is defined as twice the height of the android region below the pelvic line. 15 The android percent fat and android-to-gynoid ratio were measured using DXA. The android percent fat was calculated as the android fat mass divided by the android total mass. Hologic APEX software (Hologic, Inc., Marlborough, MA, USA) was used to calculate the android-to-gynoid ratio measured using DXA. The SIRI is calculated as the neutrophil count × monocyte count/lymphocyte count.
Statistical analysis
R version 4.1.3 (www.r-project.org) and EmpowerStats version 2.0 (X&Y Solutions, Inc., Boston, MA, USA) were used for statistical calculations in this study. Baseline tables for the study population were stratified by SIRI quartiles. Continuous variables are described using mean ± standard deviation (SD) and were analyzed using weighted linear regression models. Multiple linear regression analysis was used to calculate β values and 95% confidence intervals (CIs). Multivariate tests were constructed using three models. Model 1 was unadjusted. Model 2 adjusted for the variables of sex, race and ethnicity, and age. Model 3 was adjusted for all covariates. Smoothed curves were fitted after adjusting for variables. Threshold effects analysis was used to explore the association and inflection points between the SIRI and android percent fat and android-to-gynoid ratio. Subgroup analyses were additionally performed.
Results
Baseline characteristics
From the NHANES dataset for the United States from 2017–2018, 1731 participants with incomplete blood data were excluded. Another 3728 participants with missing android and/or gynoid data were also excluded. Body mass index (BMI) is a basic indicator related to obesity and body composition, and is an important covariate. An additional 12 participants with missing BMI data were also excluded. The study ultimately included 3783 participants. Figure 1 illustrates the participant selection.
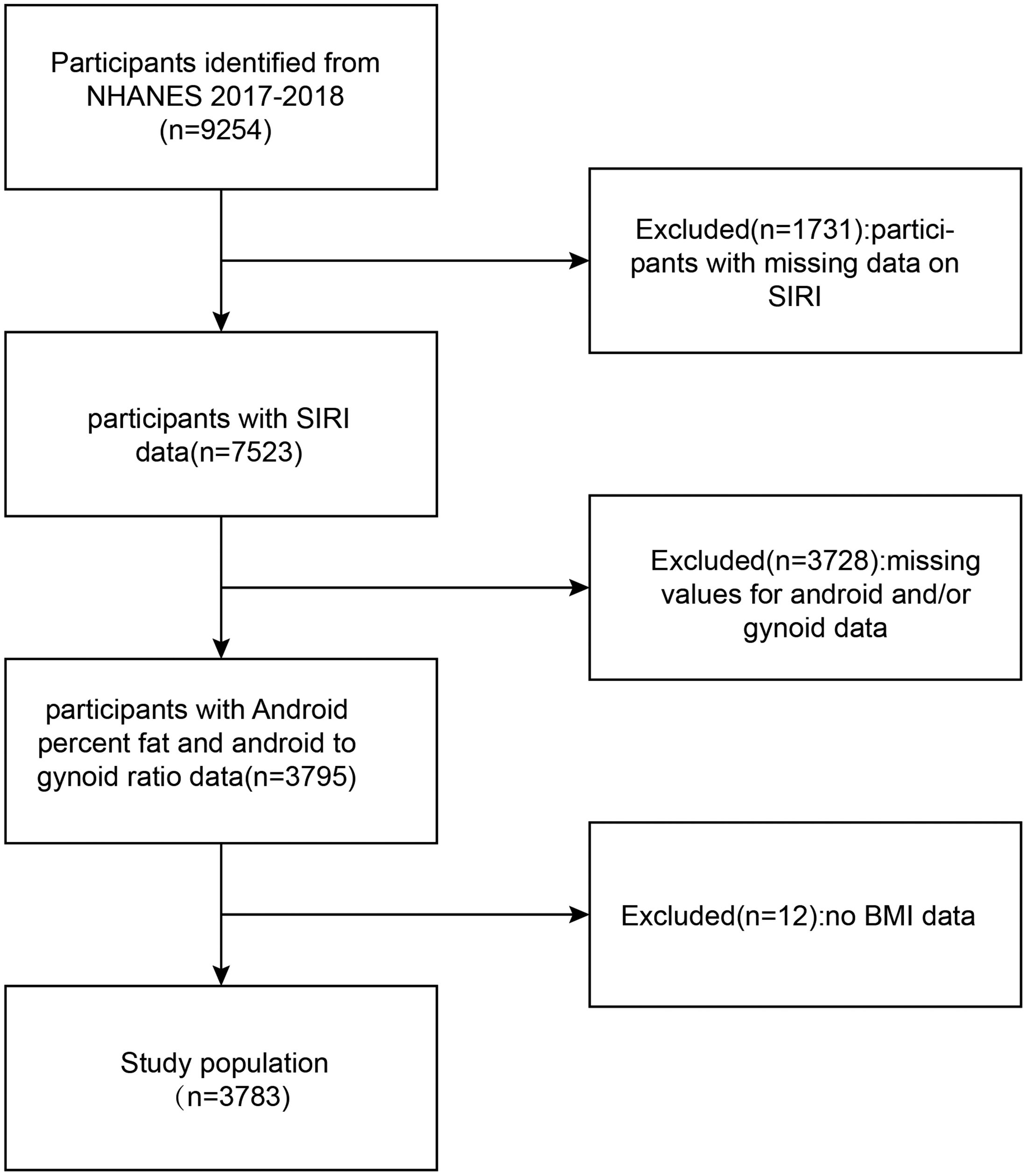
Flowchart of participant selection. NHANES, National Health and Nutrition Examination Survey; SIRI, system inflammation response index; BMI, body mass index.
Among the 3783 adults included in this study, the mean age was 33.82 ± 15.11 years. Of the total participants, 52.25% were men and 47.75% were women; 11.72% were Mexican American, 8.19% were other Hispanic, 56.11% were non-Hispanic White, 11.92% were non-Hispanic Black, and 12.06% were other race and ethnicity. The mean (SD) SIRI was 1.15 ± 0.84 (1000 cells/µL). The android percent fat and android-to-gynoid ratio were 33.74 ± 9.60% and 0.97 ± 0.20, respectively.
The SIRI was divided into four groups, according to quartiles (Table 1). Participants with high SIRI levels were likely to be non-Hispanic White, smokers, and have lower household income and education levels. High SIRI levels were significantly associated with high BMI, waist circumference (WC), hip circumference, total cholesterol, triglyceride (P = 0.0026), monocyte count, neutrophil count, android percent fat, and the android-to-gynoid ratio (all P < 0.0001, except triglyceride). High SIRI levels were also significantly associated with low levels of direct high-density lipoprotein (HDL) and low lymphocyte count. High SIRI levels were more common in older individuals, and those with high SIRI levels were more likely to have comorbid diabetes (all P < 0.0001).
Basic characteristics of participants, by systemic inflammation response index quartiles.

Mean ± standard deviation for continuous variables: P value was calculated using a weight linear regression model.
% for categorical variables: P value was calculated using the weighted chi-square test.
SIRI, system inflammation response index; HDL, high-density lipoprotein; LDL, low-density lipoprotein.
Table 2 shows the results of multiple regression analysis. SIRI was significantly associated with android percent fat in the unadjusted model (β 1.58, 95% CI 1.22–1.94). After adjusting for sex, age, and race and ethnicity, the association remained significant in Model 2 (β 1.39, 95% CI 1.06–1.72). After adjusting for all covariates, the relationship between SIRI and the android percent fat remained significant (β 0.92, 95% CI 0.25–1.59, P < 0.0001).
Relationship between systemic inflammatory response index (SIRI) and android percent fat.

Model 1: no covariates were adjusted. Model 2: age, sex, race and ethnicity were adjusted. Model 3: age, sex, race and ethnicity, education level, family income-to-poverty ratio, smoking status, alcohol consumption, direct HDL, LDL, total cholesterol, triglyceride, and glucose were adjusted.
In the subgroup analysis stratified by sex and smoking status, the model was not adjusted for sex and smoking status, respectively.
CI, confidence interval; HDL, high-density lipoprotein; LDL, low-density lipoprotein.
Subgroup analyses were performed to assess the stability of the relationship between SIRI and android percent fat stratified by different factors. The results showed that factors other than smoking status did not have a significant effect on the relationship between SIRI and android percent fat. The difference in the association between SIRI and android percent fat with different sex strata was not statistically significant in model 3, adjusted for all variables. The presence or absence of comorbid diabetes also had no effect on the association between SIRI and android percent fat.
As shown in Figure 2, adjustments were made for all significant predictor variables, including age, sex, race and ethnicity, education level, family income-to-poverty ratio, smoking status, alcohol consumption, direct HDL, low-density lipoprotein (LDL), total cholesterol, triglyceride, and glucose. Smooth curve fitting was applied to describe the nonlinear relationship between SIRI and android percent fat.

Association between system inflammation response index (SIRI) and android percent fat. Solid red line represents the smooth curve fit between variables. Blue bands represent the 95% confidence intervals for the fit.
Using a two-linear regression model, an inflection point (K) of 1.92 was identified, describing the relationship between SIRI and the android percent fat (Table 3).
Threshold effect analysis of SIRI on android percent fat using a two-piecewise linear regression model.
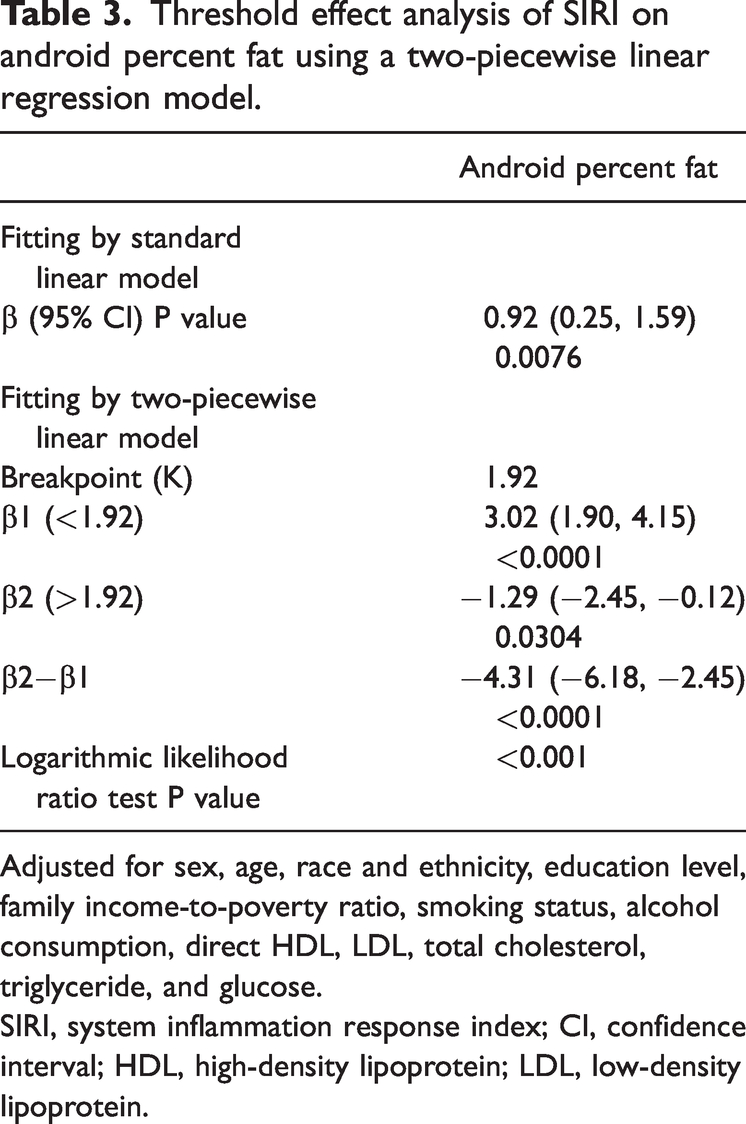
Adjusted for sex, age, race and ethnicity, education level, family income-to-poverty ratio, smoking status, alcohol consumption, direct HDL, LDL, total cholesterol, triglyceride, and glucose.
SIRI, system inflammation response index; CI, confidence interval; HDL, high-density lipoprotein; LDL, low-density lipoprotein.
As seen in Table 4, SIRI and the android-to-gynoid ratio were significantly correlated in the unadjusted model (β 0.03, 95% CI 0.02–0.04) and the partially adjusted model (β 0.02, 95% CI 0.01–0.02). After adjusting for all covariates, the relationship between SIRI and the android-to-gynoid ratio remained significant in model 3 (β 0.01, 95% CI 0.00–0.03, P < 0.0001).
Relationship between SIRI and android-to-gynoid ratio.

Model 1: no covariates were adjusted. Model 2: age, sex, race and ethnicity were adjusted. Model 3: age, sex, race and ethnicity, education level, family income-to-poverty ratio, smoking status, alcohol consumption, direct HDL, LDL, total cholesterol, triglyceride, and glucose were adjusted.
In subgroup analysis stratified by sex and smoking status, the model was not adjusted for sex and smoking status, respectively.
SIRI, system inflammation response index; CI, confidence interval; HDL, high-density lipoprotein; LDL, low-density lipoprotein.
We analyzed the association between SIRI and the android-to-gynoid ratio in subgroups stratified by sex, smoking status, and comorbid diabetes. Smoking status was significant in the association between SIRI and the android-to-gynoid ratio (P for interaction <0.05). In model 3, adjusted for all covariates, the difference in the association between SIRI and the android-to-gynoid ratio was not significant across sex strata. The presence or absence of comorbid diabetes also had no effect on the association.
As shown in Figure 3, adjustments were made for age, sex, race and ethnicity, education level, family income-to-poverty ratio, smoking status, alcohol consumption, direct HDL, LDL, total cholesterol, triglyceride, and glucose. Smooth curve fitting was applied to describe the nonlinear relationship between SIRI and the android-to-gynoid ratio.

Association between system inflammation response index (SIRI) and android-to-gynoid ratio. Solid red line represents the smooth curve fit between variables. Blue bands represent the 95% confidence intervals for the fit.
Using a two-linear regression model, an inflection point (K) of 1.59 was found, describing the relationship between SIRI and the android-to-gynoid ratio (Table 5).
Threshold effect analysis of SIRI on android-to-gynoid ratio using a two-piecewise linear regression model.

Adjusted for sex, age, race and ethnicity, education level, family income-to-poverty ratio, smoking status, alcohol consumption, direct HDL, LDL, total cholesterol, triglyceride, and glucose.
SIRI, system inflammation response index; CI, confidence interval; HDL, high-density lipoprotein; LDL, low-density lipoprotein.
Discussion
In the present study, a positive association was found between SIRI and both the android percent fat and android-to-gynoid ratio. Subgroup analyses revealed that this positive association remained consistent across sex and smoking status subgroups, except for the diabetes status subgroup. Notably, there was an inverted U-shaped relationship between SIRI and both the android percent fat and android-to-gynoid ratio, with inflection points of 1.92 (1000 cells/µL) and 1.59 (1000 cells/µL). This showed that SIRI was an independent risk factor for android fat percent when the SIRI values was below 1.92 (1000 cells/µL). SIRI was an independent risk factor for the android-to-gynoid ratio when the SIRI value was below 1.59 (1000 cells/µL).
To the author’s best knowledge, this is the first cross-sectional investigation to explore the relationship between SIRI and the android percent fat and android-to-gynoid ratio. Many studies have demonstrated that inflammation is associated with obesity. Adipose tissue inflammation is a combination of systemic inflammation and metabolic disorder, which is associated with increased systemic inflammation and decreased insulin sensitivity. 16 Abdominal (central) obesity is an important component of metabolic syndrome (MetS). Wang et al. 12 showed that SIRI is significantly associated with MetS and its components, with a higher SIRI being associated with a higher risk of metabolic disorders. Nicoară et al. 17 found that children with MetS have higher levels of inflammatory status (systemic immune-inflammation index and/or SIRI). Elevated inflammatory indices are significantly correlated with the presence and severity of MetS, which is consistent with the findings of the present study. Therefore, how best to control inflammation may be a new direction in obesity control and the treatment of obesity-related metabolic diseases, such as insulin resistance and type 2 diabetes.
Conclusions differ regarding the relationship between non-obesity-related inflammatory diseases and fat distribution in the android/gynoid region. Crohn's disease is a representative chronic inflammatory disease. In contrast to the conclusions of most studies,18,19 Dowling et al. 20 found that adult patients with Crohn's disease exhibited less fat in the android region and more fat in the gynoid region compared with the healthy population, independent of changes in disease. The mesenteric adipose tissue encapsulating the diseased intestine, also known as “creeping fat,” is a protective barrier against inflammatory mediators and intestinal bacterial translocation, 21 and its presence is limited to the android region. Greater inflammation in Crohn's disease before effective treatment is associated with less mesenteric fat in the android region. In patients with Crohn's disease, the relative paucity of fat in the android region co-occurs with creeping fat, weakening of the intestinal barrier, translocation of numerous pathogenic bacteria, and initiation of an immune response by the mesenteric lymph nodes, which causes intestinal inflammation. Surgical diversion of feces can slow the systemic inflammatory and fibrotic processes. 22 Postoperative whole blood tests show a decrease in neutrophils and monocytes and an increase in lymphocytes, confirming an improvement in inflammatory status, in comparison with the preoperative period; this is in line with the assessment of inflammation levels according to SIRI. In previous studies, SIRI has been used as an indicator to assess the progression and prognosis of postoperative oncology,23,24 cardiovascular disease,7,9,25,26 and rheumatic immune diseases. 5 Okosun et al. 27 showed that the android–gynoid fat percentage was more strongly associated with cardiometabolic disorders than the android fat percentage, gynoid fat percentage, or BMI. A mix of android and gynoid fat is associated with much greater cardiometabolic risk than android or gynoid fat alone.
Neutrophil counts and ratios are traditional indicators of the inflammatory state of the immune system. Circulating monocytes and lymphocytes can be involved in immune defense, regulation, and damage repair processes. Therefore, SIRI calculated from peripheral neutrophil, monocyte, and lymphocyte counts may be a powerful and reliable indicator of inflammatory status that can effectively and thoroughly reflect the inflammatory state of the body and the state of the immune system as a composite inflammatory index. The use of DXA in body composition analysis is important for the assessment of follow-up in patients with obesity. The android-to-gynoid ratio is significantly associated with obesity-related diseases such as non-alcoholic fatty liver disease, insulin resistance, and postmenopausal osteoporosis.15,28,29 WC has been proposed as a surrogate for indirectly assessing visceral fat gain and as an indicator of abdominal obesity in the diagnosis of MetS. 30 However, similar to BMI, WC by itself cannot quantify abdominal fat content and distribution. This study is consistent with previous research findings that higher levels of inflammation are associated with greater levels of abdominal fat accumulation.
Metabolic regulation and immune response are basic requirements for survival, and the proper function of each is dependent on the other. 11 The mechanisms behind the link between inflammation and central fat accumulation are unclear. The onset and progression of obesity and related metabolic diseases depend on low-grade chronic systemic inflammation induced by various types of cellular stress responses and immune cell activation in adipose tissue. 31 The low-grade inflammatory state is often associated with damage to peripheral tissues and disturbances in insulin metabolism. 32 Therefore, investigating the association between the level of body inflammation and central obesity is crucial for reducing central fat accumulation and ameliorating metabolic disturbances.
Adipose tissue not only plays an important role in storing excess nutrients but it also senses nutritional status and regulates energy mobilization. Excess nutrients and a positive energy balance may induce cellular stress in adipose tissue, releasing chemokines, initiating adaptive inflammatory responses, and causing adipocytes to expand to reduce capacity storage. 31 There is evidence that obesity and its comorbidities are associated with chronic inflammation in the body.11,33,34 The results of a study conducted by Łuczyński et al. 35 showed a higher percentage of T helper 17 cells in the peripheral blood of centrally obese children, suggesting that chronic inflammation accompanied by immune disorders may have an important role in the pathogenesis of obesity. However, other studies have not reached the same conclusions, Goswami et al. 36 conducted animal experiments on excessive weight gain in mice lacking interleukin (IL)-17A receptors; their findings suggested that IL-17 inhibits the growth of adipose tissue. In another study, elevated serum levels of IL-17 in obese female patients were not associated with BMI, WC, HOMA index, or leptin levels. 37
The strengths of this study included the large sample size, a representative, multiracial study population, and the use of smooth curve fitting, segmented regression, and log-likelihood ratio tests in determining the existence of a threshold. The advantages of using DXA to measure soft-tissue components allowed for the direct quantification of the regional fat distribution throughout the body. However, despite adjusting for some covariates, other factors may still be influential and the presence of other potential confounders, such as medication use, including glucocorticoids and weight-loss medications, and dietary status, cannot be completely ruled out, which may affect the interpretation of the data. In addition, owing to the cross-sectional nature of this study, a causal relationship could not be confirmed.
Conclusion
The study findings suggested that elevated SIRI levels are associated with increased android percent fat and android-to-gynoid ratio. Larger prospective studies are needed to confirm these findings.
Footnotes
Acknowledgements
The author thanks all the participants in NHANES for their valuable contributions to this study.
Conflict of interest
The author declares that there is no conflict of interest.
Data availability statement
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.