
Abstract
Blood-disseminated Aspergillus spondylitis in immunocompetent individuals is rare. The clinical, imaging, and pathological manifestations of this condition are not specific. Therefore, this disease is prone to misdiagnosis and a missed diagnosis. Systemic antifungal therapy is the main treatment for Aspergillus spondylitis. We report a case of blood-disseminated Aspergillus versicolor spondylitis in a patient with normal immune function. The first antifungal treatment lasted for 4 months, but Aspergillus spondylitis recurred a few months later. A second antifungal treatment course was initiated for at least 1 year, and follow-up has been ongoing. Currently, there has been no recurrence.
Introduction
Mycotic spondylitis is a rare, clinical, spinal infectious disease, 1 and is more common in immunosuppressed patients than in immunocompetent patients. Spinal involvement, whether by direct or haematogenous dissemination, is usually secondary to fungal infection in the lungs, gastrointestinal tract, or brain. The misdiagnosis rate of this condition is relatively high because of its low incidence and thus there is an insufficient understanding of its clinical manifestations and imaging features. We report a case of blood-disseminated Aspergillus versicolor spondylitis in an immunocompetent host.
Case report
Patient and medical history
The patient was a man in his early 60s who had been working in the brewing industry for more than 30 years. He was admitted to our Orthopaedics Department in August 2020 because of 50 days of lower back pain. Initially, he had no pronounced symptoms or restricted mobility and thus did not seek medical attention. A month previously, the pain worsened and became severe, with radiating pain to the right lower limb. The mobility of his lower back was limited and gradually worsened, resulting in an inability to stand. At this point, he visited the hospital for medical treatment.
This study received approval (approval number: L2021-04-049) for publication from the Ethics Committee of Dingli Clinical Institute of Wenzhou Medical University (Wenzhou Central Hospital), and written informed consent was obtained from the patient. The reporting of this study conforms to the CARE guidelines. 2
Physical examination
There were no obvious deformities in the spine. Cervical spinal movement was smooth, and there was no obvious tenderness in the cervical or thoracic intervertebral spaces. The lumbar spine was less mobile but there was no tenderness near the vertebral bodies. The results of a battery of tests were as follows: in the straight leg elevation test, the left side was 70° and the right side was 30°; in the reinforcement test, the left side was negative and the right side was positive; in the “4” sign, the left and right sides were negative; knee reflex, left (++) and right (++); Achilles tendon reflex, left (++) and right (++); and for extensor dorsalis pedis muscle strength, the left was level 5 and the right was level 4, with decreased sensation in front of the calf and dorsalis pedis.
Laboratory tests
No abnormalities were detected in the following tests: routine blood work-up, liver and kidney function, tumour markers, the antinuclear antibody spectrum, and concentrations of immunoglobulin light chain, anti-O antibodies, rheumatoid factor, anti-neutrophil antibody, urine light chain, Aspergillus galactomannose, and Aspergillus antibody immunoglobulin G. M protein was not found, and tests for Cryptococcus capsule antigen in the blood were negative. However, the blood C-reactive protein concentration was 221.6 mg/L (normal range: 0–8 mg/L), the erythrocyte sedimentation rate (ESR) was 102 mm/hour (0–20 mm/hour), and the T cell spot test for tuberculosis infection was positive.
Imaging examinations
Positron emission tomography/computed tomography (PET/CT) findings strongly suggested a haematological tumour (e.g., multiple myeloma) based on the findings in multiple ribs (bilaterally), vertebral bodies, spinal attachments, and multiple foci in the pelvis. Magnetic resonance imaging (MRI) results were consistent with the PET/CT findings (Figure 1). A low signal intensity was obtained in T1-weighted imaging, an equal or slightly higher signal in T2-weighted imaging, and a high signal in a fat suppression sequence with obvious enhancement. In lumbar MRI, abnormal signal shadows were present in multiple thoracic, lumbar, and sacral vertebrae and attachments, suggesting multiple myeloma or a metastatic tumour (Figure 2). Cervical MRI showed degenerative changes in the cervical spine, with mild herniation of the C3/4, C4/5, C5/6, and C6/7 intervertebral discs, with possible yellowing myelination of the cervical and thoracic vertebral bodies. In thoracic CT, the following findings were observed bilaterally: micronodules under the pleura in the upper lobes, together with uneven emphysema in the upper lobes; fibrotic lesions in the lower lobes; and a small amount of pleural effusion accompanied by poor compression and expansion in the lower lobes. Multiple old rib fractures on the left side were also observed.

Positron emission tomography/computed tomography obtained on 31 August 2020 shows a focal increase in glucose metabolism in the spinal appendage.

Thoracic and lumbar spine magnetic resonance imaging obtained on 26 August 2020 shows multiple abnormal signal shadows in the thoracic, lumbar, and sacral vertebral bodies and attachments (arrow).
Diagnosis and treatment
After admission, the patient received a dexamethasone injection for anti-inflammatory and analgesic treatment daily for 1 week. This injection resulted in a slight reduction in his lower back pain, a decrease in his C-reactive protein concentration to 34 mg/L, and a decrease in his erythrocyte sedimentation rate to 51 mm/hour. A pathological examination following thoracic vertebral puncture biopsy showed a thoracic vertebral body lesion, bone marrow haematogenic tissue, interstitial bleeding, and suspected fibrous protein exudation tissue. Acid fast staining was negative and silver amine staining was negative (Figure 3), but the T cell spot test for tuberculosis infection was still positive. A diagnosis of tuberculous spondylitis was considered. The patient was placed on anti-tuberculosis treatment for 1 month, but his back pain did not considerably improve and he continued to take painkillers. Another chest and lumbar spine MRI showed no resolution of the lesions. The patient was re-admitted, and a bone marrow puncture and re-biopsy were recommended but the patient refused. After discussion, a blood sample was sent for metagenomic next-generation sequencing (mNGS) on 12 October 2020. The results strongly suggested the presence of the pathogen A. versicolor, and a diagnosis of A. versicolor spondylitis was considered. We obtained the patient’s consent for treatment. He was treated with voriconazole capsules (200 mg) administered orally every 12 hours. After 2 weeks of treatment, he no longer complained of lower back pain, and a follow-up blood test showed a normal C-reactive protein concentration and erythrocyte sedimentation rate. After 2 months, his chest and lumbar spine MRI were consistent with a disappearance of the lesions (Figure 4). The treatment was terminated after 4 months and the patient was symptom-free, including no lower back pain, during the following 1 year. However, in December 2021, he experienced a recurrence of pain accompanied by limited lower limb mobility. There was no change in MRI imaging findings. Another biopsy was suggested but the patient refused. Recurrence of Aspergillus spondylitis (AS) was suspected, and in June 2022, he was restarted on voriconazole capsule antifungal treatment, which quickly relieved his lower back pain. Antifungal treatment has been discontinued for at least 1 year. MRI follow-up in August 2023 showed further absorption of spinal lesions compared with previous images in June 2022 (Figure 5). The patient is currently in good health.
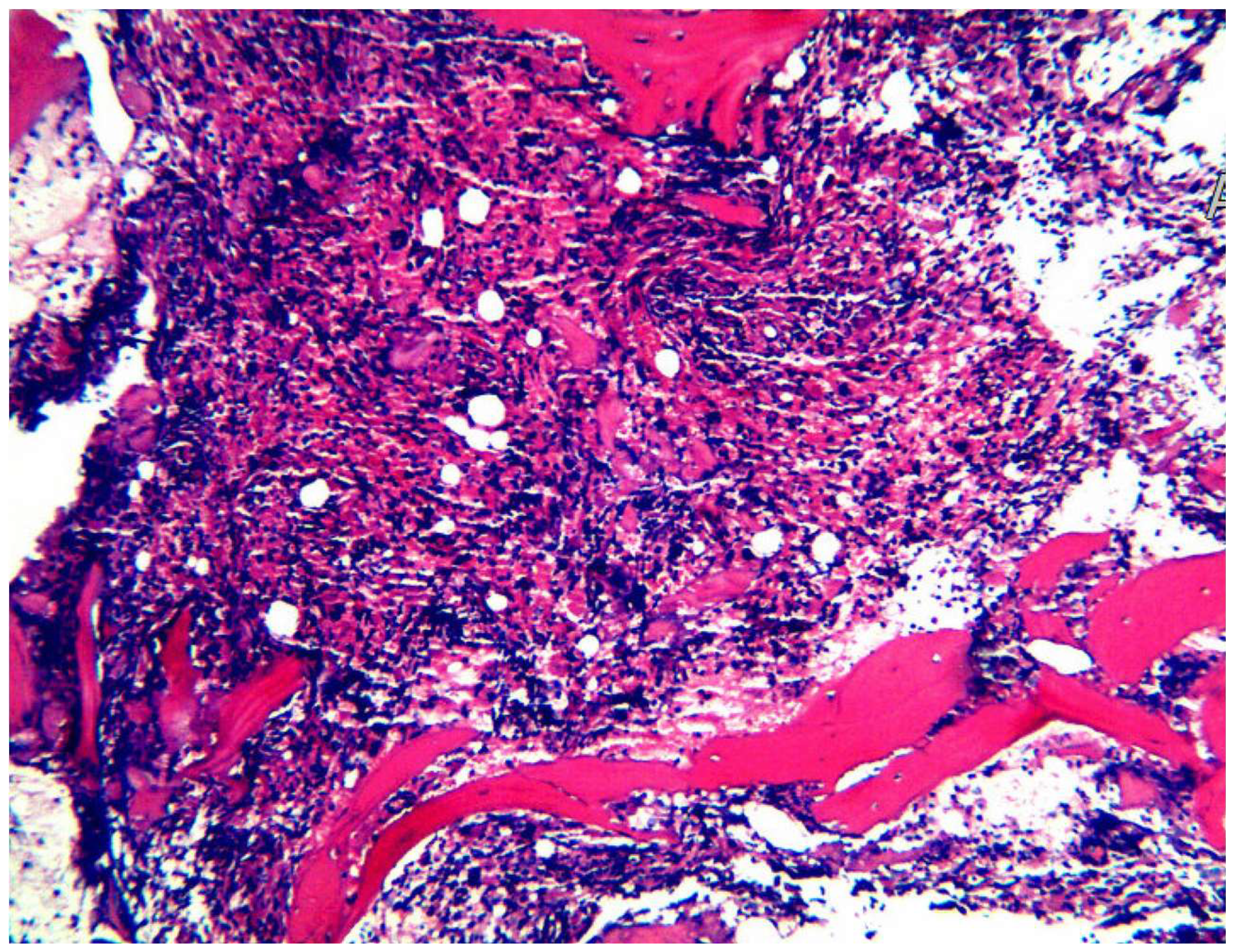
Pathological results of a thoracic vertebral puncture biopsy, including a lesion of the thoracic vertebral body in bone marrow haematopoietic tissue, interstitial haemorrhage, and suspected fibrin exudate. Acid fast staining, periodic acid–Schiff staining, and hexamine silver staining were negative.

Magnetic resonance imaging on 4 December 2020 shows that multiple abnormal signal shadows of the cervical vertebrae (left) are improved (slightly reduced range and degree) compared with previous imaging on 26 August 2020 (right).

Magnetic resonance imaging in August 2023 shows considerable improvement in the resolution of abnormal signal shadows in the thoracic and lumbar vertebrae compared with previous imaging (June 2022, October 2020) (arrow).
Discussion
The majority of patients with AS are immune-deficient or have immune-suppressing conditions (acquired immune deficiency syndrome, organ transplantation, chemotherapy, or immunosuppressive treatment), and this disease is rare in healthy people. 3 A retrospective study of Aspergillus osteomyelitis showed that the vertebrae were the most commonly affected (49%) and 13% of patients had no risk factors. 1 Nicole et al. 4 analysed 44 cases of AS in patients with normal immune function. The average age of the patients was 48.45 years and more men were affected than women. AS-promoting factors were detected in 84% of the patients, including pulmonary aspergillosis, pulmonary tuberculosis, diskectomy, diabetes, chronic obstructive pulmonary disease, and mycotic endocarditis. A. fumigatus (74%) and A. flavus (12%) were the most frequently isolated fungi, but A. versicolor was also identified. Blood-borne spread is the dominant pathway (62%) of AS, but other routes include direct vaccination (related to trauma, spinal surgery, and epidural injection) and continuous spread.4,5
The clinical manifestations of AS are nonspecific but the most common initial symptom is lower back pain. If there is an epidural abscess or granuloma formation, symptoms of spinal cord nerve compression can occur. Some patients with AS experience paraplegia and/or fever.4,6 Our patient’s basic immune function was normal but his long-term employment in the brewing industry may have been a factor in the aetiology of his disease. His main clinical manifestations were basically consistent with those reported in the literature, including lower back pain, numbness in the right lower limb, and decreased muscle strength but not fever. 5 At present, there is no highly sensitive and specific serological test for AS. 4 The diagnosis of AS mainly relies on puncture or pathological examination of surgical specimens, but repeated biopsy or culture may be required for the diagnosis. Consequently, the early clinical diagnosis of AS is difficult. The blood G test, Aspergillus galactomannose test, blood culture, and biopsy pathology were negative in our patient. Consequently, he was misdiagnosed with tuberculous spondylitis and treated accordingly for 1 month. The correct diagnosis was made by mNGS of a blood sample. In 2014, Wilson et al. 7 reported a case of Leptospira, which was detected in cerebrospinal fluid using metagenomic sequencing and subsequently successfully treated. Since this report, mNGS has attracted increasing clinical and research attention and has changed the diagnosis and treatment of infectious diseases. mNGS has a higher sensitivity than traditional culture methods, and is more accurate in the diagnosis of tuberculosis, fungi, viruses, and anaerobic bacteria.8,9 In a clinical study of periprosthetic joint infection, the sensitivity and specificity of mNGS reached 94.8% and 89.2%, respectively, while traditional culture methods had lower sensitivity (58.6%) and higher specificity (94.6%). In addition, the time to perform mNGS is considerably shorter than traditional cultivation methods (average of 1.3 hours compared with 5.2 hours). 10
The imaging manifestations of AS are related to the patient’s immune status and the disease duration.6,11,12 In the early stages, CT shows bone absorption on the surface of the vertebral body, followed by the development of areas of honeycomb or foam-like bone destruction of the vertebral body with marginal bone sclerosis. AS then progresses, particularly in low-density areas, and the intervertebral discs may also be involved. MRI in our patient showed that the lesion was initially limited to the vertebral endplate in the early stages, but then involved the entire vertebral body and its attachments, forming paravertebral and epidural granulomas or abscesses. In the early stages of AS, the intervertebral disc is not affected and the intervertebral space is normal, while in late stages, the disc can collapse or cause intervertebral space stenosis and spinal cord compression. Williams et al. 13 found that a low disc signal and the presence of intervertebral spaces in T2-weighted imaging are important features for distinguishing AS from purulent spondylitis. The radiological characteristics of AS in our patient were not different from those reported in a series of cases of tuberculosis vertebral osteomyelitis. 14 Therefore, the tuberculin skin test, the T cell spot test for tuberculosis infection, and a specimen X-pert examination should also be performed to obtain a correct diagnosis.
A literature review showed that, after surgery and/or antifungal treatment, the treatment success rate of AS was 65.7% to 75%, but a small portion of patients had poor outcomes, with a mortality rate ranging from 16% to 28.8%.1,4,15 In the treatment of Aspergillus, the main antifungal drugs currently used are triazoles, such as voriconazole and itraconazole, and posaconazole is an optional alternative drug. 16 Voriconazole has acceptable safety, extensive systemic antifungal activity, high oral bioavailability, and good bone diffusion. However, for the treatment of invasive aspergillosis, voriconazole is superior to amphotericin B in terms of survival and toxicity. 17 Although experience in the use of voriconazole to treat AS is limited, the current guidelines of the American Society of Infectious Diseases recommend it as a first-line antifungal drug for treating Aspergillus osteomyelitis. The optimal treatment time has not been determined, but at least 6 to 8 weeks is recommended. 18 The average duration of AS antifungal treatment in clinical practice is 6.1 months. 19 The treatment duration of our patient was 4 months, with recurrence after 1 year. He was then treated with voriconazole for another year. Further research is required to determine the optimal course of antifungal treatment, and whether combined antifungal therapy and surgical treatment are superior to antifungal therapy alone. In a retrospective analysis of 44 cases of AS in patients with normal immune function, the cure rate achieved with antifungal drugs without surgery (15/19, 79%) was better than that with surgery (16/25, 64%), but the difference was not statistically significant. 4 The course of treatment in this previous study was 3 weeks to 14 months. In another systematic review, patients with Aspergillus osteomyelitis treated surgically and with antifungal therapy had a lower recurrence rate than those treated with antifungal therapy alone. 20 Surgical indications include abscess formation, vertebral destruction, and neurological deficits. 20
Summary
A. versicolor spondylitis is rare and difficult to diagnose. Antifungal treatment for this condition should be considered to be extended for an appropriate period of 6 months or even 1 year because of the spread of blood through menstruation.
Footnotes
Acknowledgement
We appreciate the patient for consenting to share his case information.
Author contributions
S.X.D. and Z.L. designed and performed research; Q.D.L. and X.J.D. analysed data; and S.X.D. wrote the manuscript. All authors read and approved the final manuscript.
Data availability statement
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.