
Abstract
Objective
To understand primary care physicians’ perspectives on academic detailing from an antimicrobial stewardship team to combat antibiotic overuse for upper respiratory infections and bronchitis in the COVID-19 era, which will help prevent avoidable outpatient visits.
Methods
In this prospective study, 14 female Croatian physicians completed standardized qualitative interviews using a semi-structured guide. The data were analyzed using inductive methodology based on reflexive thematic analysis. We used a theoretically informed approach based on a conceptual framework of healthcare intervention implementability focused on three domains: acceptability, fidelity, and feasibility.
Results
We identified six key themes highlighting barriers to changing prescribing practices, with patient pressure and specialist recommendations having an impact on the effectiveness of academic detailing. Despite challenges, primary care physicians described appreciation of direct interaction with evidence-based practices and reported usefulness, effectiveness, and further need for academic detailing.
Conclusion
This study highlights the complex dynamics involved in implementing healthcare interventions and provides valuable insights for enhancing strategies directed at improving antibiotic prescribing practices. Specifically, our findings emphasize factors influencing behavior changes in physicians’ antibiotic prescribing. The authors advocate for a collaborative approach involving community and hospital-based professionals to provide tailored guidance and address questions, ultimately improving prescribing practices.
Keywords
Introduction
Acute upper respiratory tract infections and acute bronchitis (ARI&AB) are the most common reasons for outpatient physician office visits and inappropriate antibiotic prescribing in adults, which is particularly relevant in the era of COVID-19.1,2 Studies show that more than 90% of antibiotic prescriptions are made in the community setting, with up to 50% of those for ARI&AB being unnecessary.1,3 This contributes to the increase in antimicrobial resistance (AMR), which has led to a 16% rise in annual European AMR deaths from 2016 to 2019.4,5 Additionally, yearly reports from the European Centre for Disease Prevention and Control (ECDC) and World Health Organization (WHO) Regional Office for Europe indicate that resistance to antibiotics is more common in southern and eastern Europe, where antibiotic use per person is greater than that in northern Europe. 6 For instance, the use of antibiotics in Southern European countries is approximately three times higher than that in Scandinavia and the Netherlands. 7
Combating antibiotic-resistant bacteria is crucial, and improving antibiotic prescribing practices in healthcare settings is a key component in this effort. 5 Antimicrobial stewardship programs (ASPs) aim to ensure the judicious use of antimicrobials and improve patient outcomes, reduce the spread of resistance, prevent deaths from resistant infections, and reduce healthcare costs.8,9 Most ASP teams (A-teams) comprise an infectious disease physician, a clinical microbiology physician, and a clinical pharmacist.5,10 Clinician-focused ASPs such as those involving audit feedback with peer comparison, academic detailing (AD), and clinician communication training, have been shown to be effective in reducing unnecessary antibiotic treatment of ARI&ABs. 11 Additionally, these programs promote evidence-based and internationally-standardized optimization of antimicrobial use. 12
AD is an educational outreach method in which peers, colleagues, or opinion leaders including other clinicians and pharmacists, have one-on-one meetings with prescribers, providing them with the latest evidence-based information on commonly used drugs. This helps facilitate changes in antibiotic prescribing practices. 13 AD for acute respiratory tract infections has been successful in improving antibiotic prescribing in Norway, Saudi Arabia, and the United States, leading to increased safety and savings.14–16 For this reason, AD is one of the main antimicrobial stewardship strategies recommended in the international literature for improving prudent antibiotic use. 17 Additionally, studies show that AD is suitable for keeping primary care physicians (PCPs) up-to-date and that PCPs welcome future AD visits.18,19
Currently, there is a scarcity of research on the effectiveness of ASPs in improving prudent antimicrobial use in Southeast Europe, including during the COVID-19 pandemic. 20 Although clinician-focused ASPs have been successful globally, it is unknown whether AD programs would be accepted and useful in Southeast European countries such as Croatia. Furthermore, which ASP interventions are appropriate and feasible in this area remains unclear, as do the potential barriers to AD implementation.
Given the increasing concerns about unnecessary patient exposure to broad-spectrum antibiotics, trends in antimicrobial resistance patterns, and associated costs, the aim of this study was to investigate PCPs’ perspectives on usefulness, attitudes, and perceived barriers and facilitators to one-on-one education via AD intervention provided by an A-team for ARI&AB. By understanding the acceptability and effectiveness of such intervention, it will be possible to develop future strategies for safe and prudent antibiotic use, address care gaps, and promote changes in practice in Croatia as well as in other countries.
Methods
Our prospective study was part of a larger investigation on AD in Croatia. We recruited PCPs in Koprivnica-Križevci County on a voluntary basis. The AD program aimed to improve antibiotic prescribing during April 2020. The A-team, comprising infectious disease physicians, clinical microbiologists, and clinical pharmacists, conducted a regular ASP at Koprivnica-Križevci County General Hospital. With that experience, they developed educational materials tailored for primary care settings to be delivered in a 30-minute AD visit. The intervention also involved the distribution of educational materials, including posters for PCPs’ practices and patient-friendly brochures that emphasized prudent antibiotic use. The AD intervention was provided once to each PCP who agreed to participate. AD sessions consisted of a face-to-face meeting that included sharing of data on local antibiotic consumption and antimicrobial resistance data, research evidence on the consequences of imprudent antibiotic use, national and international guidelines, and examples of improved prescribing through teamwork with patients and their families.21–23
In this study, qualitative research methods were applied, using a theoretically informed approach based on the conceptual framework of healthcare intervention implementability. This framework outlines factors that influence adoption of health interventions in routine practice, divided into five domains: acceptability, fidelity, feasibility, scalability, and sustainability. 24 We focused on the acceptability, 25 fidelity, 26 and feasibility 27 of AD intervention, which are crucial in the early phase of intervention development. Scalability and sustainability are dependent on these pre-conditions and should be re-evaluated as the intervention is implemented in diverse populations or settings. 24 The study adhered to the consolidated criteria for reporting qualitative research (COREQ) guidelines.28,29
Interview guide development
The research team, comprising experts in clinical pharmacy (DKP), infectology (VM), clinical microbiology (VJP), primary care (APA), university research clinical pharmacy (DKP), and a health services researcher (MK), developed a semi-structured interview guide (see Additional file 2). The guide was designed based on three domains of the healthcare intervention implementability framework: acceptability, fidelity, and feasibility. The questions explored PCPs’ views on the usefulness of AD, their attitudes toward AD, and their perceived effectiveness of AD intervention as an ASP. The investigated aspects of the domain fidelity included adherence to guidelines after AD intervention, likelihood of recommending the intervention to other PCPs, and potential for intervention repetition. Feasibility concerns were addressed, such as operational issues for AD implementation in everyday practice and any impact on PCPs’ practices. The interview started with open-ended questions, with subsequent follow-up prompts. A pilot test was conducted among three PCPs, two of whom were not part of the study, to ensure comprehension, clarity, and content validity of the questionnaire.
Ethical approval statement and consent to participate
This study was reviewed and approved by The Regional Ethical Committee for Medical and Health Research Ethics for Outpatient Clinics of Koprivnica-Križevci County (reference number 2137-16-5266/2021; 28 September 2021). All methods were carried out in accordance with Declaration of Helsinki and national relevant guidelines and regulations. Written and/or verbal informed consent was obtained from all participants depending upon whether the interview was conducted in person (written and verbal) or by telephone (verbal).
Recruitment and data collection
Selective recruitment for the study occurred between 1 September and 30 November 2022. All 16 PCPs from Koprivnica-Križevci County, Croatia who participated in a previous AD study were contacted. Qualitative interviews were conducted one-on-one by telephone or at each PCP’s clinic by a researcher (DKP) with qualitative research and AD experience. The study overview and sample questions were explained; with verbal consent, interviews were audio recorded and transcribed anonymously. The sample size was determined upon reaching theoretical saturation, meaning that no new information was obtained from additional interviews. Transcripts were offered for review, but all participants declined owing to time constraints. Data were securely stored at the General Hospital “Dr. Tomislav Bardek” Koprivnica. No compensation was provided to participants.
Data analysis
Two researchers (MK and DKP) conducted the analysis using an inductive approach based on reflexive thematic analysis, as proposed by Braun and Clarke. 30 The six-phase analysis framework was followed. The researchers familiarized themselves with the data by reading and highlighting key points. Codes were generated collaboratively, labeling data extracts and identifying patterns. Discussions and re-readings were carried out to refine the codes until all relevant data items were included. The themes were defined and a report was written. Owing to a manageable data volume, Microsoft Word was used for the analysis. The results were then mapped to the domains of acceptability, fidelity, and feasibility in the conceptual framework of implementability of healthcare interventions. PCPs’ details were de-identified such that participants could not be identified in any way.
Results
Of the 16 PCPs contacted, 14 completed the interview and were included in the analysis. Demographics, employment status, and location of PCPs’ practice are presented in Table 1. Regarding the reasons for declining to participate in the interview, one PCP expressed a lack of interest and the other was on long-term sick leave. Only female physicians agreed to participate in the study. Participants had practiced for an average 27.9 (standard deviation 11.9) years. Ten PCPs refused audio recording, so notes were taken. Interviews ranged from 20 to 40 minutes, averaging 30 minutes in length. Six themes were identified within the domains of acceptability, fidelity, and feasibility. Information and representative quotes for each theme are presented in Table 2.
PCPs’ demographic information, employment status, and location of practice
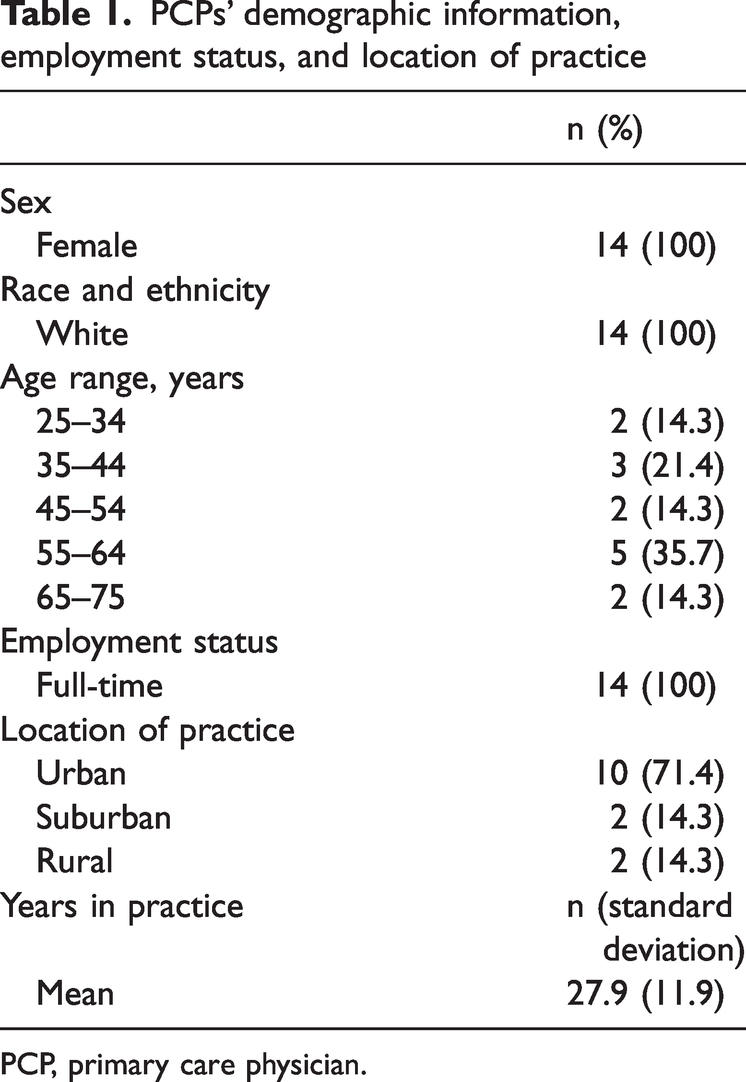
PCP, primary care physician.
Identified themes and relationships within the conceptual model.

Note: The table is based on an example plan for using the framework of implementability of Klaic M. et al., 2022.
AD, academic detailing; AMR, antimicrobial resistance; ASP, antimicrobial stewardship program; PCP, primary care physician.
Acceptability
Theme 1: Usefulness of AD as an ASP
The interview started with questions about PCPs’ antibiotic prescribing practices and changes since graduation from medical school. Most PCPs reported making changes with experience, but three said they had strictly maintained the same practices since graduation. One PCP was in the process of gaining further experience, and another did not specify a reason.
All PCPs agreed that the AD intervention was appropriate and useful for improving their practice. They discussed how participating in AD provided them with knowledge about the widespread issue of AMR in their community, which changed their attitude toward prescribing practices. They noted that this information was not available from other resources they had used previously. PCPs valued the clear explanation in the guidelines for practically treating ARI&AB, which was specific to their local practices. They also appreciated the focus on raising awareness about prudent antibiotic use as part of the AD intervention.
Before academic detailing, I knew about AMR, but I was not aware that AMR was so widespread in our county and that made me even more careful about what I am prescribing (PCP #2).
Factors that have made me stringent in antibiotic prescribing after AD include data on local antibiotic resistance patterns, recommendations from a microbiology specialist—such as in the case of a chronic wound swab that does not require antibiotics—and current developments in the field of antibiotic treatment (PCP #15).
Theme 2: Antibiotic prescribing over time and perceived effectiveness of AD
PCPs embraced the challenge of setting clear goals, aiming to be more stringent in their antibiotic prescribing decisions. Over time after AD, most PCPs reported effective rational prescribing owing to increased knowledge, an improved decision-making process, and greater self-confidence in not prescribing antibiotics.
Not a clear plan, but [after AD] I am trying more rigorously to decide based on the clinical status of patients, and if needed, ordering further laboratory tests. They can help me guide a decision on antibiotic prescribing. If laboratory tests show that the patient did not react to an antibiotic or the inflammatory markers are inside the reference range, I stop the antibiotic. But I prescribe antibiotics very rationally, so this does not happen often (PCP #2).
After undergoing academic detailing, I do not have a clear plan, but I am more cautious and take into consideration local antibiotic resistance patterns when making decisions on antibiotic prescriptions (PCP #3).
One PCP noted that AD intervention only confirmed her knowledge and current practices.
Fidelity
Theme 3: AD as an intervention for further reinforcement of prudent antibiotic use
PCPs improved their adherence to guidelines after AD intervention and stressed the importance of one or two lectures per year on maintaining restrictive antibiotic prescribing. They also highlighted the need for education among primary and secondary care colleagues, undergraduate students, preschoolers, school children, and patients. Written materials were suggested for further support.
Live lectures every 6 or 12 months in small groups, more like a workshop, to remind me to continue being adherent to guidelines, which were nicely presented at [AD] intervention (PCP #1).
Most PCPs agreed to recommend another AD intervention for colleagues from their practice, but two were unsure.
I think that [other PCPs] would be keen on getting to know current news regarding prudent use of antibiotics by having [AD] intervention or something similar (PCP #10).
Theme 4: Influence of pharmaceutical promotion on antibiotic prescribing practices after AD intervention
Most PCPs reported no influence from the pharmaceutical industry regarding antibiotic prescribing. AD intervention helped them stay up to date with the guidelines and ensure optimal patient care.
No, pharmaceutical representatives do not encourage me or my colleagues to prescribe more antibiotics. I also refreshed my knowledge through AD intervention, which made me more self-confident; therefore, it would be more difficult for them if trying to persuade me to prescribe what they want. Actually, they do not come so often for information on antibiotics, as is the case for other classes of medicines (PCP #10).
Only one PCP reported an influence:
Yes, pharmaceutical representatives try to influence my prescribing practices for antibiotics, although I do not follow their recommendation if not necessary. An example is when changing the prescribed antibiotic to one from another manufacturer owing to unavailability of the prescribed antibiotic (PCP #9).
Feasibility
Theme 5: Working environment barriers to implementing AD
Despite its practicality and high acceptance, PCPs acknowledged that the work environment can influence their prescribing practices. PCPs reported that they sometimes yield to patient pressure or recommendations from other healthcare specialists or a combination of both. After the AD intervention, PCPs also identified lack of time as a barrier to adhering to prudent antibiotic prescribing. As for challenges, three PCPs mentioned a shortages of antibiotics, and one mentioned a lack of point-of-care tests.
I think I have just one big barrier, which is pressure from patients. But in the current situation, we also have shortages of antibiotics, such as co-amoxiclav, so we have to prescribe another generation of antibiotics; but this is an extraordinary situation. It is not my everyday practice. Also, I would like to add a lack of point of care tests in everyday practice, which would make AD intervention even more successful (PCP#2).
Theme 6: Impact of AD intervention on concerns regarding PCP practices
Almost all PCPs expressed confidence that the AD intervention reinforced their responsible prescribing habits.
I am not worried about an impact on my practice. [Patients] are aware of my responsible prescribing habits and AD intervention confirmed my approach in maintaining my rigorous prescribing practices. I am also aware that my patients go to other PCPs seeking antibiotics if I do not prescribe them. They always come back to me with other issues not related to antibiotics as they know my attitude. But I am not concerned about it at all (PCP #16).
Only one PCP reported an occasional concern:
Depends on the situation, sometimes yes and sometimes I am not [concerned about the impact on my practice]. What really concerns me is that, despite a lot of effort and time dedicated to explaining, patients still do not have an understanding of why they did not get antibiotics and go elsewhere seeking an antibiotic. This kind of [AD intervention] education should also be designed for patients to better understand the importance of prudent antibiotic use and their active involvement in this (PCP #12).
PCPs’ views on the scalability and sustainability of AD in the Croatian healthcare system were not explored in depth and are encompassed within the domains of fidelity (themes 3 and 5) and feasibility for scalability (theme 5).
Discussion
Our study aimed to explore the views of PCPs regarding implementation of AD as an ASP in Croatia with respect to usefulness, attitudes, and perceived barriers and facilitators to changing prescribing practices, including during the COVID-19 era. We found that pressure from patients and recommendations from hospital specialists were the main barriers to AD implementation. Despite challenges, PCPs appreciated the direct interaction and evidence-based practices promoted in AD, suggesting its potential to reduce inappropriate antibiotic use and combat AMR. This study underscores the importance of personalized interaction with experts to address knowledge gaps and promote responsible antibiotic use. However, our study was focused on PCPs’ opinions and attitudes and lacked objective outcomes. Further research is needed to assess the effectiveness of AD in reducing inappropriate antibiotic prescribing and improving patient outcomes.
The impact of COVID-19 on the diagnosis and treatment of ARI&AB is a crucial consideration in the context of this study. It also underscores the need for ongoing research and investigation into the intersection of infectious diseases and AMR. The COVID-19 pandemic has substantially altered the diagnostic process for these diseases owing to the overlap of symptoms with COVID-19, potentially impacting the accuracy of diagnoses and treatment decisions.31–33 This may lead to challenges in distinguishing between COVID-19 and other respiratory illnesses as well as the possibility of misdiagnosis or delayed diagnosis. 34 The weighted-incidence syndromic combination antibiogram could be used as a tool to combat these difficulties, including AMR. Because this approach considers the body site from which the organism is recovered, it gives a weighted susceptibility to all organisms causing a specific infection-related syndrome. 35 This may comprise a part of AD, if available, with an A-team ensuring the dissemination of syndromic antibiogram results among healthcare professionals. As such, it is essential for healthcare professionals to remain informed about the latest diagnostic protocols and guidelines and to collaborate with infectious disease experts (such as an A-team) to ensure the most accurate diagnoses and treatments. Furthermore, this study highlights the importance of developing and implementing adaptive strategies for addressing the growing threat of AMR, considering the constantly evolving landscape of infectious diseases. For instance, evidence-based behavior change techniques that emphasize the importance of health consequences have been shown to be effective in improving prescribing practices, especially when targeting individual physicians rather than larger groups or institutions.36,37 We recommend repeating and evaluating these techniques at least once or twice per year, as suggested by the PCPs in our study, to assess the sustainability of AD. Furthermore, regular AD interventions can also increase PCPs’ self-confidence in resisting patients’ demands, which was identified as a leading driver of inappropriate prescribing in our study as well as in other studies.36,38 Future research should examine how our AD intervention can be scaled up, as it is shown to increase PCPs’ confidence in using their clinical judgment for prudent antibiotic prescribing.
Additionally, it may be important to consider the potential impact of COVID-19 on patients’ demands for antibiotics because patients may be more likely to request antibiotics out of fears related to COVID-19. Consequently, it may be beneficial to include evidence-based behavior change techniques that address patient demands in addition to those emphasizing the importance of antibiotics’ health consequences. The approach to tackle AMR is relevant but the impact of COVID-19 on the diagnostic process and patients’ behavior toward antibiotics should also be considered.
Among others, fear of complications and insufficient knowledge about ARI&AB are important factors that contribute to inappropriate antibiotic prescribing.36,39 In our research, we found that PCPs do not fear complications of ARI&AB but rather that hospital physicians recommend antibiotics owing to fear of these complications. To overcome this challenge, improving education and knowledge could have a large impact on reducing unnecessary antibiotic prescribing. PCPs should be provided with facts regarding the rarity of ARI&AB complications compared with the frequency of antibiotic-associated adverse drug events. For instance, the number needed to treat to prevent one serious complication is more than 4000, whereas 19.3% of all emergency department visits are related to drug-related adverse events.40–42 This information can have an important impact on reducing unnecessary antibiotic prescribing. In addition to improving education and knowledge, regular AD intervention can also help reduce the number of recommendations for antibiotics from hospital healthcare specialists and increase PCPs’ confidence in using their clinical judgment for prudent antibiotic prescribing. Supporting approaches that target changing these factors can help overcome the challenge of inappropriate antibiotic prescribing for fear of complications and insufficient knowledge about ARI&AB.
In addition to the factors mentioned above, our study also aimed to explore other potential drivers of inappropriate antibiotic prescribing. Interestingly, we found that PCPs are not concerned about losing patients or receiving encouragement from the pharmaceutical industry. This is a crucial finding because these factors are often mentioned as potential drivers of inappropriate antibiotic prescribing. The lack of concern about losing patients may indicate that PCPs prioritize the health and well-being of their patients above all else. This finding is reassuring as it suggests that PCPs are not motivated by financial gain or personal interest when making decisions about antibiotic prescribing. Similarly, the lack of concern about receiving encouragement from the pharmaceutical industry suggests that PCPs are not influenced by external pressures or incentives to prescribe antibiotics. This finding is of interest because the pharmaceutical industry has been known to engage in marketing practices that promote the use of antibiotics, even when they are not medically necessary. These findings have important implications for efforts to reduce inappropriate antibiotic prescribing, suggesting that interventions targeting changes in PCPs’ attitudes and behaviors may be more effective than interventions focused solely on external factors, such as financial incentives or marketing practices.
Antibiotic shortages is an issue that has been increasingly reported by healthcare providers in recent years.43,44 Although only a few participants in our study reported this as a problem, it is important to acknowledge the potential impact of shortages on irrational antibiotic prescribing. Because antibiotics are the medication most affected by shortages, substitution remains a leading strategy to mitigate this issue. However, this strategy carries several risks, including the potential for AMR and suboptimal health outcomes. 44 To address this issue, it is important to provide education and training to healthcare providers, such as via AD intervention, to ensure that appropriate prescribing practices are followed even in the context of shortages. This could include strategies to optimize the use of antibiotics, such as limiting their use to patients who truly need them and using narrow-spectrum antibiotics whenever possible. Additionally, it may be necessary to explore alternative strategies to manage infections in the context of shortages, such as using non-antibiotic therapies or infection prevention and control measures to reduce the spread of infection. Addressing the issue of antibiotic shortages and ensuring that healthcare providers have the tools and knowledge necessary to make informed decisions about antibiotic prescribing can help mitigate the potential harms associated with antibiotic shortages and ensure that patients receive the appropriate care they need.
Future research should focus on designing educational programs using AD as a strategy for mitigating AMR, which can assist policymakers in creating an environment that fosters prudent antibiotic use. AD can provide personalized interaction with experts in the field, which can help address any uncertainties related to the diagnosis and treatment of ARI&AB, especially within the context of the COVID-19 era. This approach can also improve communication and information exchange between hospital and community settings, which is crucial to ensuring that patients receive appropriate care.45,46 Future research should also evaluate the effectiveness and sustainability of AD interventions in different settings and populations and explore ways to scale up these interventions to reach more healthcare providers. Additionally, researchers should investigate the impact of AD on patient outcomes, such as antibiotic resistance and adverse drug events, to determine the full extent of its benefits. Overall, AD has the potential to be a valuable tool in the fight against AMR and should be further explored and utilized in educational programs aimed at improving antibiotic prescribing practices.
Despite its contributions, our study has several limitations that should be considered. One of the main limitations is the small number of PCPs who participated in the AD intervention owing to the low response rate and their availability. PCPs have a heavy workload, making it difficult for them to participate in non-essential activities such as research. Moreover, the PCPs who participated in this study may be more open to new experiences and more willing to share their views on prescribing practices than those who did not participate. Because this was a qualitative study, we were unable to measure the effectiveness of AD intervention in terms of real outcomes. To elucidate how to improve antibiotic prescribing practices, a quantitative study has also been performed, which is registered on ClinicalTrials.gov with the identifier NCT05090475. Furthermore, the geographic specificity of our study, which was conducted among PCPs in Croatia, may also limit the generalizability of our results to other healthcare settings or countries. However, using a qualitative approach allowed us to gain a deeper understanding of the subjective experiences and perspectives of PCPs, which can provide valuable information for the development of future ASPs that are effective and acceptable in various healthcare settings.
Conclusion
Our study investigated the opinions of PCPs after AD and their behavioral changes in decision-making regarding antimicrobial drug prescription, specifically in the context of ARI&AB, which is particularly relevant in the challenging era of COVID-19. Our findings demonstrate the potential of AD as part of a broader strategy for antimicrobial stewardship in improving the quality of broad-spectrum antibiotic prescribing in primary care. By promoting evidence-based practices through direct interactive education, AD may be an effective intervention to reduce the negative consequences of inappropriate antibiotic use on public health and slow the spread of AMR. However, further research is needed to determine the effectiveness of AD in reducing inappropriate antibiotic prescribing and improving patient outcomes. Furthermore, continuing education for both PCPs and other healthcare professionals is critical to transform the culture of irrational antibiotic prescribing. The insights gained from our study may inform the development of future ASPs and help policymakers create targeted initiatives to enhance clinical decision-making, focusing on AD implementation and collaboration between primary and secondary healthcare. Although education itself may not be a standalone solution, it remains a valuable tool in broader efforts to address the complex challenges posed by AMR.
Supplemental Material
sj-pdf-1-imr-10.1177_03000605231222242 - Supplemental material for Perspectives of primary care physicians on academic detailing for antimicrobial stewardship: feasibility and impact assessment
Supplemental material, sj-pdf-1-imr-10.1177_03000605231222242 for Perspectives of primary care physicians on academic detailing for antimicrobial stewardship: feasibility and impact assessment by Darija Kuruc Poje, Maja Kuharić, Ana Posavec Andrić, Vesna Mađarić, Janeš Vlatka Poje, Marina Payerl-Pal, Arjana Tambić Andrašević, Juraj Mark Poje, Vesna Bačić Vrca and Srećko Marušić in Journal of International Medical Research
Supplemental Material
sj-pdf-2-imr-10.1177_03000605231222242 - Supplemental material for Perspectives of primary care physicians on academic detailing for antimicrobial stewardship: feasibility and impact assessment
Supplemental material, sj-pdf-2-imr-10.1177_03000605231222242 for Perspectives of primary care physicians on academic detailing for antimicrobial stewardship: feasibility and impact assessment by Darija Kuruc Poje, Maja Kuharić, Ana Posavec Andrić, Vesna Mađarić, Janeš Vlatka Poje, Marina Payerl-Pal, Arjana Tambić Andrašević, Juraj Mark Poje, Vesna Bačić Vrca and Srećko Marušić in Journal of International Medical Research
Footnotes
Acknowledgements
We would like to extend our sincere thanks to everyone who participated in the project: primary care physicians, administrative assistants, IT assistants, and principals from all relevant health care institutions. Special thanks to supporters of the project, namely, Darko Koren and Ratimir Ljubić from Koprivnica-Križevci County and Mato Devčić from General Hospital “Dr. Tomislav Bardek” Koprivnica, Croatia.
Author contributions
The study design was developed by DKP, MK, APA, VM, and VJP. Data collection was done by DKP. Data analysis and writing were conducted by DKP and MK. Reviewing an editing was carried out by MPP, ATA, JMP, VBV, and SM. All authors read and approved the final manuscript.
Data availability statement
The datasets used and analyzed in this study are not publicly available but are available from the corresponding author upon reasonable request.
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.