
Abstract
Objectives:
“Nosocomial infections” or “healthcare-associated infections” are a significant public health problem around the world. This study aimed to assess the rate of laboratory-confirmed healthcare-associated infections, frequency of nosocomial pathogens, and the antimicrobial resistance patterns of bacterial isolates in a University Hospital.
Methods:
A retrospective evaluation of healthcare-associated infections in a University Hospital, between the years 2015 and 2019 in Tekirdag, Turkey.
Results:
During the 5 years, the incidence densities of healthcare-associated infections in intensive care units and clinics were 10.31 and 1.70/1000 patient-days, respectively. The rates of ventilator-associated pneumonia, central line–associated bloodstream infections, and catheter-associated urinary tract infections in intensive care units were 11.57, 4.02, and 1.99 per 1000 device-days, respectively. The most common healthcare-associated infections according to the primary sites were bloodstream infections (55.3%) and pneumonia (20.4%). 67.5% of the isolated microorganisms as nosocomial agents were Gram-negative bacteria, 24.9% of Gram-positive bacteria, and 7.6% of Candida. The most frequently isolated causative agents were Escherichia coli (16.7%) and Pseudomonas aeruginosa (15.7%). The rate of extended-spectrum beta-lactamase production among E. coli isolates was 51.1%. Carbapenem resistance was 29.8% among isolates of P. aeruginosa, 95.1% among isolates of Acinetobacter baumannii, and 18.2% among isolates of Klebsiella pneumoniae. Colistin resistance was 2.4% among isolates of A. baumannii. Vancomycin resistance was 5.3% among isolates of Enterococci.
Conclusion:
Our study results demonstrate that healthcare-associated infections are predominantly originated by intensive care units. The microorganisms isolated from intensive care units are highly resistant to many antimicrobial agents. The rising incidence of multidrug-resistant microorganisms indicates that more interventions are urgently needed to reduce healthcare-associated infections in our intensive care units.
Introduction
Healthcare-related infections (HAIs), previously referred to as nosocomial infections (NIs), are infections acquired by patients in healthcare settings. It usually occurs 48–72 h after the patient’s hospitalization or within 10 days after discharge. Many studies have shown that the most common events that affect hospitalized patients are drug side effects, NI, and surgical complications.1–3 The US Centers for Disease Control and Prevention (CDC) reported that approximately 1.7 million hospitalized patients annually acquire HAIs or NIs while being treated due to other health problems and that more than 98,000 of these patients (approximately 1 in 17) die due to HAIs. HAIs are reported to be one of the 10 most important causes of death in the United States. However, the World Health Organization reports that HAIs usually attract public attention when an outbreak occurs.3–5
HAIs have a dynamic process that varies in each center and over time. In many European multicenter studies, 4.6%–9.3% of hospitalized patients have been reported to develop NIs. In another study, the frequency of HAIs was 5.9% (country range: 2.9%–10.0%). This rate was 7% in tertiary hospitals. In various studies conducted in our country, the rate of healthcare-associated infection has been reported between 1% and 16%. HAIs are most commonly associated with invasive medical devices or surgical procedures. Intensive care unit (ICU) patients have a higher risk of developing HAIs compared to other hospitalized patients.2,6–9
Despite the early diagnosis of infections and improvements in hospital conditions, HAIs continue to pose a significant risk of morbidity and mortality. In addition to increased morbidity and mortality, length of hospital stay, antibiotic use, the risk of developing multiple antibiotic resistance of pathogens, and maintenance costs increase. Lower respiratory tract and bloodstream infections are the most fatal. Prevention of HAIs is the responsibility of healthcare institutions and their employees. Everyone should work collaboratively to reduce the risk of infection for patients and staff. Surveillance of HAIs is an important part of infection control and has been widely accepted worldwide as a primary step toward prevention. Local surveillance data are also important to guide empirical treatment and to ensure optimal therapy. Therefore, each center should determine its own distribution of HAIs, causative agents, and their antibiotic resistance status to guide the development of infection control policies. In this study, we aimed to evaluate the incidence of laboratory-confirmed HAIs, distribution of infections, infectious agents, and antibiotic resistance status of these agents in Namik Kemal University Hospital during the years 2015 and 2019.
Materials and methods
Study design—data collection
This study was a retrospective analysis of laboratory-confirmed HAIs of hospitalized patients at the Namik Kemal University Hospital, a tertiary care hospital with 430 beds, between the years 2015 and 2019. The ICUs had 80 beds. Patient data were obtained by laboratory and patient-based active surveillance methods. Follow-up, registration, and examination of HAIs were carried out by the infection control team. All cases with NI were recorded by using a standard data collection form that included the patient’s name, age, sex, microbiological culture results, underlying conditions, risk factors for NIs, interventions at the hospital, the reason for hospitalization, and treatment for all patients. Patients hospitalized in ICUs were followed by an Infectious Disease specialist and an Infectious Disease Nurse Daily. Patients hospitalized in other units were followed by an infection control team three times a week. The study included all patients hospitalized for more than 48 h. The overall patient HAI rate, the incidence density, and device-associated HAI rates were determined. All HAIs were culture-confirmed.
The bacterial identification was performed by the automatized VITEK 2 (bioMérieux, France) in addition to conventional microbiological methods. The Kirby-Bauer disk diffusion method and automatized VITEK 2 system determined the antibiotic resistance patterns of isolated microorganisms. The presence of extended-spectrum beta-lactamase (ESBL) positivity was detected using the double-disk synergy test (DDST).
This study was approved by the Ethical Committee of Namik Kemal University, Faculty of Medicine (approval number 2021.15.01.15). Written informed consent was waived by the Ethical Committee because of the retrospective nature of this study.
Statistical analysis
Variations in the resistance rate during the 5-year period were analyzed by the chi-square test for trends. p-value < 0.05 was considered significant.
Definition
The incidence rates of HAIs were calculated by dividing the total number of patients with HAIs by the total number of patients (×100) during the observed period. The incidence density of HAIs was calculated by dividing the total number of HAIs recorded in the observed period by the total number of patient days (×1000).
A bloodstream infection (BSI) was classified as primary in the absence of an identified source of infection or if it was catheter-related. A BSI was classified as secondary in the presence of an identified source infected with the same microorganism at another body site. Device-associated HAI rates of ventilator-associated pneumonia (VAP), central line–associated bloodstream infections (CLA-BSI), and catheter-associated urinary tract infections (CA-UTIs) per 1000 device-days were calculated by dividing the total number of device-associated HAI by the total number of specific device-days and multiplying the result by 1000.
Multidrug-resistant (MDR) Gram-negative bacteria were defined as Gram-negative bacteria resistant to at least one agent in each of three or more categories of antimicrobial agents including β-lactam/β-lactamase inhibitor combinations (piperacillin/tazobactam), extended-spectrum cephalosporins (ceftriaxone, ceftazidime, cefepime), carbapenems (imipenem/meropenem), monobactams, aminoglycosides (gentamicin, amikacin), and/or fluoroquinolones. In Gram-positive bacteria, vancomycin resistance for Enterococcus faecium and methicillin resistance for Staphylococcus aureus have been defined as MDR.
Inclusion criteria
Being hospitalized for more than 48 h in the study hospital.
HAI was diagnosed using the CDC case definitions. 10
Exclusion criteria
Patients who developed infections before or in the first 48 h of hospitalization.
Results
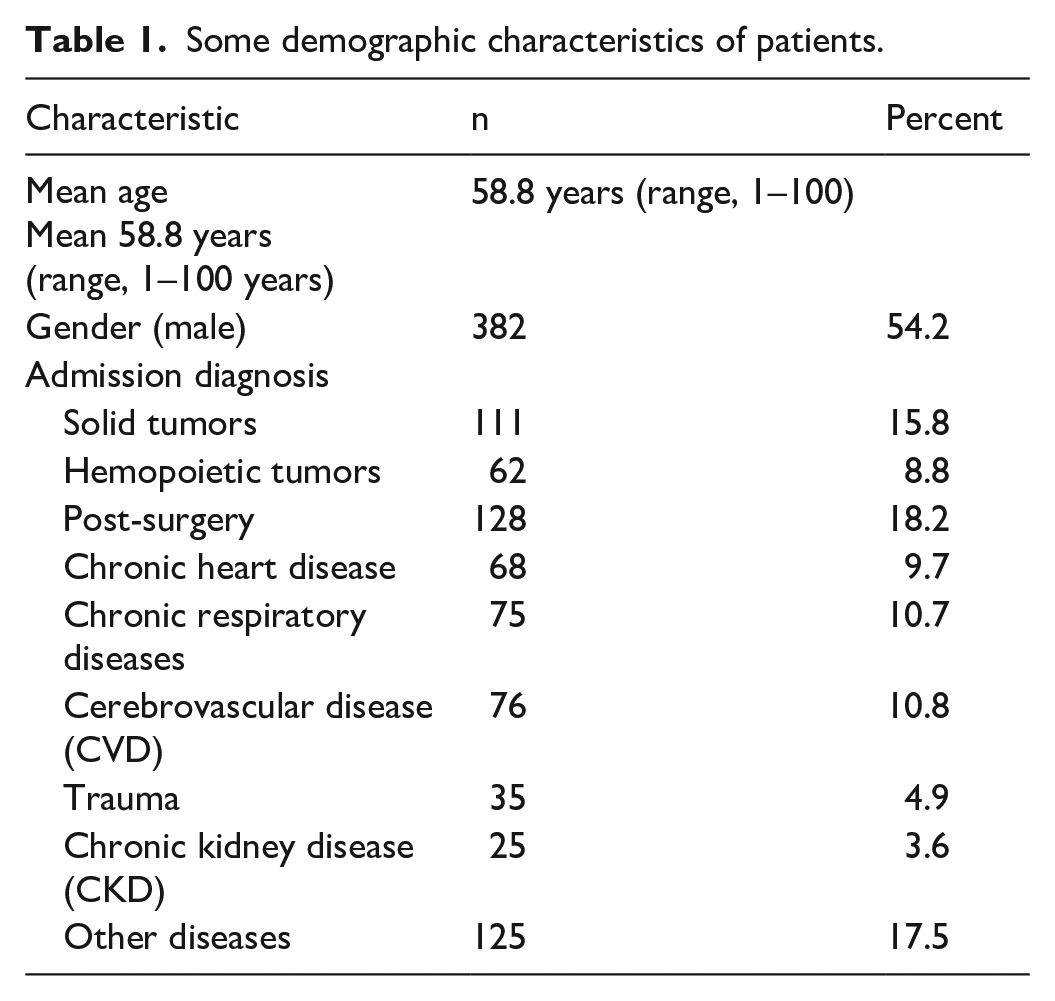
During the study period, 1050 laboratory-confirmed HAI episodes were detected in 705 patients aged <1–100 years old (age: 58.8). In total, 382 (54.2%) patients were males. The majority of the patients were on admission following surgery 128 (18.2%), followed by solid tumors 111 (15.8%) and cerebrovascular disease (CVD) 76 (10.8%). The demographic characteristics of patients are given in Table 1. The total number of inpatients was 53,716. The overall incidence rates (HAI/100) and incidence densities (HAI/1000 patents days) of HAIs were 1.95% and 3.58/1000 patient-days, respectively. In total, 603 (57.4%) of the infections originated from the ICUs. The incidence rates of HAIs in ICUs and clinics were 5.73 and 0.92/100 patients, respectively. The incidence densities of HAIs in ICUs and clinics were 10.31 and 1.70/1000 patient-days, respectively. The distribution of infection rate and density by year is given in Table 2.
Some demographic characteristics of patients.
The distribution of HAIs.
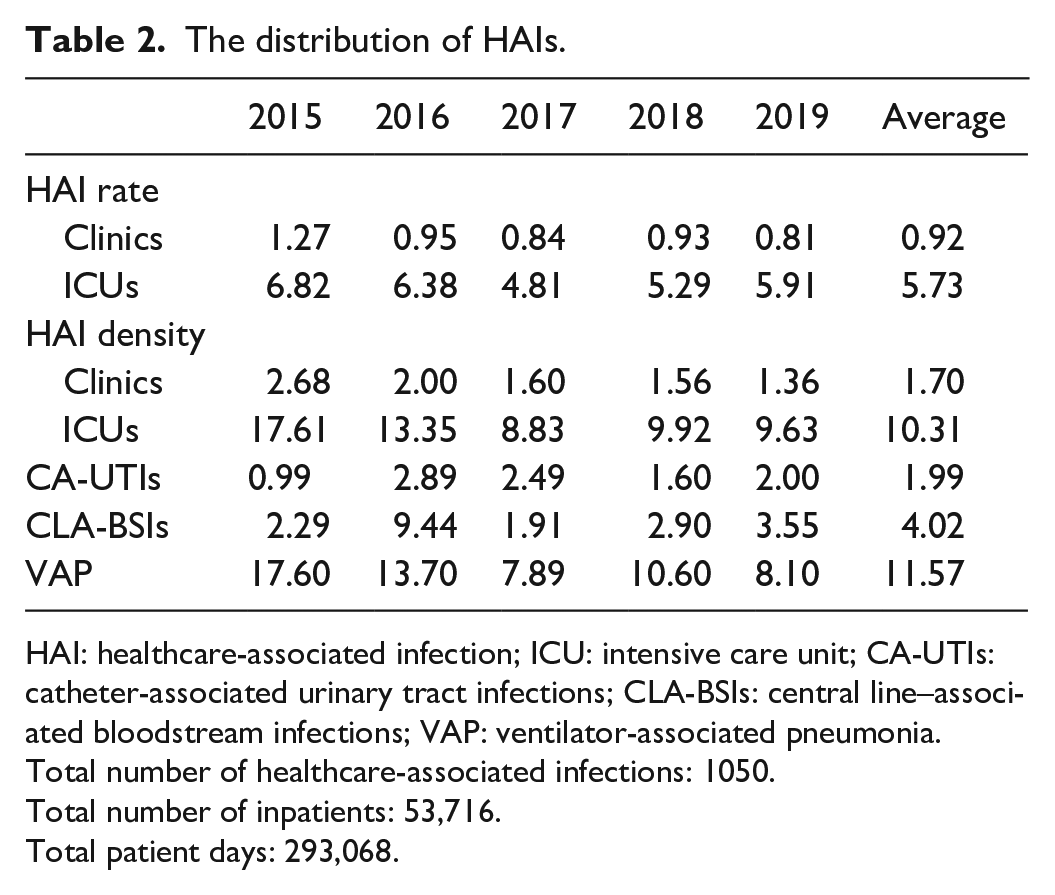
HAI: healthcare-associated infection; ICU: intensive care unit; CA-UTIs: catheter-associated urinary tract infections; CLA-BSIs: central line–associated bloodstream infections; VAP: ventilator-associated pneumonia.
Total number of healthcare-associated infections: 1050.
Total number of inpatients: 53,716.
Total patient days: 293,068.
HAIs according to the primary sites were BSIs (55.3%), pneumonia (20.4%), surgical site infections (SSIs) (13.7%), and urinary tract infections (UTIs) (9.5%). BSIs were the most common hospital infections, followed by VAP in 2015, 2017, 2018, and 2019, and SSIs in 2016. 19.5% of BSIs are secondary BSIs. 34% of BSIs were catheter-related BSIs, 47.5% of BSIs were BSI without invasive device-related. The rates of VAP, CLA-BSIs, and CA-UTIs in ICUs were 11.57, 4.02, and 1.99 per 1000 device-days, respectively.
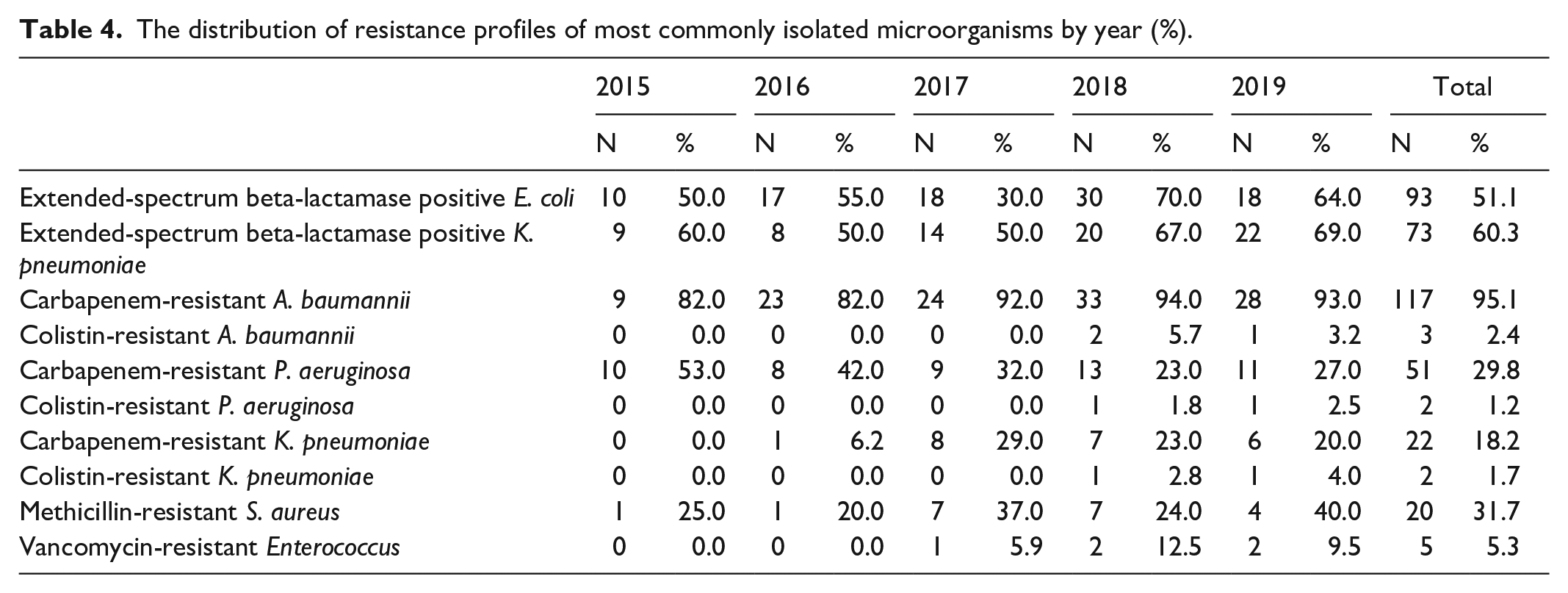
In total, 732 (67.5%) of the isolated microorganisms as nosocomial agents were Gram-negative bacteria, 271 (24.9%) of Gram-positive bacteria, and 82 (7.6%) of Candida. 35.3% of the Candida were Candida albicans. The most frequently isolated microorganisms were Escherichia coli (E. coli) (16.7%) followed by Pseudomonas aeruginosa (P. aeruginosa) (15.7%), Acinetobacter baumannii (A. baumannii) (11.3%), Klebsiella pneumoniae (K. pneumoniae) (11.1%), and coagulase-negative Staphylococci (CoNS) (10.0%). The most frequently isolated microorganisms were CoNS and E. coli in BSIs; E. coli and P. aeruginosa in urinary tract infections; E. coli in SSIs; and P. aeruginosa and A. baumannii in VAP, respectively. The distribution of the most commonly isolated microorganisms according to the type of infection is given in Table 3. The prevalence of ESBL-producing K. pneumoniae was 60.3% and E. coli was found as 51.1%. In this study, all ESBL-producing E. coli isolates were sensitive (100%) to meropenem and K. pneumoniae showed 81.8% sensitivity to meropenem. Carbapenem resistance was 29.8% among isolates of P. aeruginosa; 95.1% among isolates of A. baumannii. Colistin resistance was 2.4% among isolates of A. baumannii, 1.2% among isolates of P. aeruginosa, and 1.7% among isolates of K. pneumoniae. Methicillin resistance was 31.7% and 83.4% among isolates of Staphylococcus aureus and CoNS, respectively. All Staphylococci isolates were susceptible to vancomycin and linezolid. Vancomycin resistance was 5.3% among isolates of Enterococci. The prevalence of NIs caused by MDR bacteria was 45.66%. The distribution of the resistance profiles of nosocomial pathogens by year is given in Table 4. Carbapenem resistance among P. aeruginosa isolates was decreased slightly from 53% to 27% in the last 2 years; however, this trend was not significant statistically (p > 0.05). There was no statistically significant difference between ESBL-producing K. pneumoniae numbers in comparisons of 5 years (p > 0.05). There was a statistically significant decrease in 2017 in EBSL-producing E. coli (p < 0.05).
The distribution of the most isolated microorganisms according to the type of infection.
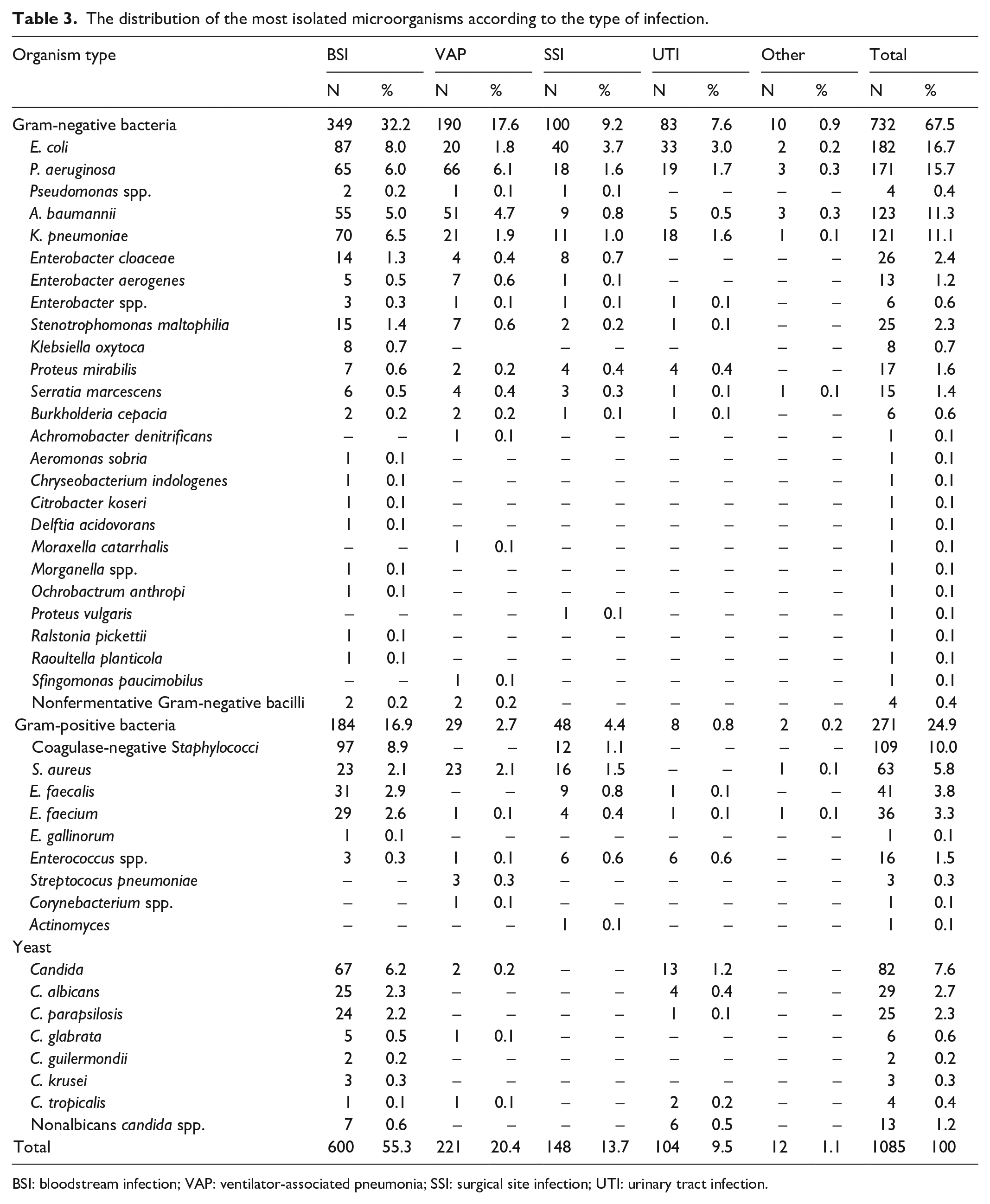
BSI: bloodstream infection; VAP: ventilator-associated pneumonia; SSI: surgical site infection; UTI: urinary tract infection.
The distribution of resistance profiles of most commonly isolated microorganisms by year (%).
Discussion
According to the data of our hospital, the incidence densities of HAIs in ICUs and clinics were 10.31 and 1.70/1000 patient-days, respectively. The incidence densities of HAIs acquired from ICUs were approximately 5–10 times higher than those acquired from clinics. There are also studies with the same values as our study results. HAI prevalence in the European Union/European Economic Area was 5.9% (country range: 2.9%–10.0%). 7 The rate of HAIs in our country is reported to be between 1.3% and 16.6% in the various studies. 9 In a study, the HAI rate was 1.6, and HAI density was 3.6. 11
Wenzel et al. 12 reported that although 5%–10% of hospitalized patients were followed in the ICU, 25% of HAIs were seen in this unit. In our study, 57.4% of HAIs were originated from ICUs. 18.6% of the beds in our hospital are intensive care beds. The rate of HAIs was higher than other services in our hospital too. Patients in ICUs are with a worse general condition who remain in the hospital for a long time period and with more frequent invasive procedures, more resistant bacterial infections, and more frequent use of antibiotics. According to the data, device-related infection rates in a multicenter study from Turkey were 4.86–16.69 per 1000 device-days for ventilator-related events, 1.59–4.98 for catheter-related urinary tract infections, and 2.82–5.65 for BSIs, respectively. 13 According to our data, the rates of VAP, CLA-BSIs, and CA-UTIs in ICUs were 11.57, 4.00, and 1.99 per 1000 device-days, respectively. It has been seen that our results are in the average Turkey values.
The most common HAIs are urinary tract infections (UTIs), pneumonia, BSIs, and SSIs. 14 In some studies, respiratory tract infections were the most common type.15–17 There are also some studies that indicate that SSIs are more common. 11 In our hospital, 53.5% of HAIs were BSIs. While 34% were catheter-related BSIs, 19.5% were secondary BSIs. 47.5% of BSIs were BSI without invasive device-related. 20.4% of VAP were accompanied by BSIs, 13.7% were SSIs, and 9.5% were UTIs. Healthcare-associated BSIs are an important cause of morbidity and mortality. Appropriate empirical antibiotic therapy is known to be the most effective treatment for BSIs, as shown in many studies. With preventive efforts, BSIs can be reduced. 14 Based on these findings, preference for the subclavian region for central venous catheter (CVC) insertion, use of chlorhexidine for cleaning the site before central line insertion, and application of maximum sterile barrier precautions (sterile gloves, long-sleeved sterile gown, mask, hood, and large, sterile sheet cover) have been added to our local guidelines. In our hospital, infection prevention and care bundles started to be used in 2021. It is hoped that HAIs will decrease with daily monitoring of infection prevention and care bundles, especially in ICUs.
Gram-negative bacteria have been reported as causative agents in approximately half of all HAIs. These bacteria predominate in most cases of VAP and urinary tract infections. Acinetobacter is the only Gram-negative bacillus that increased significantly in incidence as a cause of VAP compared to previous years. In the SENTRY Antimicrobial Surveillance Program study, Acinetobacter species were accounted for 7% of ICU infections in the United States and European countries.18–21 Infections caused by non-fermentative Gram-negative bacteria have increased compared to previous years in our study.
Microorganisms that cause HAIs are often resistant to antimicrobial agents. Unfortunately, the dramatic increase in MDR microorganisms including P. aeruginosa, A. baumannii, and ESBL-producing or carbapenemase-producing Enterobacteriaceae have been reported as agents of NIs in recent decades. For example, 50%–60% of more than 2 million NIs in the United States are caused by antibiotic-resistant pathogens. The incidence of MDR Gram-negative bacteria in the ICU is higher compared with other hospital units. Antibiotic use has been identified as an important risk factor in the emergence of antibiotic resistance. 22 In this study, the prevalence of NIs caused by MDR bacteria was 45.66%.
MDR microorganism is a serious public health problem in the world. The treatment is difficult, and morbidity and mortality are high. Antibiotics used in the treatment are limited, patients have longer hospital stays, and increased treatment costs. In a European study, one out of every 20 inpatients reported that health-related infections developed and the causative microorganisms (Klebsiella pneumoniae and Acinetobacter spp.) were generally multiple resistant.6,8,23 In a systematic review of Southeast Asian countries (Brunei, Myanmar, Cambodia, East Timor, Indonesia, Laos, Malaysia, Philippines, Singapore, Thailand, and Vietnam), the prevalence of HAI was 9.1% and the common microorganisms were P. aeruginosa, Klebsiella spp., and A. baumannii. 24 The most common causative agent of HAIs was Gram-negative bacteria in our hospital. The most resistant microorganism in our study was Acinetobacter spp. The rate of ESBL-producing E. coli and K. pneumoniae was high. About 51.1% of E. coli and 60.3% of K. pneumonia isolates were identified as ESBL producers. It is interesting that the susceptibility of P. aeruginosa to carbapenems remains high. Carbapenem resistance was 29.8%, 95.1%, and 18.2% in P. aeruginosa, A. baumannii, and K. pneumoniae isolates, respectively. Especially in A. baumannii isolates, antibiotic resistance was higher than in other isolates. Microorganisms isolated from ICUs showed high resistance to many antimicrobial agents. In the last 2 years, there was an increase in infections caused by colistin-resistant P. aeruginosa, A. baumannii, K. pneumoniae, and carbapenem-resistant K. pneumoniae. In addition, the increasing rate of carbapenem-resistant K. pneumoniae and vancomycin resistance Enterococcus (VRE) has also emerged. Carbapenem resistance among A. baumannii isolates was very high and the same trend during the study period. Unnecessary antibiotic administration and prolonged intensive care hospitalization may increase the spread of MDR pathogens. Monitoring of antimicrobial susceptibility and appropriate antimicrobial use might be effective to prevent the emergence of antimicrobial resistance in ICUs.
Limitations of study
This study has several limitations. It is a retrospective, single-center study with limited sample size. In addition, there was no systematic post-discharge follow-up to assess whether patients developed SSIs. However, one trained infection control doctor (MI) and the same infection control nurses conducted all data, which was a major advantage of our investigation.
Conclusion
In conclusion, this study demonstrates a high rate of antimicrobial resistance to commonly prescribed antibiotics among the microorganisms isolated from patients with HAIs hospitalized in ICUs. Infection control and antibiotic management strategies should be reconsidered in our ICUs. We know that an insufficient number of nurses is an important problem in the ICUs of Namik Kemal University Hospital which may explain why effective strategies are needed to prevent and control HAIs.
Footnotes
Author contributions
I.E. and I.Y. made contributions to the study design and lead data acquisition as well as analysis and interpretation of data. I.E., I.Y., B.S., B.E., M.D., C.K., and C.A. designed the study and made substantial contributions to the analysis and interpretation of data. I.E., R.K., E.A., I.Y., M.E.K., E.Y., and K.S.K. took part in data acquisition. All authors read and approved the final manuscript.
Availability of data and materials
All necessary data supporting our findings are contained in the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
This study was approved by the Ethical Committee of Namik Kemal University, Faculty of Medicine (approval number 2021.15.01.15).
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was waived by the Ethical Committee because of the retrospective nature of this study.