
Abstract
Objective
Urinary tract infections (UTI) are common during pregnancy. Identification of antimicrobial susceptibility patterns of microorganisms in pregnant women is important to select the most appropriate antimicrobial. We assessed common uropathogens in pregnant women with UTI and antimicrobial susceptibility, to guide empirical antibiotic selection.
Methods
In this retrospective study, we analyzed mid-stream urine culture and antibiotic susceptibility data from pregnant women who attended Jordan University Hospital during 2014 to 2018. Data were collected from patients’ charts and urine cultures, and sensitivity results were extracted from the laboratory electronic system. We calculated descriptive statistics and determined correlations among pathogens and antibiotics.
Results
We examined 612 positive urine cultures from 559 pregnant women, including 163 (29.2%) inpatients. Escherichia coli (29.4%) was the most frequently identified microorganism, followed by coagulase-negative staphylococci (CoNS) (21.6%). All bacterial isolates were sensitive to aztreonam, chloramphenicol, fosfomycin, ofloxacin, pefloxacin, piperacillin, and colistin sulfate; 87.5% were sensitive to amikacin. Only 15.79%, 18.93%, and 17.91% were sensitive to oxacillin, nalidixic acid, and erythromycin, respectively.
Conclusion
E. coli and CoNS were the most commonly identified microorganisms in this study. We found increased antibiotic resistance in Enterobacter species. The chosen antimicrobial therapy in pregnancy should be determined by sensitivity/resistance and fetomaternal safety.
Introduction
Pregnant women are at increased risk of urinary tract infections (UTIs) owing to physiological changes. Infections can cause pregnancy complications and may be transmissible to the fetus. 1 UTIs are the most common type of infection during pregnancy, affecting up to 10% of pregnant women, and all UTIs during pregnancy, including asymptomatic infections, require treatment. 2 Asymptomatic or symptomatic bacteriuria occurs in 5% to 10% and 1% to 3% of pregnant women, respectively. 3 Screening for and treatment of asymptomatic bacteriuria in pregnancy is standard obstetric care, and most antenatal guidelines include routine screening for asymptomatic bacteriuria. 4 Antimicrobial resistance represents a major global challenge that is largely attributed to widespread misuse and overuse of antimicrobials by physicians or by other health care workers in some countries and self-medication practices among individual patients to treat infections.1,2 The identification of frequently isolated pathogens in UTIs among pregnant women and antimicrobial susceptibility patterns of such microorganisms will help in guiding physicians with selecting the appropriate antimicrobial therapy, which will improve management outcomes and will help in reducing the emergence of resistant microbial strains.5–7 The presence of asymptomatic bacteriuria and antibiotic susceptibility testing results should be taken into consideration during the management of pregnant women who are visiting an antenatal care clinic. 8
Although infection with uropathogens among pregnant women is a common medical problem, there is a little information on these microorganisms in pregnancy, and very little is known about their antimicrobial susceptibility patterns. Investigation of this issue is needed, to identify the etiologic agents involved for subsequent treatment with the proper antimicrobial agent.
In this study, we aimed to determine the most frequent UTI pathogens and their antimicrobial susceptibility among pregnant women who attended Jordan University Hospital (JUH) from 2014 to 2018. The results will help guide the management of UTIs in pregnancy.
Methods
Study design
In this retrospective study, we collected urine culture and sensitivity results for pregnant women who were seen at JUH from 2014 to 2018. The pregnancy status of patients was confirmed in urine or blood pregnancy testing and ultrasound scan examination. Urine cultures were requested on the clinical grounds of suspected UTI, with symptoms of frequency, urgency, incontinence, suprapubic pain, low back pain, renal angle tenderness, fever, chills or rigors or in patients with asymptomatic bacteriuria in routine urinalysis as evidenced by white blood cell count more than 10 to 12/high power field.
This study was approved by the institutional review board at JUH (decision number 112/2019, dated 14 May 2019). The requirement for informed consent was waived as the study was retrospective and data were collected using patients' files, and confidentiality and anonymity were maintained throughout the study process.
Study sample collection
The microbiological and antimicrobial susceptibility data in this study were obtained from records of the clinical microbiology laboratory and JUH electronic databases. Data from 2014 to 2018 were extracted using a data extraction sheet. The clinical microbiology laboratory of JOH uses a predefined procedure for culturing, bacterial identification, and susceptibility testing.
Urine sample collection, primary inoculation, and analysis
About 10 mL of mid-stream urine was collected by pregnant women, after appropriate instruction was given. Urine samples were delivered immediately to the microbiological laboratory. Women were given specific instructions to avoid contamination and avoid using of any kind of antiseptics on the vulva, vagina, and urethral orifice. Only mid-stream samples were taken.
Urine samples were cultured on 5% blood agar and MacConkey agar using calibrated loops in semi-quantitative assessment and incubated in aerobic conditions at 35 to 37°C for 18 to 24 hours. Isolates were identified and confirmed using standard methods including Gram staining; colony morphology on media; growth on selective media; lactose and mannitol fermentation; hydrogen sulfide production; catalase, oxidase, coagulase, and indole tests; citrate utilization; and urease testing. Urine infection cultures were considered positive with bacterial counts ≥105/mL. All patients with positive urine cultures were treated.
Antimicrobial susceptibility testing
For reliable detection, laboratories may use conventional, quantitative susceptibility testing methods or specially developed, single concentration agar screening tests for some resistant species, as previously described. 9 The antibiotic discs consisted of antibiotics, according to the type of bacteria; for gram-positive bacteria, the antimicrobials listed in Table 1 were tested; for gram-negative bacteria, antimicrobials listed in Table 2 were tested.
Antimicrobials for gram-positive bacteria.

*Provided as single discs.
Antimicrobials for gram-negative bacteria.

*Provided as single discs.
Antimicrobial susceptibility testing for UTIs in the laboratory is performed using two groups of antimicrobial discs for cascade reporting, a strategy recommended by the Clinical and Laboratory Standards Institute. In this strategy, the reporting of antimicrobial susceptibility test results for the second group of agents (e.g., broader-spectrum, more costly) may only be reported if an organism is resistant to primary agents within a particular drug class. If a pathogen shows resistance to all of these, the laboratory will move to the second stage for testing broad-spectrum antibiotics.
Identification and sensitivity testing were done if the culture was pure and growth was significant (≥105 CFU/mL). If the culture growth involved a mix of two pathogens and no isolate was dominant, or more than two types of colonies were grown, then it was reported as a mixed growth and clinical correlation was needed to make a determination. In such cases, no sensitivity testing was carried out.
Statistical analysis
Data were analyzed using IBM SPSS software version 22 (IBM Corp., Armonk, NY, USA). Chi-square or Fisher’s exact tests were used to identify any significant association between the most frequent pathogens and their antimicrobial susceptibility in pregnant women.
Results
A total of 612 urine samples from pregnant women with suspected UTI were selected for isolation and identification of bacteria and antimicrobial susceptibility testing. Among these, 11 patients showed recurrent infections. The mean age of patients who underwent urine testing was 32.3± 6.5 years. Of 559 patients, 29.2% (163/559) were inpatients and 70.8% (396/559) were outpatients (Table 3).
Demographic profile of the study population.
SD, standard deviation.
The most frequently identified microorganism identified was Escherichia coli (29.4%) followed by coagulase-negative staphylococci (CoNS; 21.7%); Candida was identified in 48 samples (7.8%) (Table 4).
Number and percentage of microorganisms isolated from pregnant urine samples between 2014 and 2018.

CoNS, coagulase-negative staphylococci.
All isolate were sensitive to aztreonam, chloramphenicol, fosfomycin, ofloxacin, pefloxacin, piperacillin, and colistin sulphate; 87.5% were sensitive to amikacin. Only 15.79%, 18.93%, and 17.91% of cultures were sensitive to oxacillin, nalidixic acid, and erythromycin, respectively (Table 5).
Overall sensitivity of antimicrobial agents.

More than three-quarters (76.65%) of isolates were sensitive to nitrofurantoin (Table 5). Regarding E. coli, most cultures were sensitive to meropenem, ertapenem, imipenem, piperacillin/tazobactam, and cefoxitin. However, approximately two-thirds were resistant to nalidixic acid and ampicillin. All Klebsiella cultures were sensitive to amikacin, ertapenem, and imipenem. Nearly half of Klebsiella isolates were sensitive to different cephalosporins whereas only 20.9% were sensitive to nitrofurantoin. Enterobacter species showed 100% sensitivity to amikacin, ciprofloxacin, co-trimoxazole, ertapenem, and imipenem. These cultures were most resistant to augmentin, cefoxitin, and cefuroxime (Table 6).
Antimicrobial sensitivity in gram-negative bacterial isolates.

S, sensitive; R, resistant; I, intermediate.
All Proteus species were sensitive to most tested antibiotics. Nevertheless, these cultures showed high resistance of nearly 100% to ceftriaxone and tetracycline (Table 6).
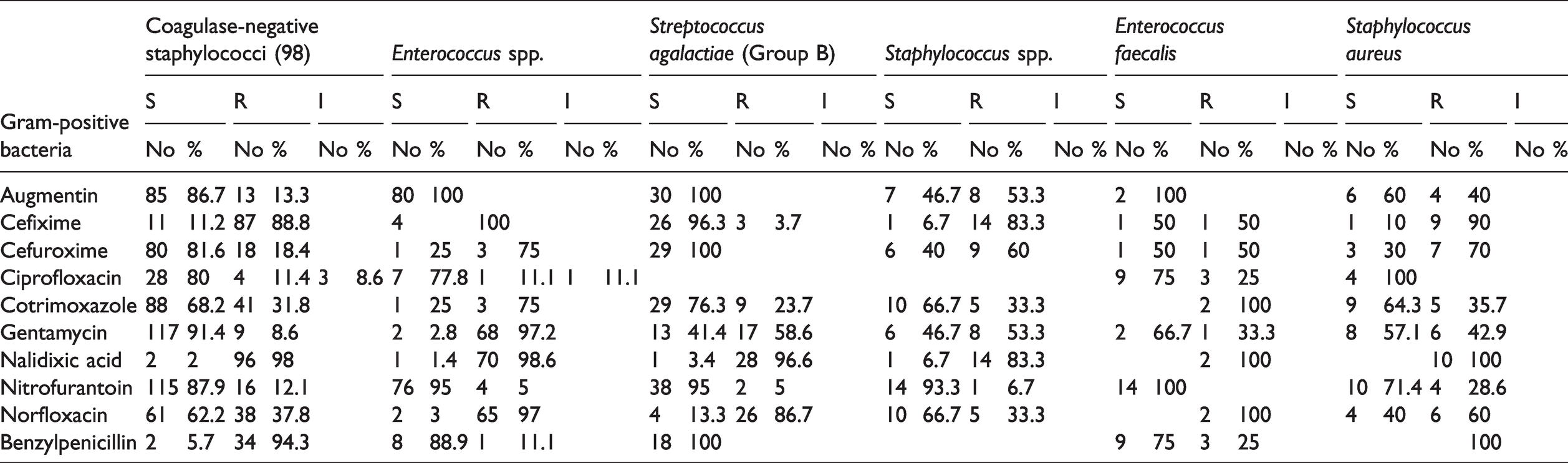
All Acinetobacter species showed resistance to augmentin, cefepime, cefixime, cefuroxime, nalidixic acid, nitrofurantoin, and norfloxacin. These microorganisms were sensitive to colistin sulphate. Of these species, 75% were sensitive to co-trimoxazole and gentamycin (Table 5). All CoNS isolates were sensitive to tigecycline, vancomycin, ampicillin, and linezolid, and most were sensitive to quinupristin (93.3%), gentamicin (91.4%), and augmentin (86.7%). These microorganisms were less sensitive to cefixime, nalidixic acid, benzylpenicillin, and oxacillin, compared with other antibiotics (Table 7). Staphylococcus aureus isolates were 100% sensitive to ciprofloxacin, levofloxacin, linezolid, moxifloxacin, tigecycline, vancomycin, and quinupristin. Enterococcus species were sensitive to augmentin, cefixime, nitrofurantoin, linezolid, oxacillin, tetracycline, and vancomycin (Table 7); all were resistant to nalidixic acid, benzylpenicillin, and oxacillin. All Enterococcus faecalis cultures were sensitive to augmentin, nitrofurantoin, linezolid, tigecycline, vancomycin, and ampicillin, but all isolates were resistant to cotrimoxazole, nalidixic acid, norfloxacin, tetracycline, and quinupristin (Table 7). Most Streptococcus agalactiae (Group B) isolates were sensitive to augmentin, cefixime, cefuroxime, nitrofurantoin, benzylpenicillin, levofloxacin, linezolid, moxifloxacin, tigecycline, vancomycin, ampicillin, and quinupristin (Table 7). All Candida isolates were sensitive to micafungin and voriconazole, and most were sensitive to amphotericin B, fluconazole, flucytosine, and caspofungin (Table 8).
Antimicrobial sensitivity in gram-positive bacterial isolates.
Anti-fungal sensitivity and resistance patterns.

S, sensitive; R, resistant; I, intermediate.
A history of antibiotic therapy was the only variable that remained an independent factor for the occurrence of multi-drug resistant bacterial infection among pregnant women (odds ratio [OR] 5.461, 95% confidence interval [CI] 1.622–17.578; p < 0.05) (Table 9).
Multi-drug resistance among pregnant women.

* p-value < 0.05.
COR, crude odds ratio; AOR, adjusted odds ratio; CI, confidence interval; MDR, multi-drug resistant; UTI, urinary tract infection.
Discussion
Pregnant women are at increased risk of developing UTI, mainly because of a shift in the position of the urinary tract and hormonal changes throughout pregnancy, making it easier for bacteria to reach the kidney and leading to both symptomatic and asymptomatic bacteriuria. UTIs can adversely affect both the woman and her fetus, without timely intervention.1–3 Initial screening and antimicrobial treatment are the preferred interventions. The findings of this study showed that E. coli was the most commonly identified pathogen, which was in line with the findings of previous studies, such as that by Tandan et al. 10 in which E. coli was found to be the commonest UTI-causing organism. In addition, Gessese et al. 5 found that E. coli was the most frequently identified pathogen in 46.4% of study participants with mean age 25 years. Those authors also identified S. aureus in 14.3% of participants, CoNS in 14.3%, and Proteus in 10.6%. Souza et al. 11 found that E. coli and S. aureus were the most commonly identified species, and 89% of isolates were sensitive to fosfomycin. All cultures in this study were sensitive to fosfomycin. Assefa et al. 12 also found high susceptibility to amoxicillin/clavulanic acid (70%), chloramphenicol (83.3%), gentamicin (93.3%), kanamycin (93.3%), nitrofurantoin (87.7%), and co-trimoxazole (73.3%).
Regarding E. coli susceptibility and resistance, Kibret et al. 13 found results similar to the findings of this study. Those authors identified high resistance rates to amoxicillin (86.0%) and tetracycline (72.6%) and a high degree of sensitivity to nitrofurantoin (96.4%), gentamicin (90.6%), and ciprofloxacin (79.6%). Most E. coli isolates in this study were susceptible to norfloxacin, which is relatively safe for use in pregnancy and breastfeeding.14–18 E. coli is considered to be the predominant uropathogenic bacteria because of a number of virulence factors related to invasion and colonization of the urinary epithelium. E. coli is also related to ascent from periurethral regions contaminated by fecal flora because of the close proximity of the perianal area. Chloramphenicol, tetracyclines, and cotrimoxazole should be avoided in pregnancy. 19 However, during early pregnancy chloramphenicol treatment presents little, if any, teratogenic risk to the fetus in humans. 20
Regarding use of nitrofurantoin in pregnancy, there is no increased risk for cardiovascular malformations, oral cleft, or craniosynostosis but the risk of hypoplastic left heart syndrome has been demonstrated (OR 3.07, 95% CI 1.59–5.93). 20 Muanda et al. 21 found that exposure in utero to clindamycin, doxycycline, quinolones, macrolides, and phenoxymethylpenicillin was linked to organ-specific malformations whereas exposure to amoxicillin, cephalosporins, and nitrofurantoin was not associated with major congenital malformations. Bookstaver et al. 22 concluded that beta-lactams, vancomycin, nitrofurantoin, metronidazole, clindamycin, and fosfomycin were generally considered safe and effective in pregnancy whereas fluoroquinolones and tetracyclines should generally be avoided in pregnancy. Among gram-positive bacteria, CoNS showed higher resistance rates to ciprofloxacin, norfloxacin, kanamycin, gentamicin, nitrofurantoin, erythromycin, and amoxicillin/clavulanic acid. The resistance to nitrofurantoin of gram-positive and gram-negative bacteria was comparatively low in this study. The reason might be owing to less frequent use of nitrofurantoin in the study area. In the present study, gram-negative Enterobacter species showed significant resistance to cefuroxime, cefoxitin, and cefalotin. This finding indicates that the recognized practice of oral empirical treatment with these agents should be abandoned. Emerging resistant Enterobacter species have also been identified in other studies.23–26
Napier et al. 27 identified colistin-heteroresistant Enterobacter cloacae in the United States. In the present study, all bacterial isolates were sensitive to colistin sulphate. Ceftazidime–avibactam, colistin, polymyxin B, fosfomycin, aztreonam, aminoglycosides, and tigecycline are treatment options for UTIs caused by carbapenem-resistant Enterobacteriaceae. 28
Contrary to Enterobacter, Proteus species were very sensitive to most cephalosporins, except ceftriaxone. Resistance to tetracycline is of little importance in our study as this antibiotic is contraindicated in pregnancy. For better management, detection of extended-spectrum beta-lactamases (ESBL) should be conducted routinely for Proteus isolates and the genotype surveyed periodically. 29 A high prevalence of ESBL and AmpC β-lactamases has been found in Proteus infections. 30 Phenotypic methods could be implemented in routine diagnostic laboratories along with susceptibility testing, to help in the control of infections. 31 The low resistance levels observed in the present study might be associated with the relative inaccessibility and high prices of these drugs compared with other antimicrobials. Thus, these drugs can be used as adjunct medications in the management of UTIs.
The second most common uropathogen identified in our study was Staphylococcus species. The findings of the antimicrobial resistance profile are supported by the findings of numerous previous studies5,10 showing that Staphylococcus species are highly resistant gram-negative bacteria. In addition, most isolated gram-negative bacteria are sensitive to gentamicin, ceftazidime, and ciprofloxacin whereas these bacteria are resistant to ampicillin, chloramphenicol, and amoxycillin.32,33
CoNS are sensitive to a wide range of antimicrobials but are resistant to benzylpenicillin and oxacillin. Taponen et al. 34 found that penicillin resistance was the most common type of antimicrobial resistance in CoNS, and Staphylococcus epidermidis was the most resistant among the four major species. Those authors also found that phenotypic oxacillin resistance was found in all four main species. CoNS are challenging owing to the large proportion of methicillin-resistant strains and increasing number of isolates with less susceptibility to glycopeptides. 35 Our study findings indicated high sensitivity of CoNS to gentamicin, vancomycin, and linezolid, which was in agreement with the findings of Cui et al. 36 The virulent nature of this infection justifies the use of such agents in pregnancy.
Enterococcus species were susceptible to augmentin, nitrofurantoin, linezolid, tigecycline, vancomycin, and ampicillin. According to Fallah et al., 37 linezolid, chloramphenicol, and nitrofurantoin are the most effective agents against Enterococcus species. All E. faecalis cultures were sensitive to a wide range of antimicrobials; they were all resistant to cotrimoxazole, nalidixic acid, norfloxacin, tetracycline, and quinupristin. Hussain et al. 38 found that 90.09% of E. faecalis strains exhibited resistance to gentamicin, 86.95% to norfloxacin, and 85.71% exhibited multi-drug resistance. Among the urine cultures tested, 7.8% were Streptococcus agalactiae (Group B), and recto–vaginal swab samples showed a 25.5% carriage rate in the third trimester, as reported by Slotved et al. 39
Most Streptococcus agalactiae (Group B) cultures were sensitive to a wide range of antibiotics including augmentin, cefuroxime, and benzylpenicillin. Among 481 recto–vaginal cultures from pregnant women in a study by Shore et al., 40 all were sensitive to penicillin and 19% were resistant to clindamycin. The rate of recurrent infection in this study was 1.8%. In a national sample of non-pregnant women in the United States with uncomplicated UTI, the overall incidence of recurrence was 102/100,000 women. 41
Candida accounted for only 7.8% of all infections in this study. Candida showed sensitivity to most antifungals tested. Pregnancy is a risk factor for UTIs owing to Candida species. 42 Pregnant women are mainly treated with fluconazole and amphotericin B deoxycholate because other drugs have extremely low concentrations in urine. 43
There are some limitations to this study. Routine screening and treatment are still a matter of debate and depend on the prevalence of pathogens. Antimicrobial treatment has not yet shown any benefit for the outcomes of pregnancy,44,45 and overtreatment with antibiotics should be prevented owing to the development of resistance. Our choice of the study period of 2014 to 2018 was owing to JUH having begun using an electronic database in 2014. Additionally, this study was only conducted in one hospital. These may be possible sources of bias in this study. Bacterial resistance is currently at a very high rate, which is often associated with the misuse or inappropriate use of antimicrobial drugs, the absence of stringent drug control and monitoring, and failure to follow standard treatment guidelines.
Conclusion
E. coli and CoNS were the most common microorganisms identified in this study. Empirical therapy with meropenem, ertapenem, imipenem, piperacillin/tazobactam, cefoxitin, tigecycline, vancomycin, ampicillin, amikacin, or linezolid are very appropriate. Most of these antibiotics are relatively safe to be used in pregnancy and breastfeeding. We found increased antibiotic resistance in Enterobacter species. Oxacillin, nalidixic acid, tetracycline, and erythromycin should not be used empirically owing to increased resistance. The choice of antimicrobial therapy in pregnancy should be determined according to sensitivity/resistance and fetomaternal safety.