
Abstract
Objective
Critically ill patients with COVID-19 develop acute respiratory distress syndrome characterized by relatively well-preserved pulmonary compliance but severe hypoxemia. The challenge in managing such patients lies in optimizing oxygenation, which can be achieved through either high oxygen flow or noninvasive mechanical ventilation. This study was performed to compare the efficiency of two methods of noninvasive oxygen therapy: continuous positive airway pressure (CPAP) and high-flow nasal oxygen therapy (HFNO).
Methods
This retrospective cohort study involved 668 patients hospitalized in the intensive care unit (ICU) of the “Sf. Apostol Andrei” Emergency Clinical Hospital, Galati, Romania from 1 April 2020 to 31 March 2021 (CPAP, n = 108; HFNO, n = 108).
Results
Mortality was significantly lower in the CPAP and HFNO groups than in the group of patients who underwent intubation and mechanical ventilation after ICU admission. Mortality in the ICU was not significantly different between the CPAP and HFNO groups.
Conclusions
HFNO and CPAP represent efficient alternative therapies for patients with severe COVID-19 whose respiratory treatment has failed. Studies involving larger groups of patients are necessary to establish a personalized, more complex management modality for critically ill patients with COVID-19.
Keywords
Introduction
The global impact of the COVID-19 pandemic, caused by SARS-CoV-2, has affected health systems worldwide with a novel pathology resulting in very high morbidity and mortality (on 5 April 2023, there were 762,201,169 confirmed cases and 6,889,743 confirmed deaths). 1 Specific features of COVID-19 pneumonia have been observed since the beginning of the pandemic, with an extremely high infection rate and various transmission modalities.2–4 The clinical features are highly variable, ranging from asymptomatic infection to severe respiratory failure with a poor prognosis.3,5,6 Most critically ill patients with SARS-CoV-2 pneumonia develop an atypical form of acute respiratory distress syndrome (ARDS) characterized by relatively well-preserved pulmonary compliance but severe hypoxemia. 7 This type of ARDS is caused primarily by the direct effects of the virus and secondarily by the substances released by host cells. Excessive production of inflammatory cytokines, such as interleukin-6 and tumor necrosis factor-α, plays a key role because these cytokines can lead to ARDS aggravation and extended tissue damage with potential progression to multiple organ dysfunction and death.8–11 Approximately 15% to 30% of patients with COVID-19 develop hypoxemia and progression to acute respiratory failure, and 5% require intensive care unit (ICU) admission for specific respiratory management and provision of oxygen.12,13 The severity and mortality of the disease is dependent on the viral subtype. As of 2023, six subtypes had been identified: Alpha (B.1.1.7, December 2020), Beta (B.1.351, December 2020), Gamma (P.1, January 2021), Delta (B.1.617.2, December 2020), and Omicron (BA.1 and BA.5, November 2021).14,15 The Alpha, Beta, and Gamma variants of SARS-CoV-2 proved to be highly competitive because of mutations that allowed immune system escape, whereas the Delta variant was found to be more transmissible. Omicron, however, showed even higher transmissibility and greater immune escape than Delta. 15 The Omicron variants (BA.2 and BA.5) produce less severe disease than the Alpha and Delta variants. 16
Conventional oxygen therapy is insufficient for most patients with COVID-19 in the ICU. Although the prognosis of patients with pneumonia of other etiologies improves by initiation of invasive mechanical ventilation, the mortality rate is extremely high among intubated patients with COVID-19. 12 Optimal oxygenation, either by high-flow oxygen or noninvasive mechanical ventilation, represents a challenge in treating critically ill patients with COVID-19 in the ICU. Thus, there is a great need to develop strategies for noninvasive oxygenation by which survival can be increased.17,18 High-flow nasal oxygen therapy (HFNO) may more effectively reduce the intubation rate compared with conventional oxygen therapy, but the benefits of its use are controversial.19–21 HFNO is a relatively new technique used in the management of severe respiratory failure. It is also a type of ventilatory support that provides, by means of a nasal cannula, previously heated and humidified oxygen at 60- to 100-L flow and a concentration of up to 100%. 22 Noninvasive ventilation (NIV) is a mechanical ventilatory support technique that utilizes interfaces other than an orotracheal tube, such as a nasal, oronasal, or integral mask or a helmet. 23 HFNO and NIV are the main methods used for management of hypoxemic acute respiratory failure, and many clinical studies have shown that they are associated with good results in patients with COVID-19, lowering the need for invasive mechanical ventilation and the mortality rates.24–26 However, a 2022 study showed that NIV was associated with higher mortality and intubation rates compared with HFNO and continuous positive airway pressure (CPAP). 27
A meta-analysis of 58 studies concluded that there is no consensus regarding the use of noninvasive respiratory support and that the information about the indications for initiation or suppression of these therapies is unclear. 19
Because of the lack of consensus regarding ventilatory support in patients with severe forms of COVID-19, the aim of the current study was to comparatively analyze the results of two oxygenation methods used in patients treated in the ICU of the “Sfantul Apostol Andrei” Emergency Clinical Hospital of Galati, Romania: CPAP and HFNO.
Methods
This retrospective comparative cohort study involved 668 consecutive adult patients with COVID-19 who were admitted to the ICU of the “Sfantul Apostol Andrei” Emergency Clinical Hospital of Galati, Romania from 1 April 2020 to 31 March 2021. We analyzed two groups of patients: those treated with CPAP (n = 108) and those treated with HFNO (n = 108) (Figure 1). The inclusion criteria were severe disease (usually developing 1 week after symptom onset, clinically and radiologically manifesting as pneumonia, and usually complicated by respiratory failure or other complications such as thromboembolism, circulatory shock, encephalopathy, myocardial damage, or arrhythmia 28 ), age of >18 years, and ability to grant consent. Both male and female patients were enrolled. The patients in both groups had acute respiratory failure associated with SARS-CoV-2 infection, hypoxemia (SpO2 < 90% under standard oxygen therapy), and moderately or severely increased respiratory effort.

Patient group selection. ICU, intensive care unit; CPAP, continuous positive airway pressure; HFNO, high-flow nasal oxygen therapy.
The HFNO selection criteria were as follows:
Patient refusal to undergo CPAP, generated mainly by anxiety associated with the method and claustrophobia Higher tolerance for HFNO than CPAP Pre-existing lung disease predisposing to the occurrence of pneumothorax/pneumomediastinum (i.e., pathologies associated with pulmonary emphysema, bronchopulmonary neoplasm, sequelae of pulmonary tuberculosis, or bronchial asthma) Limited number of ventilators required for CPAP
The CPAP selection criteria were as follows:
Low degree of anxiety and high tolerance for CPAP Absence of pre-existing pathologies predisposing to the occurrence of pneumothorax/pneumomediastinum during the use of positive-pressure mechanical ventilation
Patients in both groups required frequent small doses of sedation to decrease their level of anxiety without affecting their state of consciousness. The patients in the HFNO group adopted the prone position for 10 to 16 hours per day.
The criteria for invasive oxygen therapy were an altered state of consciousness, severely increased respiratory effort requiring use of accessory muscles or a respiratory rate of >30 breaths/minute, risk of aspiration pneumonia, and severely decompensated acidosis (pH < 7.2–7.25). Orotracheal intubation was required shortly before death for select patients (considering that orotracheal intubation is also required during resuscitation maneuvers).
The study exclusion criteria were an inability to provide written informed consent for study participation and administration of ventilation, refusal to participate in the study, pregnancy and lactation, and outliers (patients with extreme results of routine laboratory tests, including the erythrocyte sedimentation rate and concentrations of procalcitonin, fibrinogen, ferritin, and C-reactive protein). Patients who had recently undergone surgical procedures or had other non-respiratory conditions that required intensive care were also excluded.
We considered the following exclusion criteria for both groups:
Patients with indications for orotracheal intubation since presentation to the ICU Patients admitted to the ICU who required any combination of the following therapies: conventional oxygen therapy, CPAP, HFNO, or initial orotracheal intubation followed by any of the three above-mentioned therapies
Concerning the initial choice of CPAP or HFNO for patients admitted to the ICU, because of the small number of ICU beds allocated to COVID-19 in our region, we could not include age, sex, or comorbidities as criteria. The therapy was therefore chosen on the basis of the availability of a bed equipped with CPAP or HFNO and the criteria mentioned above.
The patients were monitored during hospitalization in the ICU. Notably, complete data were not available for all patients. The endpoint of the study was the total number of deaths in the ICU. Failure of CPAP and HFNO contributed to ICU mortality because patients transferred from the ICU to the medical ward required neither orotracheal intubation nor invasive ventilation. Patients who died in the ICU were either those whose condition worsened because of respiratory failure under HFNO or CPAP, necessitating invasive ventilation for several days, or those who required intubation during cardiorespiratory resuscitation.
This study was conducted according to the guidelines of the Declaration of Helsinki (following the STROBE guidelines) 29 and approved by the Ethics Committee of “Sfantul Apostol Andrei” Emergency Clinical Hospital of Galati (approval number 20924 on 22 September 2021). Written informed consent for publication was obtained from all patients involved in the study.
Patient data extracted from the observation sheets were analyzed using IBM SPSS Statistics for Windows, Version 26.0 (IBM Corp., Armonk, NY, USA). All patient details were de-identified. Gross descriptive statistical parameters were calculated for all variables analyzed. Continuous variables are presented as mean ± standard deviation, and categorical variables are presented as absolute frequency (relative frequency). The test used in the inferential analysis is specified for each variable. We calculated the φ, V, and C coefficients to analyze the correlation of the variables measured at the nominal level. The chi-square test was performed to measure the association between two categorical variables, and Pearson’s coefficient (r) was used for continuous variables. Comparisons were made between the patients in the CPAP and HFNO groups. For all statistical tests, a two-tailed p-value of <0.05 was considered statistically significant.
Results
Of 668 patients admitted to the ICU from 1 April 2020 to 31 March 2021, 355 required orotracheal intubation and mechanical ventilation with no other respiratory support, CPAP, or NIV. Of these 355 patients, only 11.5% survived; thus, the mortality rate was 88.5% in this group. The mortality rate in this group was markedly higher than that in the entire group of patients (of all 668 patients, 252 (37.7%) survived).
A total of 97 patients underwent various oxygenation strategies, including conventional oxygen therapy, combined therapies such as CPAP and HFNO, and interventions involving CPAP/HFNO and invasive ventilation.
We comparatively analyzed the CPAP group (n = 108) and the HFNO group (n = 108) with respect to demographic data, paraclinical status at ICU admission, comorbidities, antiviral and immunosuppressive therapies, and number of deaths (Table 1(a), (b); Table 2).
Baseline characteristics of patients with COVID-19 treated with CPAP versus HFNO.

CPAP, continuous positive airway pressure; HFNO, high-flow nasal oxygen therapy; SD, standard deviation; T − t, Student’s t-test for differences between means; PaO2/FiO2, ratio of arterial partial pressure of oxygen to fraction of inspired oxygen; RALE, Radiographic Assessment of Lung Edema; ESR, erythrocyte sedimentation rate.
Reference ranges: PaO2/FiO2, 400–500; serum lactate, 0.5–2.2 mmol/L; procalcitonin, 0–0.15 ng/mL; ESR, 0–15 mm/hour; C-reactive protein, 0–1 mg/L; fibrinogen, 200–400 mg/dL; ferritin, 0–400 ng/mL; lactate dehydrogenase, 0–4.2 U/L; lymphocytes, 1000–4000/μL.
Boldface italicized p values are statistically significant.
Comparison of categorial variables in patients with COVID-19 treated with CPAP versus HFNO.

CPAP, continuous positive airway pressure; HFNO, high-flow nasal oxygen therapy.
Boldface italicized p value is statistically significant.
The mean age in both groups was >65 years. The mean age in the CPAP group was 68.56 years (range, 37–99 years), and that in the HFNO group was 66.44 years (range, 20–86 years) (Table 1(a)).
Male sex predominated in both groups (Table 2).
The Radiographic Assessment of Lung Edema (RALE) score for pulmonary lesion severity imaging30,31 was slightly higher in the CPAP group (Table 1(a)), but the difference was not statistically significant.
In the CPAP group, the mean ratio of the arterial partial pressure of oxygen (PaO2) to the fraction of inspired oxygen (FiO2) (PaO2/FiO2, also known as the Horowitz index) was 92.56 (range, 44–216), which was significantly lower than that in the HFNO group (109.78; range, 45–305) (p = 0.0093) (Table 1(a)). In both groups, the ratio was close to the threshold of 100 that distinguishes between moderate and severe respiratory failure.
In the initial evaluation of the inflammatory syndrome, statistically significant differences were found for the following parameters: the procalcitonin concentration (p = 0.0296), fibrinogen concentration (p = 0.0009), and erythrocyte sedimentation rate (p = 0.309) (Table 1(a)).
The incidence of comorbidities was not significantly different between the two groups. Among patients with chronic lung disease, the mortality rate was 100% in both the CPAP and HFNO groups. Additionally, mortality was high among patients with neurological, metabolic, renal, and hepatic diseases in the CPAP group and among patients with oncological comorbidities in the HFNO group (Tables 2 and 3).
Outcome characteristics of patients with COVID-19 treated with CPAP versus HFNO.
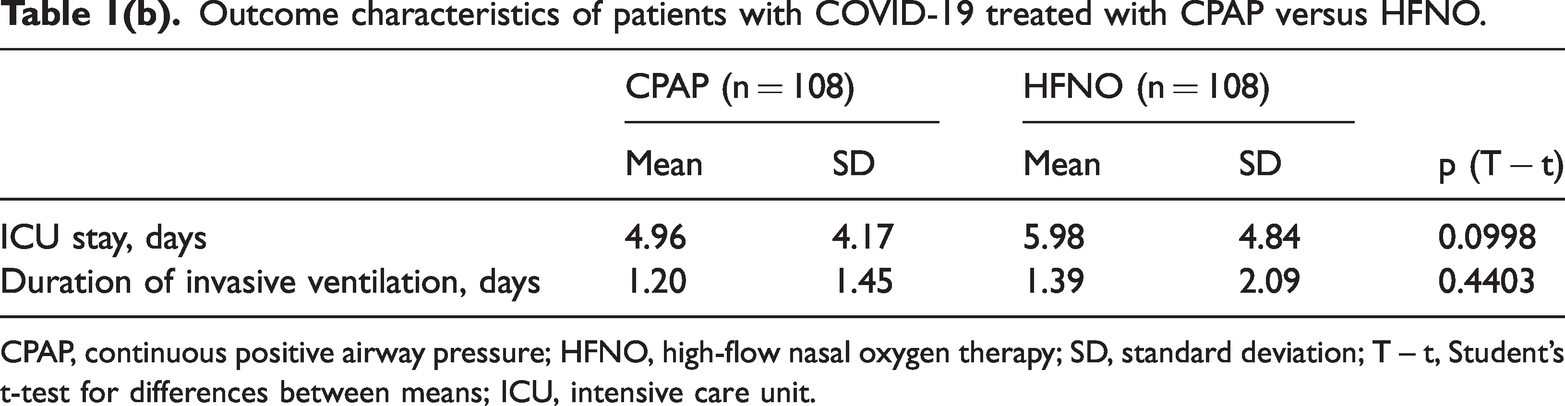
CPAP, continuous positive airway pressure; HFNO, high-flow nasal oxygen therapy; SD, standard deviation; T – t, Student’s t-test for differences between means; ICU, intensive care unit.
Remdesivir and favipiravir were used as antiviral therapy, but the number of patients treated with remdesivir was significantly higher in the HFNO than CPAP group (p = 0.0035). There was no significant difference in immunosuppressive therapy between the two groups (Table 2).
The mean ICU stay was shorter in the CPAP group (4.96 days; range, 1–18 days) than in the HFNO group (5.98 days; range, 1–25 days), but the difference was not statistically significant (Table 1(b)).
Notably, some patients had a very short duration of treatment in the ICU for the following reasons:
A significant number of patients developed sudden clinical worsening that necessitated invasive oxygen therapy, and their condition rapidly progressed toward death thereafter. Patients who showed marked respiratory improvement were transferred relatively quickly to a respiratory recovery service that provided standard oxygen therapy with a flow of up to 30 L/min because of the constant pressure to admit patients to the ICU despite the limited number of beds; additionally, higher numbers of new patients with more severe forms of respiratory failure required admission than patients who had improved statuses.
The mean duration of invasive ventilation after CPAP was 1.20 days (range, 1–11 days), which was shorter than that after HFNO (1.39 days; range, 1–10 days). However, the difference was not statistically significant (Table 1(b)).
The shorter period of artificial ventilation after CPAP than after HFNO can be explained by the fact that some of the patients suddenly died of various COVID-19 complications and required intubation during cardiorespiratory resuscitation maneuvers. Additionally, some patients’ condition worsened under noninvasive oxygen therapy, and their condition did not improve even under intubation and artificial ventilation; these patients died after a few days of intubation. The intubation criteria used in this study were altered consciousness, severely increased respiratory effort with the use of accessory muscles or a respiratory rate of >30 breaths/minute, a risk of aspiration pneumonia, and severely decompensated acidosis (pH < 7.2–7.25). Additionally, at the time of conducting this study, there was no consensus and no sufficient clinical studies establishing clear criteria for stopping noninvasive oxygen therapy and initiating assisted ventilation. Finally, very few intensive therapy beds were allocated for patients with COVID-19 in our geographical region.
Although the mortality rate was slightly higher in the CPAP than HFNO group, the difference was not statistically significant (Table 2). Additionally, there was no statistically significant difference in mortality between the two study groups or between subgroups according to sex, comorbidities, or antiviral and immunosuppressive therapies (Table 3).
Proportions of deaths between CPAP and HFNO groups by sex, comorbidity, and therapy subgroups.

CPAP, continuous positive airway pressure; HFNO, high-flow nasal oxygen therapy.
The mortality rate in both the CPAP group (64.81%) and HFNO group (74.07%) was significantly lower than that in the orotracheal intubation group (88.50%) (p < 0.0001 and p = 0.0004, respectively) (Table 1(b)).
The correlation tests in both groups revealed no significant relationship between mortality and sex, between mortality and comorbidities, or between mortality and antiviral/corticosteroid therapies. In the HFNO group, the correlation tests for the nominal variables revealed a correlation between mortality and remdesivir therapy (χ2 = 4.424, p = 0.038, φ = −286, V = 286 and C = 0.275, p = 0.035) (Tables 4 and 5).
Correlation tests in CPAP group.

CPAP, continuous positive airway pressure.
Correlation tests in HFNT group.
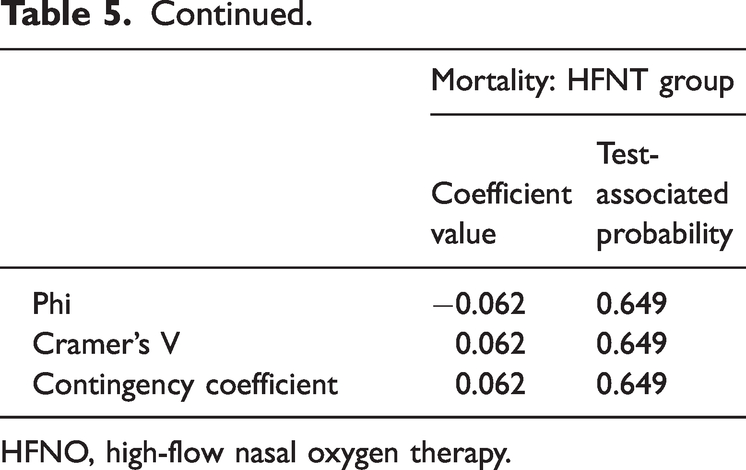
HFNO, high-flow nasal oxygen therapy.
Discussion
The European Respiratory Society recommends using HFNO for patients with acute respiratory failure of various etiologies as follows
32
:
HNFO over conventional oxygen therapy and NIV for hypoxemic acute respiratory failure HFNO over oxygen therapy during breaks from NIV Either HFNO or oxygen therapy in surgical patients with a low risk of developing pulmonary complications Either HFNO or NIV in surgical patients with a high risk of pulmonary complications HFNO over oxygen therapy in nonsurgical patients with a low risk of extubation failure NIV over HFNO for patients with a high risk of developing extubation failure, unless there are relative or absolute contraindications for NIV Testing of NIV efficiency before using HFNO in patients with chronic obstructive pulmonary disease and acute hypercapnic respiratory failure
The European Respiratory Society considers HFNO an effective therapy for acute respiratory failure of various etiologies. 32
For the acute respiratory failure that develops in patients with COVID-19, existing clinical studies are insufficient and there is no consensus regarding the use of various methods of oxygen therapy.
Clinical studies have shown that patients who receive HFNO have better compliance with the administered therapy; specifically, they are able to more efficiently feed themselves and communicate with the medical staff, and they have lower levels of anxiety. By contrast, CPAP is associated with higher levels of anxiety, posing a risk for the development of ventilator dyssynchrony; difficulties in oral nutrition, necessitating additional parenteral nutrition; difficulties maintaining the prone position; discomfort due to cutaneous lesions secondary to mask pressure, which can sometimes overlap with the lesions produced by SARS-CoV-233–35; and other complications of mechanical ventilation such as barotrauma, aspiration pneumonia, and healthcare-associated infection. 36 The prone position improves oxygenation by reducing ventilation/perfusion disorders, decreasing hypoxemia, and slowing the progression of respiratory impairment. However, further studies are needed to prove its long-term efficacy.
In the present study, we noted a lower ICU mortality rate in the HFNO group (64.81%) than in the CPAP group (74.07%), but the difference was not statistically significant. This is consistent with other studies. However, the ICU mortality rate was significantly lower in both of these groups than in the orotracheal intubation group (88.5%).
A meta-analysis of 23 studies involving 5354 patients, published before February 2022, showed lower mortality rates in the HFNO than NIV group (p = 0.0008). 36 The NIV group was divided in two subgroups: one with helmet ventilation and the other with CPAP; however, the mortality rate was not significantly different between the two subgroups. Additionally, the meta-analysis showed no statistically significant differences in the PaO2/FiO2 ratio, total number of hospital or ICU days, and intubation rate between the HFNO and NIV groups. 36
A literature review of patients with COVID-19 revealed that HFNO can decrease the need for intubation, the severity of complications related to mechanical ventilation, and the duration of ICU stay. 37
A clinical study of 1400 patients showed that the 60-day risk of mortality was similar between patients who had received invasive mechanical ventilation since admission and patients those intubated after NIV. 38 These findings suggest that NIV can be used safely in patients with COVID-19-related acute hypoxemic respiratory failure.
It should be noted that the results of some other studies are contradictory. In the randomized COVIDISCUS study, which involved French patients with severe forms of COVID-19, CPAP and HFNO did not significantly change the risk of invasive ventilation at 28 days compared with patients who had received invasive ventilation from the beginning of admission. 39
The SOHO study, which involved 711 French patients with severe forms of COVID-19 from January to December 2021, showed a 10% mortality rate on day 28 in the group treated with HFNO and 11% in the group treated with standard oxygen therapy; however, the difference was not statistically significant. 40
Many factors can influence NIV success, such as the degree of patient cooperation, the type of interface used, the etiology of respiratory failure, and the experience of the medical staff. 23
Two meta-analyses of non-COVID-19 respiratory failure revealed that CPAP can decrease both the need for intubation and the mortality rate compared with simple oxygen therapy.41,42
The RECOVERY-RS Randomized Clinical Trial in the UK, which involved 1273 adults with COVID-19 and respiratory failure, showed a lower 30-day mortality rate and a lower need for intubation in the CPAP group than in the conventional oxygen therapy group. However, there was no significant difference in the initial strategy of HFNO versus conventional oxygen therapy. 43
Acute respiratory failure in patients with COVID-19 may be triggered by many factors, including vaccines, which may exacerbate comorbidities such as psoriasis. When severe COVID-19 is associated with cardiovascular diseases, diabetes, or even systemic sclerosis, patients tend to exhibit higher severity rates and increased mortality.44–47 Consequently, such patients must be treated by a multidisciplinary medical team according to a personalized plan, and the oxygen therapy must include consecutive ventilation strategies adapted to the patient’s specific needs. Further studies are needed to achieve personalized guidelines for these patients.
This study had several limitations. It was an observational study in which no matching or randomization was performed, and it included a relatively small number of patients, preventing us from drawing precise conclusions. Another limitation is the fact that the study population was White; the results cannot be generalized to patients of other races. Additionally, there were some minor differences in the comorbidity profiles at the onset of COVID-19 between the two groups. Finally, the study was quickly set up at the beginning of the pandemic, before the development of a set of basic results for COVID-19 studies regarding the initiation of different types of oxygen therapy, the criteria for ICU and hospital discharge, or patient recovery protocols after treatment of severe COVID-19.
Conclusion
CPAP and HFNO therapies may be an efficient alternative in COVID-19 acute respiratory failure therapy. Mortality in the CPAP and HFNO groups was statistically significantly lower than in the group of intubated and mechanical ventilated patients since the admission in the ICU. Mortality in the ICU of the two groups of patients treated with CPAP and HFNO did not show statistically significant differences.
Mortality in the ICU of the two groups of patients treated with CPAP and HFNO did not show statistically significant differences. The poor prognosis of these patients may be improved by a personalized plan of consecutive ventilation methods.
Supplemental Material
sj-pdf-1-imr-10.1177_03000605231222151 - Supplemental material for Efficiency of continuous positive airway pressure and high-flow nasal oxygen therapy in critically ill patients with COVID-19
Supplemental material, sj-pdf-1-imr-10.1177_03000605231222151 for Efficiency of continuous positive airway pressure and high-flow nasal oxygen therapy in critically ill patients with COVID-19 by Corina Manole, Mihaela Dediu-Anghel, Liliana Baroiu, Ioana Anca Ștefanopol, Alexandru Nechifor, Elena Niculet, Raul Mihailov, Lavinia Alexandra Moroianu, Doina Carina Voinescu and Dorel Firescu in Journal of International Medical Research
Supplemental Material
sj-pdf-2-imr-10.1177_03000605231222151 - Supplemental material for Efficiency of continuous positive airway pressure and high-flow nasal oxygen therapy in critically ill patients with COVID-19
Supplemental material, sj-pdf-2-imr-10.1177_03000605231222151 for Efficiency of continuous positive airway pressure and high-flow nasal oxygen therapy in critically ill patients with COVID-19 by Corina Manole, Mihaela Dediu-Anghel, Liliana Baroiu, Ioana Anca Ștefanopol, Alexandru Nechifor, Elena Niculet, Raul Mihailov, Lavinia Alexandra Moroianu, Doina Carina Voinescu and Dorel Firescu in Journal of International Medical Research
Footnotes
Acknowledgements
We would like to thank the entire team in the intensive care unit who cared for the patients involved in this study with professionalism and dedication.
Author contributions
All authors substantially contributed to the conception or design of the work, drafting the work or revising it critically for important intellectual content, and providing final approval of the version to be published. All authors have agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work is appropriately investigated and resolved. All authors have read and agreed to the published version of the manuscript.
Data availability statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Funding
The article publishing charge was paid by the “Dunarea de Jos” University of Galati, Romania.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.