
Abstract
Objective
To assess the prevalence of needlestick and sharps injuries (NSSIs) and associated factors among healthcare workers (HCWs) at King Hussein Cancer Centre (KHCC), Amman, Jordan.
Methods
This retrospective cross-sectional study undertook a chart review of all HCWs that reported an NSSI between January 2015 and December 2021. Data collected included sociodemographic factors including age, sex, qualifications, and predictors of NSSIs such as working hours, work shift, and specific job roles within the oncology setting, work experience in KHCC, overall work experience and occupational category.
Results
A total of 355 NSSIs were included in this study with a peak prevalence in 2019 (81 of 355; 22.8%). Nurses (220 of 355; 62.0%), housekeeping staff (59of 355; 16.6%) and physicians (45 of 355; 12.7%) were the most affected occupations. NSSIs were most common in the surgical floor (65 of 355; 18.3%) and operating rooms (56 of 355; 15.8%). Blood collection (94 of 355; 26.5%) and waste collection (65 of 355; 18.3%) were the two primary procedures resulting in NSSIs. The risk of injury was significantly associated with the locations of NSSIs, procedure that caused NSSIs, shift and overall experience.
Conclusion
NSSIs remain common among HCWs, which highlights the need for targeted education.
Introduction
Needlestick and sharps injuries (NSSIs) are among the most common occupational hazards that need to be addressed among healthcare workers (HCWs) worldwide; they are one of the most common sources of infection at healthcare facilities. 1 These types of injuries can be described as accidental wounds caused by needles that puncture the skin. Such wounds can occur when people use, disassemble or improperly dispose of needles. Needles can hide in linen or garbage and injure workers who encounter them unexpectedly. 2 The infectious consequences of NSSI exposure in the workplace might cause substantial health problems, ranging from mild to severe anxiety. 3 Human immunodeficiency virus (HIV), hepatitis B virus (HBV) and hepatitis C virus (HCV) are currently among the diseases transmitted by NSSIs. 4 Hundreds of thousands of HCWs are exposed to contaminated needlesticks and sharps each year, putting them at risk for work-related infections such HBV, HCV, and HIV. In addition, the probability of acquiring an HIV infection through NSSIs ranges from 0.2% to 0.5%; and is 3%–10% for HCV and 40% for HBV. 5
According to estimates from the World Health Organization, 3 million people worldwide are exposed to blood pathogens annually; and of these, 2 million healthcare workers/professionals were exposed to HBV, HCV and HIV. 6 More than 90% of these exposures took place in developing nations. 3 The risk of these infections is common in NSSIs, thus safety precautions are expected to be taken by all healthcare workers. The US Centers for Disease Control and Prevention have established standard precautions, which include a multitude of protocols to prevent occupational exposure and handling infectious materials such as blood and other body fluids. These protocols include maintaining proper personal hygiene, using protective barriers, and properly disposing of sharps and other clinical waste. Additionally, the blood borne pathogens standard from the U.S. Occupational Safety and Health Administration mandates that “safety including engineering and work practice controls shall be used to eliminate or minimize employee exposure”, such as the use of sharps with safety-engineered injury protective measures. 3
The prevalence of NSSIs is higher in developing countries compared with developed countries. 7 However, experience from several developing countries demonstrates that implementing national health policy plans consisting of established safety protocols and offering mandatory training programmes to HCWs can successfully reduce the prevalence of NSSIs and associated infection. 8
According to a previous report, the factors associated with NSSI were mostly related to sociodemographic factors (work experience, qualifications, job category), environmental factors (training on infection prevention, long working hours) and other behavioural factors, including recapping needles, use of personal protective equipment and not complying with standard operating procedures. 7
In our opinion, few studies have examined NSSIs in Jordan and most have included only data collected from practicing nurses or nursing students. A previous study concluded that NSSI rates are high among nurses and nursing students; awareness of universal precaution guidelines is low, reporting the occupational exposure to NSSIs is inadequate, and young, female nurses with fewer years of experience are more vulnerable to NSSIs. 9
Studies on the proportion of NSSIs among HCWs and nurses in the oncology sector have not yet been conducted in Jordan. Moreover, there have not been any studies that have examined the practices and predisposing factors associated with NSSIs among affected HCWs in Jordan. Thus, further investigations are needed to understand the causes of the high NSSI rate and low level of knowledge of safety practices and preventive guidelines. 9
The reason for including oncology in a study focusing on NSSIs among HCWs has several rationales: (i) oncology units or hospitals may have specific characteristics and practices that differentiate them from other healthcare settings; (ii) certain healthcare occupations, such as nurses and physicians working in oncology, might face unique risks due to the nature of their work. This distinction can help identify occupations that may require targeted prevention strategies; (iii) the types of medical procedures and interventions performed in oncology units may vary from those in other hospital departments. These differences might influence the likelihood of NSSIs; (iv) findings specific to oncology may lead to the development of specialized protocols or training programmes to mitigate NSSI risks in these settings and by including both general healthcare and oncology, researchers can conduct a comparative analysis to determine if NSSI rates and risk factors differ significantly between the two. This current retrospective cross-sectional study aimed to determine the prevalence of and factors related to NSSIs among different categories of HCWs at King Hussein Cancer Centre (KHCC), Amman, Jordan.
Materials and methods
Study design and setting
This retrospective cross-sectional study was conducted at KHCC, Amman, Jordan, between January 2015 and December 2021. KHCC is the only specialized cancer centre in Jordan and is responsible for treating more than two-thirds of the cancer patients in the Kingdom, in addition to a considerable number of patients from neighbouring Middle Eastern countries. The study enrolled consecutive HCWs who were injured and reported an NSSI between 2015–2021. Participants were selected consecutively from the needlestick and sharp injury reports during the recruitment period (2015–2021). The consecutive sampling method was employed to ensure that all eligible participants who met the inclusion criteria were included in the study. The inclusion criteria were as follows: (i) all HCWs employed at KHCC, Amman, Jordan; (iii) all incidents of NSSI reported by the enrolled HCWs during the specified time period. The exclusion criteria were as follows: (i) injuries sustained by individuals who were not classified as HCWs; (ii) any injuries that were not specifically classified as NSSIs, including injuries resulting from falls, blunt objects or any other mechanisms apart from needlesticks or sharp objects; (iii) NSSIs that occurred outside the study period were excluded from the study.
Prior to conducting any data analysis or reporting, all HCW details were meticulously de-identified to ensure the protection of their privacy and confidentiality. Personal identifiers, such as names, addresses, contact information, medical record numbers and any other potentially identifiable information, were removed or anonymized from the dataset. This de-identification process allows for the presentation of the research findings in an aggregate and anonymous manner, in accordance with ethical guidelines and data protection regulations. This study was approved by the Institutional Review Board Committee of KHCC (no. 21 KHCC 182)). The requirement for informed consent was waived by the Institutional Review Board Committee of KHCC because of the retrospective nature of the study. The authors confirm that all methods were carried out in accordance with the relevant guidelines and regulations. This research was prepared based on the Strengthening the Reporting of Observational studies in Epidemiology (STROBE) checklist for cross-sectional study. 10
Variables
Data collected included sociodemographic factors including age, sex, qualifications, and predictors of NSSIs such as working hours, work shift, and specific job roles within the oncology setting, work experience in KHCC, overall work experience and occupational category. Data for exposure to NSSI included date of exposure, place of injury, procedure/task during which injury occurred and site of injury on the body.
Data sources and measurements
Data were obtained from the employee clinic as they received the needlestick incident reports from the staff, then the data were processed using Microsoft Excel® (Microsoft Corp., Redmond, WA, US). All NSSI report sheets were collected and reviewed, and all data used for analysis were extracted directly from the reports. This stringent documentation process ensured that all incidents were accurately recorded, contributing to the reliability and completeness of the data. The confidentiality of the data was ensured; information was coded to protect the participants’ identities.
Bias
Using a standardized data collection tool to collect information on NSSIs helped to ensure consistency and reduce measurement bias. Training of data collectors in the use of these tools was essential to maintain data quality to avoid bias.
Sample size
The sample size for this cross-sectional prevalence study on NSSIs among HCWs in the oncology setting was determined based on the desired level of precision, estimated prevalence and confidence level. The study aimed to estimate the prevalence of NSSIs with a 95% confidence level and a desired margin of error of ± 5%. Using available literature and preliminary data, the estimated prevalence of NSSIs was approximately 20%. Considering a Z-score of 1.96 for a 95% confidence level, the formula for calculating the required sample size (n) was as follows: n=Z2*p*(1−p)/E2; where: Z = 1.96 (for a 95% confidence level), P = 0.20 (estimated prevalence of needlestick injuries as 20%), and E = 0.05 (desired level of precision as ± 5%). To achieve the desired level of precision, a minimum sample size of 246 participants was calculated.
Statistical analyses
All statistical analyses were performed using IBM SPSS Statistics for Windows, Version 28.0 (IBM Corp., Armonk, NY, USA). Data for NSSIs are presented as frequency and percentage. χ2-test was used to measure the relationship between the needlestick incident and HCW characteristics. All P-values were two-sided. A P-value ≤ 0.05 was considered statistically significant.
Results
This retrospective cross-sectional study analysed 355 HCWs with NSSIs (164 males [46.2%]; 191 females [53.8%]). The majority of these injuries (219 of 355; 61.7%) occurred during the day shift (07:00 h –19:00 h), while 38.3% (136 of 355) of them occurred during the night shift (19:00 h–07:00 h).
From January 2015 to December 2021, the highest rate of NSSIs per was reported in 2019 (81 of 355; 22.82%), whereas the lowest incidence rates were reported in 2015 and 2016 (33 of 355 [9.30%] for each year) (
Prevalence of needlestick and sharps injuries (NSSIs) stratified according to the year in a retrospective cross-sectional study that aimed to determine the prevalence of and factors related to NSSIs among different categories of healthcare workers.


Monthly prevalence of needlestick and sharps injuries (NSSIs) stratified according to the year in a retrospective cross-sectional study that aimed to determine the prevalence of and factors related to NSSIs among different categories of healthcare workers.
In terms of the occupational category of staff, the results showed that nurses were the most frequently affected by NSSIs (220 of 355; 61.97%), followed by housekeeping staff (59 of 355; 16.62%) and physicians (45 of 355; 12.68%) (
Prevalence of needlestick and sharps injuries (NSSIs) stratified according to the occupational category in a retrospective cross-sectional study that aimed to determine the prevalence of and factors related to NSSIs among different categories of healthcare workers.

In terms of the location of the NSSI events, the surgical floor (65 of 355; 18.31%) was the most common place, followed by the operating room (56 of 355; 15.77%), then the emergency room (37 of 355; 10.42%) and intensive care units (33 of 355; 9.30%) (
Prevalence of needlestick and sharps injuries (NSSIs) stratified according to the location in a retrospective cross-sectional study that aimed to determine the prevalence of and factors related to NSSIs among different categories of healthcare workers.

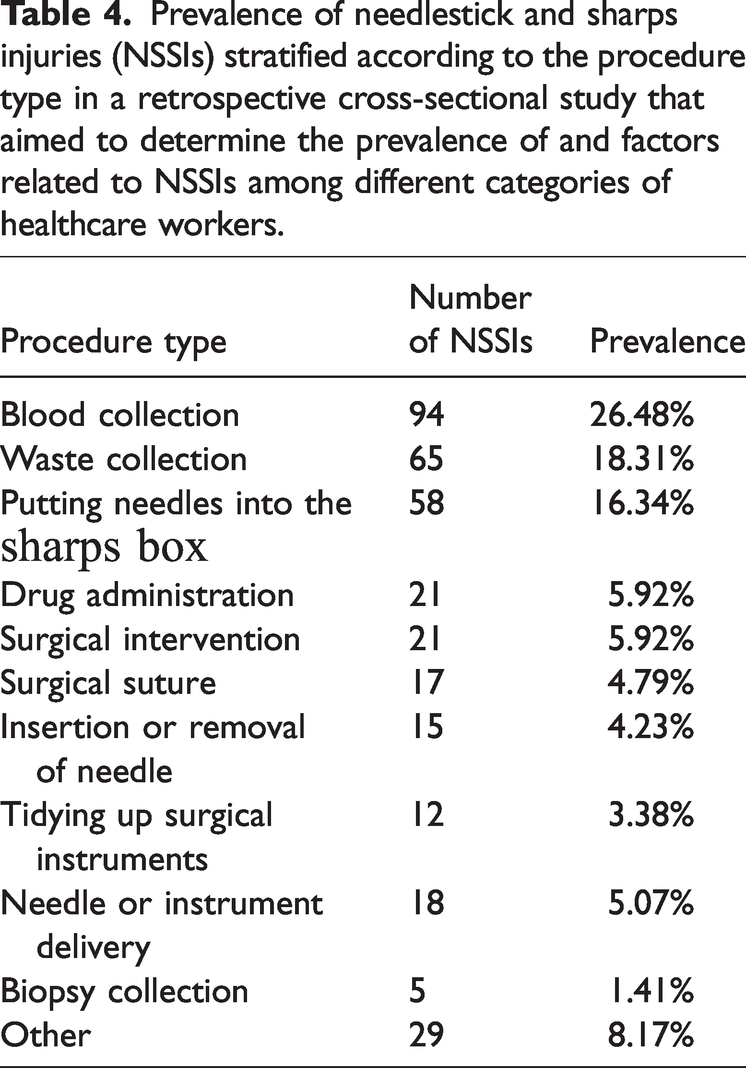
In terms of the type of procedure that resulted in an NSSI, blood collection (94 of 355; 26.48%) was the most common, followed by waste collection (65 of 355; 18.31%) and during the process of putting needles into the sharps box (58 of 355; 16.34%) (
Prevalence of needlestick and sharps injuries (NSSIs) stratified according to the procedure type in a retrospective cross-sectional study that aimed to determine the prevalence of and factors related to NSSIs among different categories of healthcare workers.
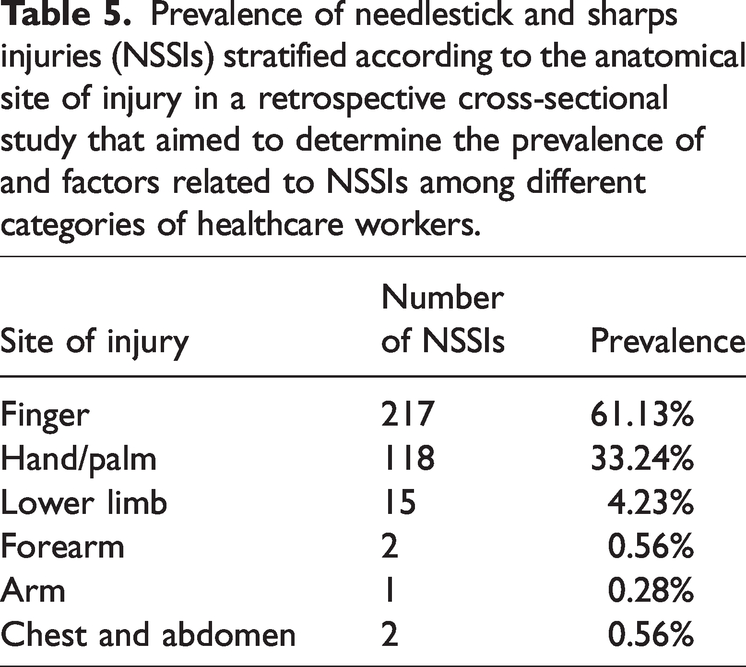
In terms of the anatomical site of the NSSI, fingers (217 of 355; 61.13%) and hand/palm (118 of 355; 33.24%) were the most frequently affected body parts (
Prevalence of needlestick and sharps injuries (NSSIs) stratified according to the anatomical site of injury in a retrospective cross-sectional study that aimed to determine the prevalence of and factors related to NSSIs among different categories of healthcare workers.
Among all HCWs, injuries during the use of the sharp item (191 of 355; 53.80%) and while disposing of the sharps (65 of 355; 18.31%) were the most common (
Prevalence of needlestick and sharps injuries (NSSIs) stratified according to the phase of needle or sharp use in a retrospective cross-sectional study that aimed to determine the prevalence of and factors related to NSSIs among different categories of healthcare workers.

With regard to the work experience at KHCC of the HCWs, the results showed that the majority of the sample (253 of 355; 71.27%) had work experience of < 2 years, followed by those who had work experience of > 5 years (58 of 355; 16.34%); and 44 of 355 (12.39%) had 2–5 years of experience (

Distribution of needlestick and sharps injuries (NSSIs) stratified according to the duration of work experience at the King Hussein Cancer Centre in a retrospective cross-sectional study that aimed to determine the prevalence of and factors related to NSSIs among different categories of healthcare workers. The colour version of this figure is available at: http://imr.sagepub.com.

Distribution of needlestick and sharps injuries (NSSIs) stratified according to the overall duration of work experience in a retrospective cross-sectional study that aimed to determine the prevalence of and factors related to NSSIs among different categories of healthcare workers. The colour version of this figure is available at: http://imr.sagepub.com.
The results of the analysis of the associations between independent variables and NSSIs in HCWs stratified according to their occupational category are presented in
Analysis of the associations between independent variables and needlestick and sharps injuries (NSSIs) stratified according to the occupational category in a retrospective cross-sectional study that aimed to determine the prevalence of and factors related to NSSIs among different categories of healthcare workers.

Data presented as n of participants (%) within occupational category.
χ2-test; NS, no significant association (P > 0.05).
For the year 2019, nurses and housekeepers demonstrated the highest NSSIs, registering at 52 of 220 (23.6%) and 13 of 59 (22.0%), respectively. Among physicians, the highest number of NSSIs, 11 of 45 (24.4%), were reported in 2021.
In terms of the location of the NSSIs, a high proportion in nurses occurred in the surgical floor (54 of 220; 24.5%), while physicians’ injuries mostly occurred in the operating room (28 of 45 ; 62.2%). NSSIs in housekeeping staff were most likely to occur in waste collection areas (15 of 59; 25.4%), with a significant association between occupational category and the locations of NSSIs (P < 0.001).
In terms of the procedure that caused the NSSI, physicians acquired injuries mostly commonly during surgical intervention (15 of 45; 33.3%) and surgical suturing (10 of 45; 22.2%). Nurses were mostly frequently injured during blood collection (87 of 220; 39.5%) and when putting needles into the sharps box (55 of 220; 25.0%). Waste collection was the most common cause of housekeeping injuries (56 of 59; 94.9%), with a significant association between occupational category and the procedure that caused the injury (P < 0.001).
When considering the time of the injuries, the majority of NSSIs in physicians, laboratory technicians and housekeeping staff occurred during the day shift. In contrast, NSSIs incurred by nurses were more evenly distributed between the day and night shifts, with a significant association between occupational category and the shift during which the injury occurred (P < 0.001).
Regarding the overall experience, the highest proportion of NSSIs occurred in physicians with > 5 years of experience (22 of 45; 48.9%). In contrast, NSSIs in nurses and housekeeping staff were predominantly associated with those with < 2 years of experience (139 of 220 [63.2%] and 25 of 59 [42.4%], respectively).
Discussion
The National Institute for Occupational Safety and Health USA has defined needlestick injuries as injuries caused by needles such as hypodermic needles, intravenous stylets and needles used to connect parts of intravenous delivery systems. 11 These events are of concern because of the risk of transmitting blood-borne diseases such as HBV, HCV and HIV. 12 The US Centers for Disease Control estimated that exposure to blood and body fluids from sharps and NSSIs affect around three million health workers annually with an estimated occurrence of six million NSSIs every year, which may lead to approximately 1100 deaths or significant disabilities. 13
The most common cause of occupational exposure to pathogens among HCWs is needlestick injuries. 14 A prospective study of HCWs estimated that the mean risk for transmission after a percutaneous exposure was approximately 6%, 30% and 1.8% for HIV, HBV and HCV, respectively. More than 90% of these infections occur in low-income countries and most could be avoided. 15
This current study's novelty arises from its focus on a specific healthcare context, its longitudinal nature, and its exploration of occupational variations, its detailed analysis of locations and procedures, and its identification of statistically significant associations. By addressing NSSIs in a specialized setting and providing context-specific insights, the study enhances the understanding of injury patterns and offers valuable recommendations for safeguarding the health and safety of HCWs. In this 7-year retrospective study spanning 2015–2021, a total of 355 NSSIs were reported. The highest concentration of NSSIs occurred in 2019 (81 of 355), accounting for 22.82% of all incidents reported during the study period. The injury rates per 100 occupied hospital beds fluctuated between 14.63% and 28.22% over the study duration. Notably, there was a gradual increase to 28.22% from 2015 to 2019, but the rate then declined to 14.63% in 2020. This decline in NSSIs in 2020 may be attributed to changes in behaviour and facility utilization patterns associated with the COVID-19 pandemic.
The proportion of NSSIs among HCWs at KHCC was relatively high in comparison with other countries. For example, it was 4.8–7.6 NSSIs per 100 occupied beds per year in Japan (the number of NSSIs tended to be higher for larger hospital sizes), while it was 10.56 NSSIs per 100 occupied beds per year in Korea.16,17 The rate was 3.2% NSSIs per 100 occupied hospital beds at Ministry of Health hospitals in Saudi Arabia, which may be due to under-reporting of such incidents. 18
In Jordan, there are few studies analysing NSSIs since they are either not well-designed or primarily focus on the nursing profession.9,19–26In this current study, nurses were the most commonly affected occupational group, followed by housekeeping staff and then physicians. This finding was consistent with the fact that among all healthcare personnel providing patient care inside healthcare facilities, nurses are the most susceptible group to suffer from NSSIs. 24 These current results were also consistent with the findings of another study conducted in Amman, Jordan, which showed that the highest NSSIs occurred among nurses (48.7%), followed by housekeepers (33.9%). 25 In another study conducted at the Jordan University Hospital in Jordan from 1993–1995, the highest occurrence of NSSIs was among nurses (34.6%) followed by environmental workers (housekeepers; 19%), 20 which was in agreement with this current study.
It is critically important to recognize that these occupational categories remain the most critical in terms of NSSI prevention programmes. This can be explained by the fact that nurses have the largest staff in any hospital or medical centre, work most of the time in close contact with patients, and are responsible for most blood sampling and other intravenous access procedures that involve a range of injection types. They therefore have much more opportunity for an NSSI than other occupations. 24 In addition, a previous study reported that nurses working in units with low staffing levels, high workloads and poor organization reported twice as many NSSIs as nurses in well-staffed units, implying that adequate staffing is safer for both patients and nurses. 27 In addition to that, rotating shifts may lead to decreased alertness at work. For example, a study conducted in the US showed that nurses who work in rotating shifts had twice the odds of reporting an accident or error related to sleepiness than their colleagues on non-rotating shifts. 28
The current study found that NSSIs were less common among physicians and laboratory technicians compared with nurses and housekeeping staff. This finding was in agreement with a previous Jordanian study that showed that NSSIs were less common among physicians (8.5%) and laboratory technicians (5.1%); and this finding was explained by the fact that nurses were in more contact daily with using needles and sharp instruments than other HCWs. 25
In this current study, most of the reported NSSIs occurred in the surgical floor, operating rooms, emergency rooms and intensive care units, which are the areas that have the most patient contact, high workloads, and high stress levels and have high daily volumes of procedures that require the use of needles and sharp objects. Such procedures are mainly done by nurses, which may explain the significant association between occupational category and locations of NSSIs as well as the association between surgical floor injuries and nurse’s work.
The results of this current study demonstrated that NSSIs occurred most frequently during blood and waste collection and during discarding needles into the sharps box. These current findings were consistent with the finding of another study conducted in Jordan that found that 22.6% of sharps injuries occurred during blood drawing, which was the most common cause of NSSIs. 23
The parts of the body most affected by NSSIs in the current study were the fingers followed by the hand/palm. This may be due the way individuals grasp needles or load/unload scalpels using mainly their hands, which includes the hand-to-hand passage of sharps. Other injuries such as lower limb, chest and abdominal injuries, which were in the minority, might have been due to a lack of separation of sharps from other waste, so HCWs become exposed while carrying garbage bags containing improperly disposed-of sharps close to the body.
Most of the incidents in the current study occurred during the use of sharp items and while disposing of them, which is most likely related to malpractice in handling and disposing of the sharp instruments. This is in agreement with the EPINet Report for Needlestick and Sharp Object Injuries, which states that more than 50% of NSSIs occurred during the use of sharp the item, followed by 13% of incidents occurring after use, before disposal. 29
These current research results indicate that the majority of injuries occurred among individuals with low work experience. These current findings were consistent with previous reports in Jordan and Saudi Arabia, which found that NSSIs were more common in the early years of employment.22,30
The majority of the NSSIs occurred during the day shift (07:00 h –19:00 h) in the current study, which could be related to the higher volume of procedures compared with the evening and night shifts, thus increasing the likelihood of an NSSI. In addition to that, fatigue and alertness at work may contribute to an increase in occupational errors resulting in NSSIs.
Although occupational exposure to NSSIs is considered to be much higher in the developing world, 31 the actual data can be difficult to determine as many cases are thought to be under-reported. Under-reporting of NSSIs is most likely related to poor documentation practices, workload pressure, reluctance to admit mistakes to avoid disciplinary actions and a lack of knowledge. 32 Other reasons may be related to the different levels of awareness of infection control measures and a high rate of staff turnover. Therefore, this problem continues to present a great challenge to infection control and requires further practical steps to be resolved.
This current study had several limitations. First, the retrospective nature of the study design relies on available records and reporting practices, which potentially leads to underreporting or incomplete documentation of NSSIs. Secondly, while efforts were made to ensure the confidentiality of data, the reliance on de-identified records could introduce information gaps or potential inaccuracies in the analysis. Thirdly, the sample size was relatively small. A larger sample size could provide a more robust representation of the different HCW categories, allowing for more nuanced analyses and potentially revealing additional significant associations or patterns. The relatively small sample size might also limit the statistical power to detect less common factors that could contribute to NSSIs. Lastly, the study did not delve into the psychological and emotional impact of NSSIs on HCWs, which could provide valuable insights into the overall well-being of the affected personnel. Despite these limitations, this research provides valuable insights into the prevalence and contextual factors of NSSIs within a specialized healthcare setting, contributing to the broader understanding of HCW safety.
In conclusion , this current study demonstrated the prevalence of NSSIs among HCWs at KHCC in Amman, Jordan. The findings indicate a potential need for comprehensive measures to address the occupational hazards associated with NSSIs and to enhance the safety of healthcare personnel. The study demonstrated that NSSIs were more common in certain work settings and during specific procedures, emphasizing the importance of targeted interventions and training programmes. The association between NSSIs and lower work experience underscores the necessity of tailored educational efforts for newly employed HCWs. With observed relationships between NSSIs and various factors, this study may offer insights for designing evidence-based interventions aimed at minimizing the risk of NSSIs and enhancing workplace safety. The current findings provide a basis for healthcare facilities to consider prioritizing preventive measures, safety protocols and continuous training to potentially reduce the occurrence of NSSIs and enhance the protection of HCWs’ health and well-being.
Footnotes
Acknowledgements
The authors thank all participants and collaborators for their support of this project. Special thanks go to King Hussein Cancer Centre. We are grateful to the Science Health Education Centre and Dana-Farber Cancer Institute for their guidance in editing and review of this manuscript. A special thank you goes to the Editor, Elizabeth Hamlin, for her contribution to the finalization of this manuscript. Finally, the authors would like to thank the reviewers, whose useful and constructive criticism significantly improved the manuscript.
Author contributions
S. Mubarak contributed to study conception and design; R. Abuwardeh was responsible for data collection; K. Ammar contributed to the analysis of the data; S. Mubarak and H. Al Ghawrie contributed to the interpretation of the data, took responsibility for the integrity of the data and the accuracy of the data analysis, and drafted the initial manuscript. All authors have reviewed and approved the final manuscript.
Declaration of conflicting interest
The authors declare that there are no conflicts of interest.
Funding
This research received no specific grant from funding agency in the public, commercial, or not-for-profit sectors. The article write-up and publication fee were supported by King Hussein Cancer Centre.