
Abstract
Macrodystrophia lipomatosa (MDL) is a rare disorder characterized by overgrowth of mesenchymal cells, resulting in gigantism of one or more digit. We report a case of a woman in her late 60s who presented with abnormal enlargement of the right second toe. By debulking the pathological tissue while preserving the shape of the toe as much as possible without amputation of the entire phalanx, debulking surgery not only helps walking, but also allows wearing shoes of the same size on both feet and achieves cosmetic satisfaction for patients. The functional and cosmetic improvement obtained through debulking surgery in this case resulted in no recurrence of disease 5 years postoperatively and provided a desirable alternative to amputation. Therefore, through this case, we demonstrated that debulking surgery can be a reasonable option for MDL patients.
Keywords
Introduction
Macrodystrophia lipomatosa (MDL) is a rare disease usually diagnosed at birth. MDL is characterized by local mesenchymal cell overgrowth, resulting in gigantism of the fingers or toes. 1 The lower extremities are more commonly affected than the upper extremities, with the second and third toes affected most commonly. 2 MDL is of clinical interest because of the cosmetic and mechanical problems related to abnormal gait and possible neurovascular compression due to large osteophytes secondary to degenerative joint disease. Here, we present a case of MDL and its outcomes after debulking surgery.
Case report
The reporting of this study conforms to the CARE guidelines, 3 and written informed consent for treatment and publication of this report was obtained from the patient. A woman in her late 60s presented with abnormal enlargement of the right second toe. Physical examination revealed macrodactyly of the right second toe (Figure 1); hypertrophy of this toe had been present since childhood. The size of the second toe was similar to that of the great toe during adolescence, but progressively increased in size with advancing age. The patient also had hypertension and diabetes as underlying diseases. The patient’s chief complaint was difficulty and pain when walking and wearing footwear. There were no infections or skin abnormalities, and plain radiography revealed soft tissue hypertrophy and osteoarthritis of the second metatarsophalangeal (MTP) joint (Figure 2).

Preoperative dorsal view of the enlarged right second toe.

Radiographs of the feet showing increased soft tissue densities and osseous overgrowth with a mushroom-shaped appearance.
T1- and T2-weighted magnetic resonance imaging (MRI) revealed an increase in the size of the second toe, osteosclerotic findings from the second MTP joint to the distal toe, and an increase in bone size. The increase in soft tissue volume was proportional to the increase in bone volume (Figure 3). A 7- × 5-mm cystic degenerative pituitary microadenoma was observed on brain MRI (Figure 4). However, hormone tests showed no specific findings, and the possibility of acromegaly was low.
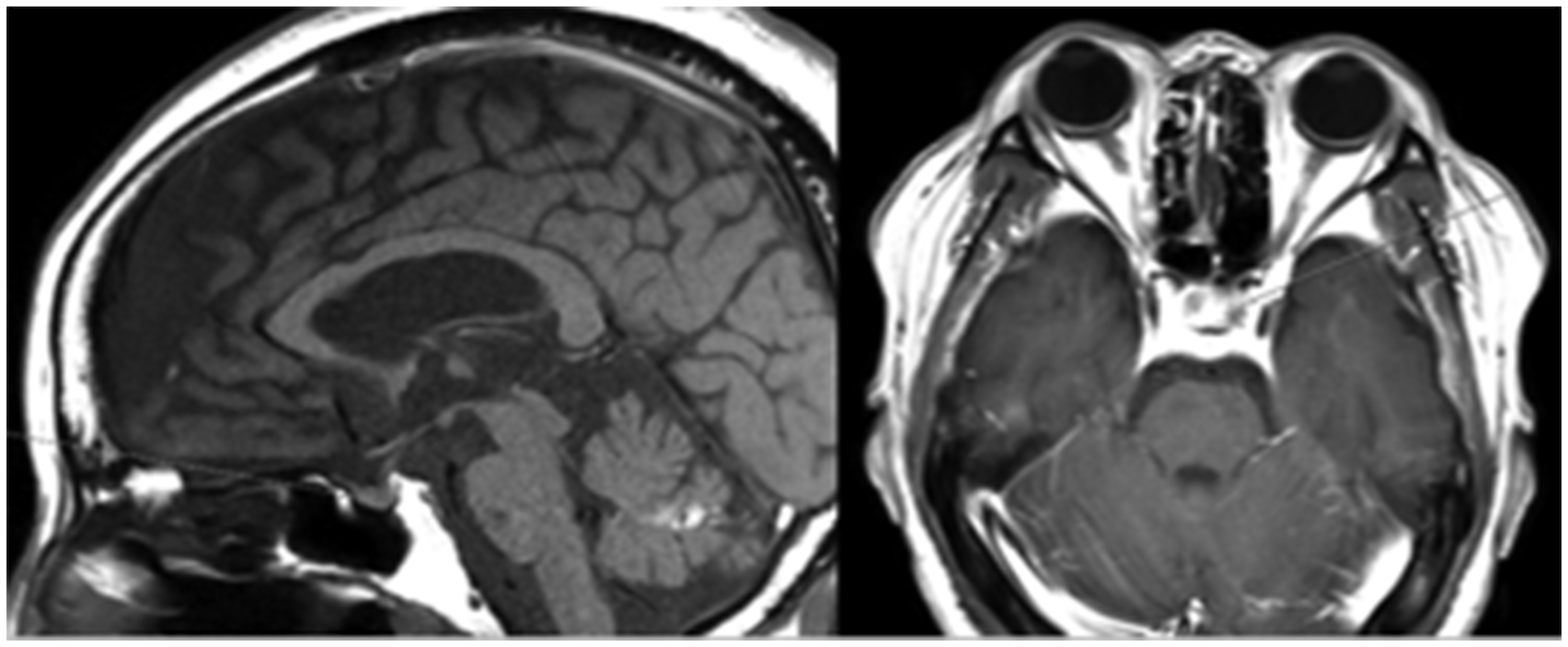
Sagittal (left) and transverse (right) T1-weighted magnetic resonance imaging of the brain showing the presence of a 7 mm × 5-mm cystic degenerative pituitary microadenoma.

Design of the second toe amputation to recreate the toe shape.
Surgery was designed to successively reduce the length, width, height, and overall bulk of the affected toe. Informed consent and agreement with the plan were obtained before surgery. Excess skin and fat were excised as planned preoperatively, followed by amputation of the distal phalanx of the right second toe, with the nail bed (Figure 5). Surgery comprised modest debulking of the dorsal and plantar aspects, with the distal phalangeal amputation. U-shaped incisions were made over the medial and lateral aspects of the toe, and the underlying fibroadipose tissue was excised. The extensor and flexor tendons of the second toe were resected, and the digit was amputated at the distal interphalangeal joint. The skin flap covering the bone was designed and then sutured tension-free after performing resection arthroplasty with a K-wire to correct the alignment of the MTP joint after the debulking surgery (Figure 5).

Surgical procedure showing the U-shaped incisions and flap coverage of the second proximal phalanx to create a toe shape, and plain radiography of the foot after surgery using a K-wire to correct alignment of the MTP joint.
Histological examination of the excised tissue showed the presence of fibroadipose tissue with areas of hyalinosis and basophilic collagen degeneration (Figure 6).

Histology of the excised tissue showing the presence of fibroadipose tissue with areas of hyalinosis and basophilic collagen degeneration (×40, hematoxylin & eosin (H&E) staining).
Six weeks after the surgery, the K-wire was removed, and follow-up revealed that the patient was able to wear the same-sized shoes on the operated and contralateral feet without complications. The patient reported no unusual discomfort, such as sensory abnormalities, while walking. Additionally, during the 5-year follow-up, no recurrence of soft tissue or bone proliferation was noted on physical examination or plain radiography (Figure 7). The clinical scores improved at the last follow-up visit compared with those recorded preoperatively (Table 1).

Photograph and radiographs of the foot at the final follow-up showing no evidence of recurrence.
Clinical scores for the patient preoperatively and at the final follow-up.
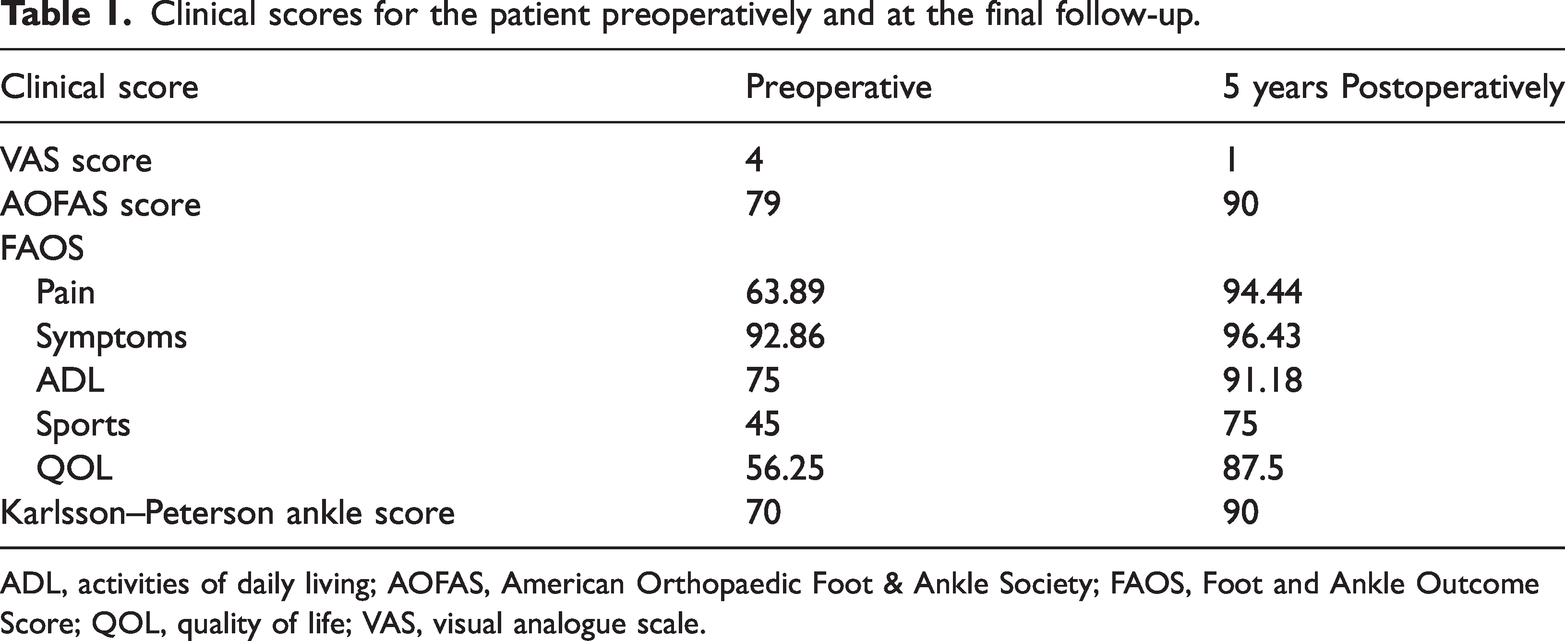
ADL, activities of daily living; AOFAS, American Orthopaedic Foot & Ankle Society; FAOS, Foot and Ankle Outcome Score; QOL, quality of life; VAS, visual analogue scale.
Discussion
Feris et al. first coined the term “macrodystrophia lipomatosa” in 1925, referring to a form of localized giant limb affecting only the lower extremities. 4 In 1960, Golding applied the term to the hands as well. 5 These lesions are not inherited and are reported as congenital hypergrowth of all mesenchymal cells, namely the bone, adipose tissue, tendons, muscles, and nerves of an extremity or digit. 1
Plain radiologic findings, such as mushroom-shaped appearance of the toe, excessive soft and bone tissue growth, and hyperproliferation of unencapsulated fibroadipose tissue on MRI, are pathognomonic signs of MDL.6,7 The differential diagnosis of MDL comprises hemangioma, neurofibroma, intraneural lipoma, Klippel–Trenaunay–Weber syndrome, Proteus syndrome, Ollier disease, and Maffucci syndrome, which can be differentiated by histological findings. 8 In the present case, we diagnosed MDL by confirming overgrowth of adipose tissue, which had a signal intensity similar to that of normal subcutaneous fat, and observing hypertrophy of mushroom-shaped bone tissue.
In 1967, Barsky reviewed the available literature and stated that there were two types of true macrodactyly: static and progressive. 9 The static type (most common) showed enlargement from birth and an increase in size proportional to growth. The progressive form showed disproportionate growth of the affected digit, which increased in size at a rate faster than could be attributed to normal growth patterns. Cosmetic problems with MDL are common in all age groups; however, mechanical problems that cause deterioration of joint function appear as secondary degenerative changes after puberty. Therefore, most static-type patients seek surgical correction for cosmetic reasons. Mechanical problems are not encountered until late childhood or adolescence, when secondary degenerative changes decease joint function. In the present report, unlike most case reports of MDL, the patient experienced a long disease course. Therefore, she experienced both mechanical and cosmetic problems.
Toe overgrowth may cause dorsiflexion of the affected toe, mainly affecting the plantar region. This lesion prevents the toe from providing support against the ground during the stance phase, which is a function of the toe, making normal walking impossible. 10 As a result, abnormal gait could result in toe or foot pain. Additionally, mechanical problems, such as secondary osteoarthritis and dysfunction caused by the compression of neurovascular structures, can occur. 11
The surgical treatment method is determined on the basis of the patient’s symptoms, age, and disease severity. For focal lesions, ray amputation and soft tissue debulking surgery may be appropriate for achieving cosmetic improvement without causing functional or neurological problems. 12 Previous studies reported that after soft tissue debulking, the recurrence rate is very high at 33% to 60%. 13 Additionally, damage to the digital artery during surgery can cause skin necrosis and inhibit wound healing. 13 In severe cases, several types of osteotomies are required, with repeat soft tissue debulking surgeries. In the present case, good results were achieved with debulking surgery and distal phalangeal resection without MTP or ray amputation, for better cosmetics. As a preoperative surgical plan, the skin incision design for reconstruction of the toe is essential, and we attempted to excise all pathological tissue while preserving the joint as much as possible. At the final follow-up, the patient was satisfied with the outcome, could wear shoes of the same size on both feet, and had normal walking ability.
Through this case, we demonstrated that debulking surgery can be a reasonable option for MDL patients.
Footnotes
Acknowledgements
This study is supported by Wonkwang University 2023.
Author contributions
All authors contributed to data collection, writing and revising the manuscript.
Data availability statement
The data that support the findings of this study are openly available.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Ethics statement
Ethics approval was not required for this study because of the retrospective design and because consent for publication was obtained from the patient.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.