
Abstract
Fallopian tube carcinoma has a rare incidence and dismal prognosis. Sister Mary Joseph’s nodule is an intra-abdominal tumor that metastasizes to the umbilicus. To date, fewer than 10 cases of fallopian tube carcinoma with Sister Mary Joseph’s nodule have been reported, with most of them exhibiting a very poor prognosis. Herein, we described a case of fallopian tube carcinoma with Sister Mary Joseph’s nodule. A 57-year-old woman was referred to the Affiliated Hospital of Shandong Second Medical University in May 2020 owing to a mass in the middle of her umbilicus. She was first diagnosed with an umbilical mass and underwent a resection of the umbilical mass, which revealed adenocarcinoma, most likely of reproductive origin. One month after the first surgery, she underwent laparoscopic cytoreductive surgery, and pathological examination revealed fallopian tube adenocarcinoma with pelvic lymph node metastasis. She was diagnosed with fallopian tube carcinoma (stage IIIC) and then underwent 10 cycles of chemotherapy. She achieved a complete response, and no recurrence or progression has been reported until now. The overall survival time exceeded 50 months. Thus, for patients with umbilical masses, physicians should consider the possibility of Sister Mary Joseph’s nodule. When a malignancy is suspected in the abdominal or pelvic cavity but the physical examination and imaging studies reveal no abnormality, laparoscopic surgery should be used for determining the primary tumor. For patients with fallopian tube carcinoma and Sister Mary Joseph’s nodule, surgery and adjuvant chemotherapy can achieve good results.
Keywords
Introduction
Fallopian tube carcinoma (FTC) is a rare gynecologic tumor that accounts for 0.14%–1.8% of all female genital malignancies. 1 A population-based study indicated that the average incidence of FTC is 3.6 cases per 1,000,000 women per year. 2 The etiology of FTC remains unclear and may be related to chronic fallopian tube inflammation, infertility, tubal endometriosis, and tuberculous salpingitis. The clinical manifestations of fallopian tube cancer, including abdominal pain, abdominal mass, vaginal discharge, vaginal bleeding, or no symptoms, are not specific. Only 15% of patients with fallopian tube cancer exhibit “Laztko’s triad of symptoms,” which include vaginal discharge, abdominal pain, and a palpable pelvic mass. 2 FTC mainly metastasizes through direct invasion, implantation metastasis, lymphatic spread, and hematogenous metastasis, similar to the metastasis of ovarian cancer.
The metastatic sites of FTC are mainly located in the abdominal and pelvic cavities, and some patients may have extraperitoneal metastasis such as bone and skin metastases. Umbilical metastasis is a rare type of skin metastasis of unknown origin. It is also known as Sister Mary Joseph’s nodule (SMJN), which was named after an American surgical assistant, Sister Mary Joseph. 3 SMJN generally refers to an intra-abdominal tumor that metastasizes to the umbilicus. The incidence of SMJN is extremely low, with only approximately 1%–3% of abdominal and pelvic malignancies metastasizing to the umbilical region. In men, the most common primary site is the stomach, whereas in women, the most common primary site is the ovary. Patients with SMJN have a poor prognosis. 4 Herein, we reported a rare case of FTC with SMJN at initial diagnosis.
Case presentation
A 57-year-old woman was admitted to the General Surgery Department of the Affiliated Hospital of Shandong Second Medical University in May 2020 owing to “repeated rupture of an umbilical mass for 2 months.” She had a 2-year history of hypertension and diabetes and underwent right salpingectomy 27 years ago. She experienced natural menopause at the age of 55 years and had regular menses up to menopause. Her sister had breast cancer, her father and brother had bone cancer, and her mother had diabetes. Physical examination revealed a pink mass measuring 2.5 cm × 2.0 cm × 1.5 cm in the middle of the umbilicus, with a 1-cm long surface rupture surrounded by hyperplastic granulation tissue. The mass was hard, with clear boundaries and painful upon squeezing. A small amount of yellow–white pus oozed from the rupture after extrusion.
Timeline
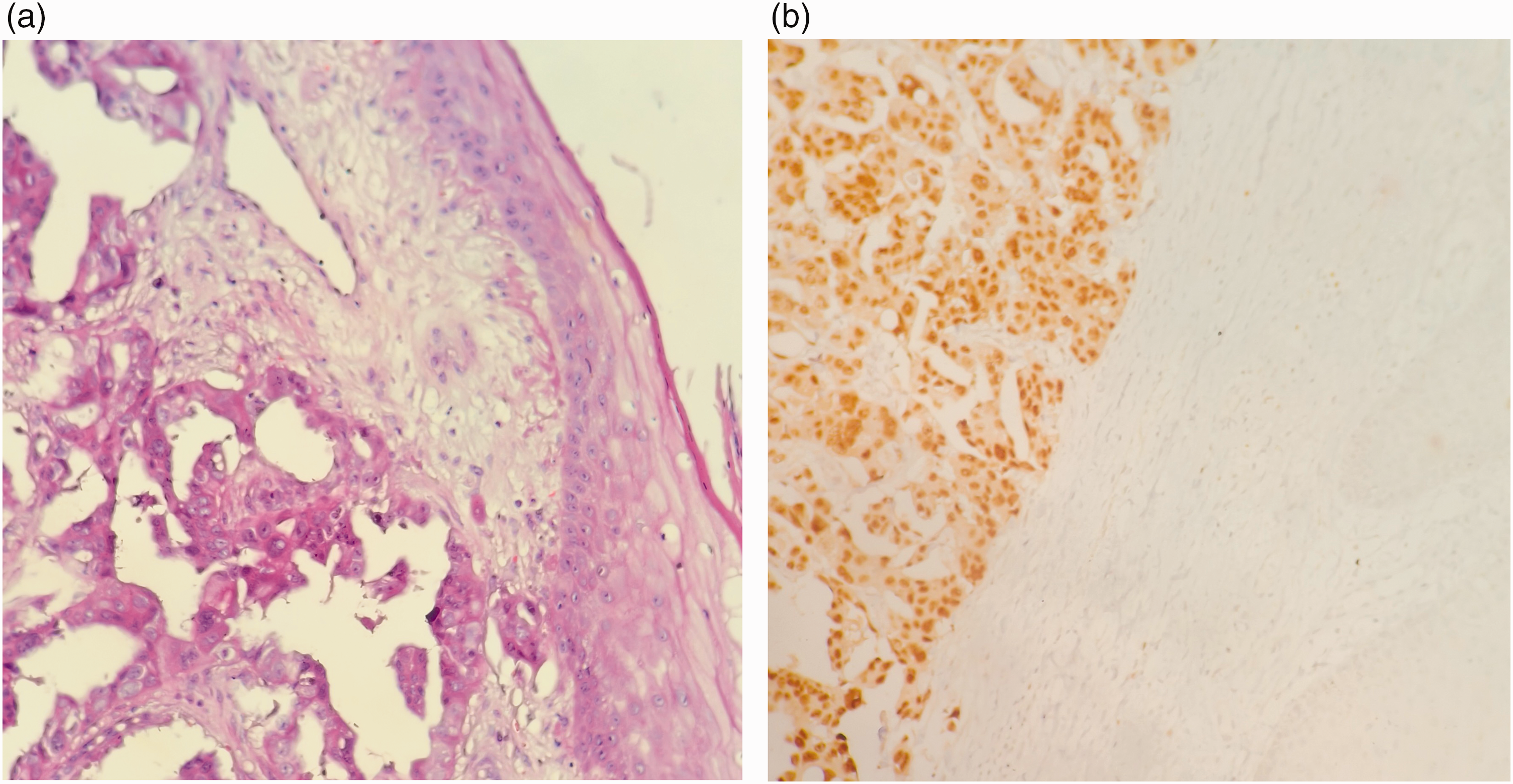
The patient was first diagnosed with umbilical inflammation and underwent surgery for removal of the umbilical mass. Histopathological examination after surgery revealed high-grade serous adenocarcinoma tissue under the squamous epithelium of the umbilicus containing a large number of psammoma bodies (Figure 1). Immunohistochemical analysis showed that the tumor was positive for cytokeratin 7 (CK7), paired box 8 (PAX-8), CK8, CK19, Wilms tumor 1 (WT-1), estrogen receptor (ER), and carbohydrate antigen 125 (CA-125) and negative for progesterone receptor (PR), CK20, GATA binding protein 3 (GATA3), thyroid transcription factor 1 (TTF-1), caudal type homeobox 2 (CDX-2), and Villin, indicating its origin in the reproductive system. These findings revealed that the umbilical mass was indicative of skin metastasis of primary FTC.

High-grade serous adenocarcinoma tissue of the left fallopian tube (HE: original magnification, 200× (a); p53: original magnification, 200× (b)). HE: hematoxylin–eosin.
One month after the first surgery (surgical excision of the umbilical mass), the patient was admitted to the gynecological ward. Physical examination showed no apparent abnormalities in the breast, whole abdomen, or pelvis. The results of serum tumor marker testing were as follows: CA-125 level: 47.23 U/mL; CA-153 level: 12.08 U/mL; CA-199 level: 69.40 U/mL; and human epididymis protein 4 level: 71.88 pmol/L. Computed tomography (CT) revealed multiple cystic lesions in the upper hepatic region with partial calcification and high-fat density around the umbilicus and uterus, accompanied with multiple calcifications. Magnetic resonance imaging of the upper abdomen and pelvis revealed abnormal signals at the top of the liver; slightly enriched diffusion-weighted imaging with background body signal suppression signals; postoperative changes around the umbilicus; mildly enlarged lymph nodes in the retroperitoneum, pelvic, and bilateral inguinal regions; and nodules between the uterine body and cervix, suggesting uterine fibroids. During laparoscopy in June 2020, a small amount of pale yellow cloudy ascitic fluid was noted in the pelvic cavity, right iliac fossa, and hepatic surface. No abnormal findings were observed in the uterus, bilateral ovaries, surface of the omentum majus, liver, or diaphragm. The right fallopian tube was absent. A friable tumor measuring approximately 1.0 cm × 0.8 cm ×0.5 cm was observed in the fimbriae of the left fallopian tube. Rapidly frozen pathology showed serous carcinoma of the fallopian tube. Based on these findings, the patient proceeded to undergo laparoscopic total hysterectomy, left salpingectomy, bilateral oophorectomy, total omentectomy, and pelvic and para-aortic lymphadenectomy. Histopathological examination after surgery revealed a high-grade serous carcinoma of the left fallopian tube, with local invasion into the deep wall of the fallopian tube (see Figure 2) and metastasis to the right pelvic lymph nodes (see Figure 3). Immunohistochemical staining was positive for P53, WT-1, P16, CK7, CK20, and calretinin and showed slight positivity for ER and Ki-67 (approximately 70%). According to the 2014 International Federation of Gynecology and Obstetrics (FIGO) staging for ovarian, fallopian tube, and peritoneal cancers, the tumor was assigned stage IIIC. Genomic sequencing analysis of the breast cancer susceptibility gene (BRCA) revealed the presence of BRCA2 NM_000059.3:c.7707dupT(p. Lys2570*, Het) mutation. The patient subsequently received six cycles of chemotherapy with paclitaxel (175 mg/m2) and carboplatin (AUC 5) and four cycles of chemotherapy with paclitaxel (175 mg/m2) every 3 weeks. After chemotherapy, no measurable lesions were observed on CT, and the serum tumor markers returned to normal levels. According to the Response Evaluation Criteria in Solid Tumors (RECIST), the patient achieved a complete response.
High-grade serous adenocarcinoma tissue under the squamous epithelium of the umbilicus (HE: original magnification, 200× (a); PAX8: original magnification, 200× (b)). HE: hematoxylin–eosin; PAX8: paired box gene 8.
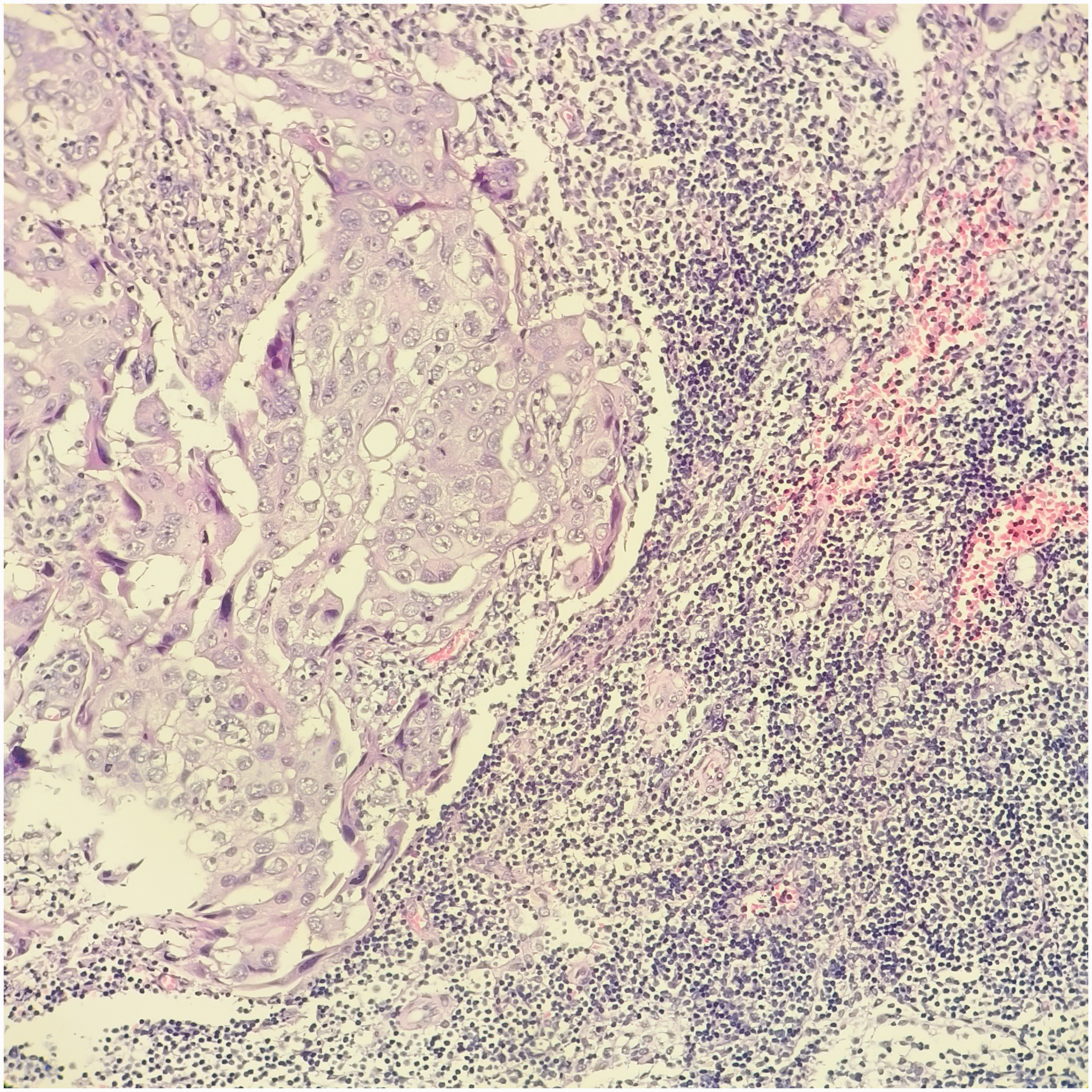
High-grade serous carcinoma metastasizing to the right pelvic lymph node (original magnification, 200×).
Considering the pathogenic mutation in BRCA2, maintenance therapy with an oral poly(ADP-ribose) polymerase (PARP) inhibitor was recommended; however, the patient declined treatment. She was followed up for serum tumor marker assessment and CT every 3 months for 2 years after completing chemotherapy and every 6 months since February 2023. The timeline was shown in Table 1. No recurrence of fallopian tube cancer has been observed. The reporting of this case conforms to the Case Report (CARE) guidelines. 5 Written treatment consent was obtained from the patient before the initiation of all treatments.
Summary of timeline.

Discussion
SMJN, which refers to the umbilicus metastasis of a malignant tumor, is regarded an ominous indicator with regard to prognosis. SMJN originates mainly from abodominal malignancy and sometimes from intra-abdominal lesions such as breast cancer. The symptoms of SMJN primarily include a belly button mass, which may be painful and ulcerated, with the mass rarely discharging pus, blood, or serous fluid. It usually exhibits a tough texture, ranging from 0.5 to 5 cm in diameter. 4 In males, SMJN mainly originates from gastrointestinal cancer, most commonly gastric cancer, whereas in females, the main source is the reproductive system, most commonly ovarian cancer. 5 Only nine cases of FTC combined with SMJN have been reported in the literature.6–10 Considering the histopathology, adenocarcinoma is the most common type, accounting for approximately 75% of all cases, followed by squamous cell carcinoma, sarcoma, melanoma, and lymphoma. 11 In many cases, umbilical plexus lesions may be benign, such as in cases of keloids, fibroids, endometriosis, foreign body granuloma, hernia, and myxoma. 12 Tumors in the abdominal or pelvic cavity may metastasize to the umbilicus via direct invasion, hematogenous (arterial and venous) and lymphatic routes, and direct extension along the remnants of embryonic ligaments. Direct implantation of the laparoscopic puncture port site is another approach for the tumor to spread to the umbilicus. 13 This patient was misdiagnosed with a benign umbilical mass without undergoing any abdominal tumor assessment. Physicians should pay attention to the differentiation of umbilical masses from the origin. If necessary, fine-needle aspiration cytology or dermoscopy can be used to determine the nature of the tumor; however, it should be performed under careful supervision.14,15
In this patient, histopathological examination of the umbilical mass was suggestive of reproductive origin; however, physical examination and imaging studies, including CT, did not reveal any pelvic mass or enlarged lymph nodes. Therefore, laparoscopy was planned to search for the primary tumor in the abdomen and/or pelvis. A delicate tumor measuring approximately 1.0 cm × 0.8 cm × 0.5 cm was indeed found at the fimbriae of the left fallopian tube during surgery, accompanied with right pelvic lymph node metastasis. Compared with previously reported cases, this patient developed SMJN and lymph node metastasis in the absence of a significant intra-abdominal tumor and extensive abdominal metastasis. 16 Laparoscopy can serve as an effective method for identifying primary abdominal and/or pelvic tumors when the origin of an umbilical malignancy remains uncertain.
SMJN represents extensive cancer metastases and are usually treated palliatively. 17 The prognosis of patients with SMJN is poor, with an average overall survival (OS) of 2–11 months. 18 According to the National Comprehensive Cancer Network guidelines, for advanced-stage patients, primary or interval debulking surgery is considered the first choice, followed by adjuvant therapy such as chemotherapy. PARP inhibitors can also be prescribed as maintenance therapy after surgery and chemotherapy. 19 The current patient had an OS of >50 months. She underwent an optimal cytoreductive surgery and 10 cycles of chemotherapy with a carboplatin–paclitaxel regimen. Although she did not use PARP inhibitor maintenance treatment, her prognosis was excellent. This may be related to the fact that she underwent radical surgery and complete chemotherapy and that the tumor did not metastasize extensively within the abdominal cavity.
Conclusion
SMJN is considered the first presenting sign or recurrent manifestation of FTC. In the early stage, the baseline tumor burden is low; however, it may also metastasize to the umbilicus through various routes. Physicians should consider whether an umbilical mass is an SMJN when evaluating patients with an umbilical mass. Laparoscopy should be considered in cases where a patient is suspected of having an intra-abdominal or pelvic tumor, but imaging and physical examination findings are unremarkable. When laparoscopic surgery is performed in a patient, tumor implantation into the puncture port site or surgical incision should be avoided. For managing FTC metastasis to the umbilicus, the ovarian cancer treatment guidelines can be referred. Surgical resection is the first choice for resectable lesions, followed by adjuvant chemotherapy and targeted therapy such as PARP inhibitors. For unresectable disease, neoadjuvant chemotherapy may be considered, followed by intermittent debulking surgery and adjuvant chemotherapy.
List of abbreviations
FTC: fallopian tube carcinoma; SMJN: Sister Mary Joseph’s nodule; CA: carbohydrate antigen; CT: computed tomography; FIGO: the International Federation of Gynecology and Obstetrics; BRCA: breast cancer susceptibility gene; PARP: poly(ADP-ribose) polymerase; CK7: cytokeratin 7; PAX-8: paired box 8; WT-1: Wilms tumor 1; ER: estrogen receptor; PR: progesterone receptor; GATA3: GATA binding protein 3; TTF-1: thyroid transcription factor 1; CDX-2: caudal type homeobox 2.
Footnotes
Acknowledgments
Not applicable.
Author contributions
XJ: Data Curation, Writing—Original Draft, Visualization; PZ: Visualization, Data Curation; HY: Resources, Visualization; XW: Writing—Review & Editing; JM and HW: Writing—Review & Editing, Supervision.
Consent for publication
Written consent to publish was acquired from the patient.
Data availability statement
All the generated data are included in this article.
Declaration of conflicting interests
The authors declare that they have no competing interests.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Patient perspective
The patient was satisfied with the treatments received.