
Abstract
The primary symptom of urticarial vasculitis (UV), which is a histopathological leukocytoclastic vasculitis disease, is an eruption that resembles urticaria. Other organs may also experience accompanying symptoms. Lung lesions with UV are mostly obstructive pulmonary disease with smoking. However, the coexistence of eosinophilic pneumonia (EP) and complicated UV remains unclear. We report a man in his 70s with chronic obstructive pulmonary disease who attended our department with ring-shaped erythema, marginal edema, and pigmentation. Additionally, a skin histological analysis showed nuclear dust and perivascular neutrophil infiltration, while a blood sample showed a decrease in C3 and C1q concentrations. Administration of prednisone temporarily improved the eruption. However, he developed a cough and a new UV eruption 1 year later. Computed tomography revealed infiltration in the right upper lobe of the lungs, and a blood sample showed a high eosinophil count. He was finally diagnosed with hypocomplementemic urticarial vasculitis syndrome and idiopathic chronic EP. A previous study showed that serum C1q concentrations in patients with EP were lower when this disease was active. Whether a decline in C1q concentrations can cause EP is unclear. However, our case is unique owing to the co-onset of EP with low complement concentrations and recurrence of UV.
Keywords
Introduction
Urticarial-like eruptions are the main sign of urticarial vasculitis (UV), which comprises different types, such as leukocytoclastic vasculitis and hypocomplementemic urticarial vasculitis syndrome (HUVS). HUVS is a rare and potentially severe form of UV. Other organs might develop symptoms associated with UV. 1 Lung lesions with UV are mostly obstructive pulmonary disease due to smoking. 1 Whether complicated UV and eosinophilic pneumonia (EP) may coexist is unknown. We describe the case of a man in his 70 s with chronic obstructive pulmonary disease (COPD) who had UV and EP concurrently.
Case report
A man in his 70 s with COPD and no history of asthma smoked 20 cigarettes/day starting in his 30 s, but stopped smoking at the age of 55 years. He sought treatment from our department a few months before developing erythema that persisted, despite using antihistamines. In his neck and extremities, he had ring-shaped erythema with marginal edema and central pigmentation (Figure 1a), and complained of pain in both elbows. Clinical photographs have been provided with the patient’s written informed consent. All patient information has been de-identified, and the Institutional Review Board of Dokkyo Medical University approved publication (DMUH-CR2023-001).

Photographs and histology of the patient. (a) Photograph of the anterior neck. Ring-shaped erythema with marginal edema and pigmentation can be seen. (b and c) Histological sections show dermal edema, perivascular neutrophil infiltration, nuclear dust, and thickening of the vascular endothelium and (d) Photograph showing recurrent urticarial vasculitis at the time of pneumonia.
There were no signs other than those in the skin and joints. A skin histological examination showed dermal edema, perivascular neutrophilic infiltration, nuclear dust, and thickening of the vascular endothelium (Figure 1b and c). A blood sample showed a decrease in the C3 concentration (3.7 µmol/L; normal range: 4.5–8.4 µmol/L, C4 was within the normal range) and a decrease in the C1q concentration (<1.5 µg/mL; normal range: 1.6–3.0 µg/mL by enzyme-linked immunosorbent assay). All autoantibodies associated with rheumatoid disease (e.g., anti-dsDNA, Smith, ribonucleoprotein, and phospholipid antibody), including antinuclear antibodies and antineutrophil cytoplasmic antibodies, and cryoglobulin were negative, but the anti-C1q antibody could not be tested because of technical difficulty. He was diagnosed with UV and prescribed prednisone 20 mg/day. The dose was tapered off owing to a good response. One year later, he visited the Respiratory Department after developing a cough for a few weeks. He was taking 5 mg/day of prednisone at that time. Additionally, the same skin eruptions caused by UV the previous year had recurred (Figure 1d), and serum C3 and C1p concentrations were decreased (C3: 3.6 µmol/L), as well as C1q concentrations (0.17 µmol/L; normal range: 0.19–0.33 µmol/L by nephelometry). Computed tomography (CT) showed diffuse consolidation in the right upper lobe and a slightly infiltrative image in the right part of the left upper lobe of the lungs (Figure 2a). The blood eosinophil count was high (42.2%). Moreover, eosinophilic infiltration was visible in a transbronchial lung biopsy (Figure 2b and c), and the eosinophil count was increased by 64% in bronchoalveolar lavage fluid.
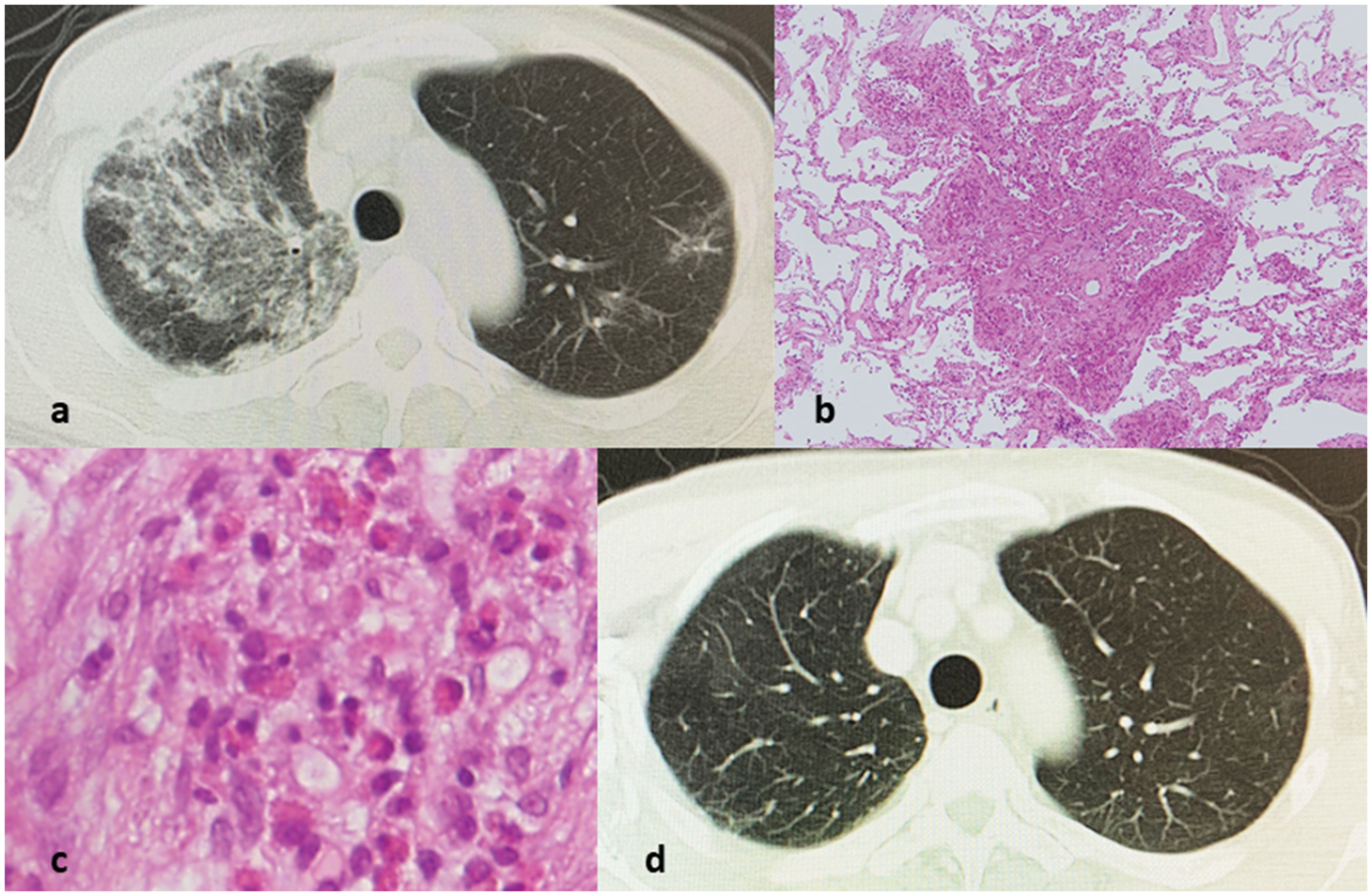
Computed tomography and histological images of the patient. (a) Computed tomography shows infiltration in the right upper lobe of the lung. (b and c) A transbronchial lung biopsy shows fibrosis and eosinophilic infiltration and (d) Lung computed tomography findings have improved with steroid administration.
His lung lesions were differentially diagnosed by following the chronic EP (CEP) diagnostic criteria of Cottin et al. 2 A culture test for bacteria, fungi, and mycobacteria in his bronchoalveolar lavage fluid and sputum was negative, as well as a serum Aspergillus antigen test and b-D-glucan test. In addition, there was no evidence suggesting a drug allergy, parasite infection, or hematological disorder. When the prednisolone dose was increased to 20 mg, his cough improved, and the infiltrative images in CT disappeared after 1 month (Figure 2d). Two months later, his pneumonia worsened owing to self-discontinuation of prednisone, but it improved after medication counseling. The patient was transferred to the local hospital 6 months after the prednisone dosage was lowered to 10 mg. At our hospital, he provided approval for every treatment and examination that were carried out.
The patient’s CT pulmonary lesions were unusual for CEP. Diffuse pulmonary alveolar consolidation with an air bronchogram and/or ground-glass opacities at chest imaging, particularly with a peripheral preponderance, are diagnostic criteria for CEP. 2 Although the CT results were inconsistent, the other examination findings, strong steroid response, and chronic clinical course suggested the diagnosis of CEP. Therefore, CEP was chosen as the diagnosis. This study adheres to the CARE reporting standards. 3
Discussion
HUVS is an uncommon disease that was first described by McDuffie et al. in 1973.1,4 Low serum complement and C1q concentrations, and chronic urticarial vasculitic lesions that last longer than 24 hours or frequently recur are the main signs of HUVS.1,4 Additionally, serum C1q precipitins were initially identified and later confirmed as C1q autoantibodies. 4 The diagnosis of HUVS is different from that of other secondary types of UV (Chapel Hill classification), 5 and the findings in our case fit the description of HUVS. In HUVS, pulmonary lesions occasionally coexist. In a case series of 18 patients with UV, Wisnieski et al. 1 found that 11 had pulmonary lesions, all of them had COPD, and 9 (81.1%) of 11 of them were moderate to heavy smokers (10–51 pack years). In our case, the patient had a long history of tobacco use and had already been diagnosed with COPD. Therefore, an association between HUVS and smoking was also postulated.
Idiopathic CEP is a rare disease of unknown etiology and is generally not associated with smoking. Patients with CEP have complications, such as asthma, which is thought to be affected by allergies. 6 An interesting finding was reported by Demedts et al., who found that serum C1q concentrations in patients with CEP were lower when this disease was active. 7 In our case, C1p concentrations were decreased at the time of EP onset. Even though there is uncertainty whether a decline in C1q concentrations can cause EP, 7 our case is unique owing to the co-onset of EP with low complement concentrations and recurrence of UV.
Wisnieski et al. 1 performed bronchoscopy in only four cases in their case series and found no evidence of vasculitis or EP. Therefore, details remain unknown for the remaining seven cases. Unfortunately, lung CT findings were not mentioned in their study. Therefore, the characteristics of CT lesions in these cases is unknown. Unfortunately, such unique situations are inadequately reported. The findings in our case suggest some associations between HUVS, CEP, and smoking.
Footnotes
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Data availability statement
All data generated or analyzed during this study are included in the published article.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.