
Abstract
Objective
To investigate the relationship between the neutrophil-to-lymphocyte ratio and chronic obstructive pulmonary disease complicated with pulmonary hypertension (COPD + PH).
Methods
We retrospectively analyzed clinical data from 242 COPD patients at our hospital from July 2018 to July 2019. Patients underwent examinations including blood analysis, C-reactive protein, N-terminal brain natriuretic peptide (BNP), pulmonary function, and cardiac color ultrasound.
Results
Patients were divided into the COPD and COPD + PH groups using pulmonary arterial pressure (<50 and ≥50 mmHg, respectively). Compared with the COPD group, the COPD + PH group had greater pulmonary arterial pressure, smoking history, neutrophil-to-lymphocyte ratio (NLR), C-reactive protein, BNP, Chronic Obstructive Pulmonary Disease Assessment Test score, and right atrium and ventricular diameters, but smaller body mass index, forced vital capacity, lymphocyte count, and left ventricular diameter. BNP and NLR had positive effects on PH; forced vital capacity had a negative impact. Moreover, BNP (area under the curve [AUC] = 0.748, sensitivity = 0.692, specificity = 0.701) and NLR (AUC = 0.679, sensitivity = 0.831, specificity = 0.452) had predictive value for PH, and both were positively correlated with PH.
Conclusions
NLR is associated with COPD + PH, and may be useful for its diagnosis.
Keywords
Background
Chronic obstructive pulmonary disease (COPD) is a clinical syndrome that is characterized by chronic respiratory symptoms, abnormal lung structure, lung function damage, or more than such two manifestations simultaneously. 1 The clinical manifestations and pathogenic mechanisms of COPD are highly heterogeneous. 2 Approximately 10% to 30% of moderate or severe COPD patients will develop pulmonary hypertension (PH). 3 COPD patients with a PH phenotype have an increased risk of acute exacerbation, increased mortality, and significantly impaired functional parameters (e.g., severe hypoxemia, low diffusing lung capacity for carbon monoxide, and decreased 6-minute walking distance). 4 , 5 Although PH is a common complication of COPD, its prognosis is poor; greater attention should therefore be paid to the diagnosis and treatment of PH. Right heart catheterization is the gold standard for diagnosing PH, but it is both expensive and invasive. Doppler echocardiography is the main non-invasive diagnostic tool for predicting PH in patients with COPD. However, ultrasound examination has certain limitations, 6 and it is difficult to implement in primary hospitals because of its imperfect COPD detection. Simple, feasible, and reliable indicators of PH are therefore needed to provide valuable information for diagnosing COPD patients.
The neutrophil-to-lymphocyte ratio (NLR) is a systematic biomarker that can reflect immune status and systemic chronic inflammation. NLR is related to the severity, nutritional status, recurrence, and fatality of a variety of chronic diseases, such as heart and kidney diseases.7–9 Moreover, it has been reported that NLR may be a promising marker for early the detection of COPD. 10 Together, these studies indicate that NLR has an important auxiliary diagnostic value for COPD.
Yanartas et al. 11 reported that elevated NLR may be useful for predicting postoperative mortality in patients with chronic thromboembolic PH. Furthermore, NLR may predict the prognosis of acyanotic congenital heart disease with PH. 12 These findings suggest the existence of a relationship between NLR and PH. Notably, NLR is also affected in other chronic diseases such as obesity, diabetes, and stroke. 13 , 14 However, the relationship between NLR and COPD complicated with PH (COPD + PH) remains largely undetermined. In the present study, we therefore aimed to explore the relationship between NLR and COPD + PH, and to analyze the value of NLR in the auxiliary diagnosis of COPD + PH.
Materials and methods
Research subjects
This retrospective study included patients with COPD who were treated in the Department of Respiratory Medicine of Liaocheng People’s Hospital from July 2018 to July 2019. All enrolled patients gave their written informed consent, and the study was approved by the ethics committee of Liaocheng People’s Hospital (approval no. 2018022). All patient details have been de-identified, and the reporting of this study conforms to TRIPOD (Transparent Reporting of a multivariable prediction model for Individual Prognosis or Diagnosis) guidelines. 15
In this study, we enrolled patients aged >50 years. Patients with any smoking status (never, current, or past) were included. Patients with financial means received long-term oxygen therapy or non-invasive mechanical ventilator treatment. The patients were divided into two groups: the COPD (COPD patients with pulmonary artery systolic pressure [PASP] < 50 mmHg) and COPD + PH (COPD patients with PASP ≥50 mmHg] groups.
According to the 2018 Golden Guidelines for COPD, 16 patients were included if they had chronic cough, expectoration, shortness of breath, and/or the presence of risk factors (such as smoking). For inclusion in the study, after bronchodilator inhalation, patients with a forced expiratory volume in 1 s (FEV1)-to-forced vital capacity (FVC) ratio (FEV1/FVC) < 0.7, or those with acute exacerbation of COPD, had an improved condition after treatment and were discharged; their condition was stable without acute exacerbation during at least 1 month of follow-up. Exclusion criteria for all patients were as follows: patients with pneumonia, lung abscess, pulmonary tuberculosis, bronchiectasis, bronchial asthma, interstitial lung disease, lung cancer, or other respiratory diseases; patients with severe underlying diseases or comorbidities who were not expected to survive; patients with heart diseases (such as left heart failure or coronary heart disease) or peripheral vascular diseases; patients with autoimmune diseases; or patients with pre-existing mental illness. For inclusion into the COPD + PH group, patients also needed to have a PASP on cardiac ultrasound of ≥50 mmHg. 17 , 18 Patients were excluded from the COPD + PH group if their PH was caused by an autoimmune disease or other known causes.
Clinical analyses
General clinical data
Sex, age, body mass index (BMI), smoking history, medication history, the number of acute exacerbations of COPD in the year before enrollment, and the course of diagnosed COPD were recorded. Blood routine (such as white blood cell, red blood cell, hemoglobin, neutrophil, and lymphocyte analyses), C-reactive protein (CRP; normal limits: 0–10 mg/mL), and BNP (normal limits: 0–125 pg/mL) tests were performed by the Laboratory Department of Liaocheng People’s Hospital. Pulmonary function testing (including FEV1, FVC, and FEV1/FVC) was performed by professionals in the pulmonary function room of Liaocheng People’s Hospital in strict accordance with the pulmonary function operation guide, 19 using a pulmonary function testing system (CHESTAC-33:8800, CHEST M.I., Inc., Tokyo, Japan). Dyspnea status was detected using the modified Medical Research Council dyspnea scale, and the COPD Assessment Test (CAT) was used to evaluate clinical symptoms. Symptom control was assessed using the Clinical COPD Questionnaire. The NLR was calculated using absolute neutrophil and lymphocyte counts.
Echocardiography
Echocardiography was measured by an experienced professional physician in the echocardiography room using a Vivid E9 Cardiac Ultrasound with color Doppler (GE Healthcare, Chicago, IL, USA) with an M5S probe (probe frequency: 1.7–3.4 MHz). Physicians were on the left side during inspections. Patients were evaluated during quiet breathing with synchronous connection electrocardiogram. A heart echocardiography was performed on the patients, with the following main measurement calculations: right chamber inside diameter (two-dimensional ultrasound in apex four-chamber view, measurement of end systolic right in the middle of the short axis transverse diameter), right ventricular diameter (two-dimensional ultrasound in end-diastolic right ventricular apex four-chamber view, measurement of the basal segment diameter), right atrial diameter, tricuspid annulus plane contractile displacement, PASP, left ventricular diameter, left atrial diameter, and left ventricular ejection fraction. The parameters and measurement methods were performed in accordance with the American Society of Echocardiography guidelines for adult echocardiography. 20
Statistical methods
IBM SPSS Statistics for Windows, version 26.0 (IBM Corp., Armonk, NY, USA) was used for data analysis. If measurement data were normally distributed, they are expressed as the mean ± standard deviation, and comparisons between two groups were performed using the two-sample t-test. If distribution was not normal, the median (interquartile range) is used to express the data, and comparisons between two groups were performed using the fit test. Enumeration data are expressed as the number of cases (percentage), and comparisons between two groups were performed using the χ2 test. Linear and logistic regression analyses were used to explore the risk factors of COPD + PH. Spearman’s correlation was used to analyze correlations between two variables. Receiver operating characteristic (ROC) curves were used to evaluate the diagnostic value of related indexes. For all tests, P < 0.05 was considered significant.
Results
In the present study, 242 patients were included. The baseline characteristics of patients are shown in Table 1. With PASP ≥ 50 mmHg as the cutoff value, the enrolled patients were divided into the COPD (n = 177, median age 66 [range 53–79] years) and COPD + PH (n = 65, median age 64 [range 54–77] years) groups. Compared with the COPD group, the COPD + PH group had significantly higher pulmonary artery pressure (t = −11.92, P < 0.01), history of smoking (t = 21.465, P < 0.01), CAT score (t = −2.09, P < 0.05), NLR (t = −4.26, P < 0.01), BNP (t = −5.91, P < 0.01), and CRP (a systemic infection marker; 21 t = −2.13, P < 0.05). Given that all participants in the study were diagnosed with stable COPD, and patients were not in the acute phase of infection, the elevated CRP level may not have been a result of infection. Compared with the COPD group, the COPD + PH group had significantly lower BMI (t = −5.91, P < 0.01), FEV1 (t = −2.16, P < 0.05), FVC (t = −3.21, P < 0.01), and number of lymphocytes (t = −4.01, P < 0.01), as well as a smaller left ventricular diameter (t = −2.18, P < 0.05). By contrast, both the right ventricular diameter (t = −5.78, P < 0.01) and right atrium diameter (t = −5.34, P < 0.01) were larger in the COPD + PH group than in the COPD group. There were no significant differences between the two groups in any other related variables.
General data from COPD and COPD + PH patients.

BMI, body mass index; BNP, N-terminal brain natriuretic peptide; CAT, Chronic Obstructive Pulmonary Disease Assessment Test; CCQ, Clinical COPD Questionnaire; COPD, chronic obstructive pulmonary disease; COPD + PH, chronic obstructive pulmonary disease complicated with pulmonary hypertension; CRP, C-reactive protein; FEV1, forced expiratory volume at the end of 1 s; FEV1/FVC, forced expiratory volume in one second/forced vital capacity; FVC, forced vital capacity; HG, hemoglobin; ICS, inhaled glucocorticoids; LA, left atrial; LABA, long-acting β2 receptor agonist; LAMA, a long-acting anticholinergic receptor antagonist; LV, left ventricular; LVEF, left ventricular ejection fraction; mMRC, modified Medical Research Council dyspnea scale; NLR, neutrophil-to-lymphocyte ratio; PASP, pulmonary artery systolic blood pressure; RA, right atrial; RBC, red blood cell count; RV, right ventricular; TAPSE, tricuspid annular plane systolic excursion; WBC, white blood cell count.
Univariate analysis revealed that BMI, smoking history, FVC, FEV1, CRP, BNP, CAT score, and NLR were risk factors of COPD + PH (Table 1). Parameters that were identified as potential risk factors in the univariate analysis were subsequently included in the linear regression analysis; of these, BNP (β = 0.001, 95% confidence interval [CI]: 0.001 to 0.002, P < 0.01) and NLR (β = 0.525, 95% CI: 0.062 to 0.988, P < 0.05) had a positive effect on PH, whereas FVC (β = −5.266, 95% CI: −9.740 to −0.791, P < 0.05) had a negative effect. Smoking history, BMI, FEV1, CAT, and CRP were not significantly associated with PH (Table 2). The parameters that were identified as potential risk factors in the univariate analysis were also included in the multivariate logistic regression analysis; of these, smoking cessation (OR = 0.279, 95% CI: 0.131 to 0.593, P < 0.01), never smoked status (OR = 0.032, 95% CI: 0.006 to 0.172, P < 0.01), FVC (OR = 0.245, 95% CI: 0.098 to 0.612, P= < 0.05), BNP (OR = 1.000, 95% CI: 1.000 to 1.000, P < 0.01), NLR (OR = 1.132, 95% CI: 1.027 to 1.249, P < 0.05), and CAT (OR = 1.105, 95% CI: 1.005 to 1.216, P < 0.05) were associated with PH as risk factors. By contrast, FEV1 and CRP were not significantly associated with PH (Table 3).
Linear regression analysis between PASP and patient parameters.

BMI, body mass index; BNP, N-terminal brain natriuretic peptide; CAT, Chronic Obstructive Pulmonary Disease Assessment Test; CI, confidence interval; CRP, C-reactive protein; FEV1, forced expiratory volume at the end of 1 s; FVC, forced vital capacity; NLR, neutrophil-to-lymphocyte ratio; PASP, pulmonary artery systolic blood pressure.
Binary logistic regression analysis between PASP and patient parameters.
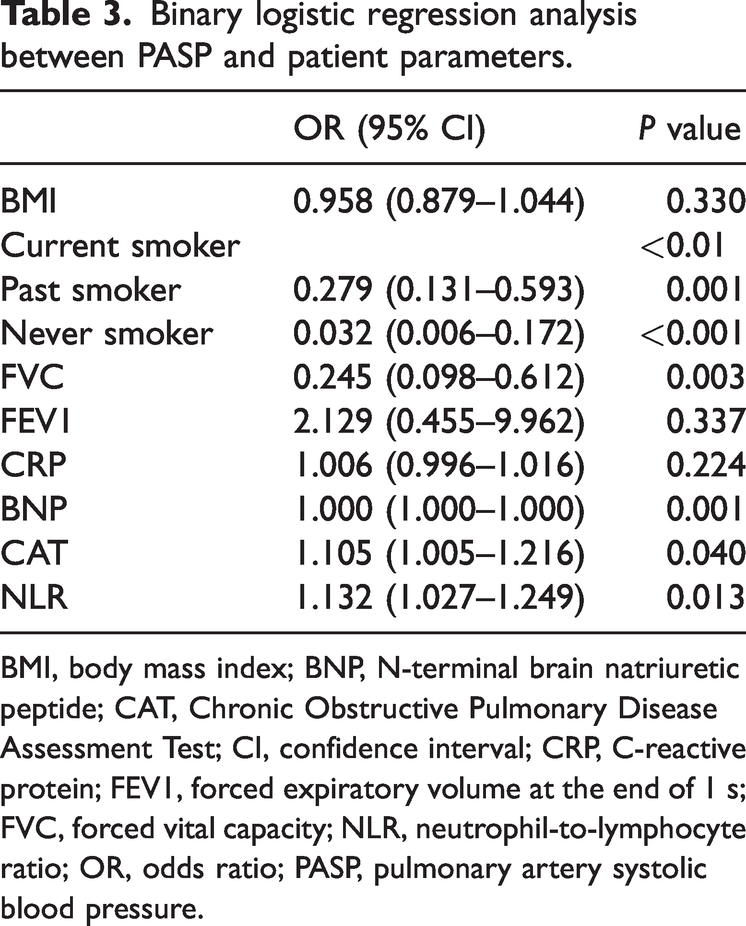
BMI, body mass index; BNP, N-terminal brain natriuretic peptide; CAT, Chronic Obstructive Pulmonary Disease Assessment Test; CI, confidence interval; CRP, C-reactive protein; FEV1, forced expiratory volume at the end of 1 s; FVC, forced vital capacity; NLR, neutrophil-to-lymphocyte ratio; OR, odds ratio; PASP, pulmonary artery systolic blood pressure.
As shown in Figure 1, an ROC curve was drawn, and Youden’s index was used to determine the optimal cut-off values of BNP and NLR, as well as their corresponding sensitivity and specificity for predicting PH. For predicting PH, the AUC of BNP was 0.748 (P < 0.01, sensitivity 0.692, specificity 0.701) and that of NLR was 0.679 (P < 0.01, sensitivity 0.831, specificity 0.452) (Table 4).
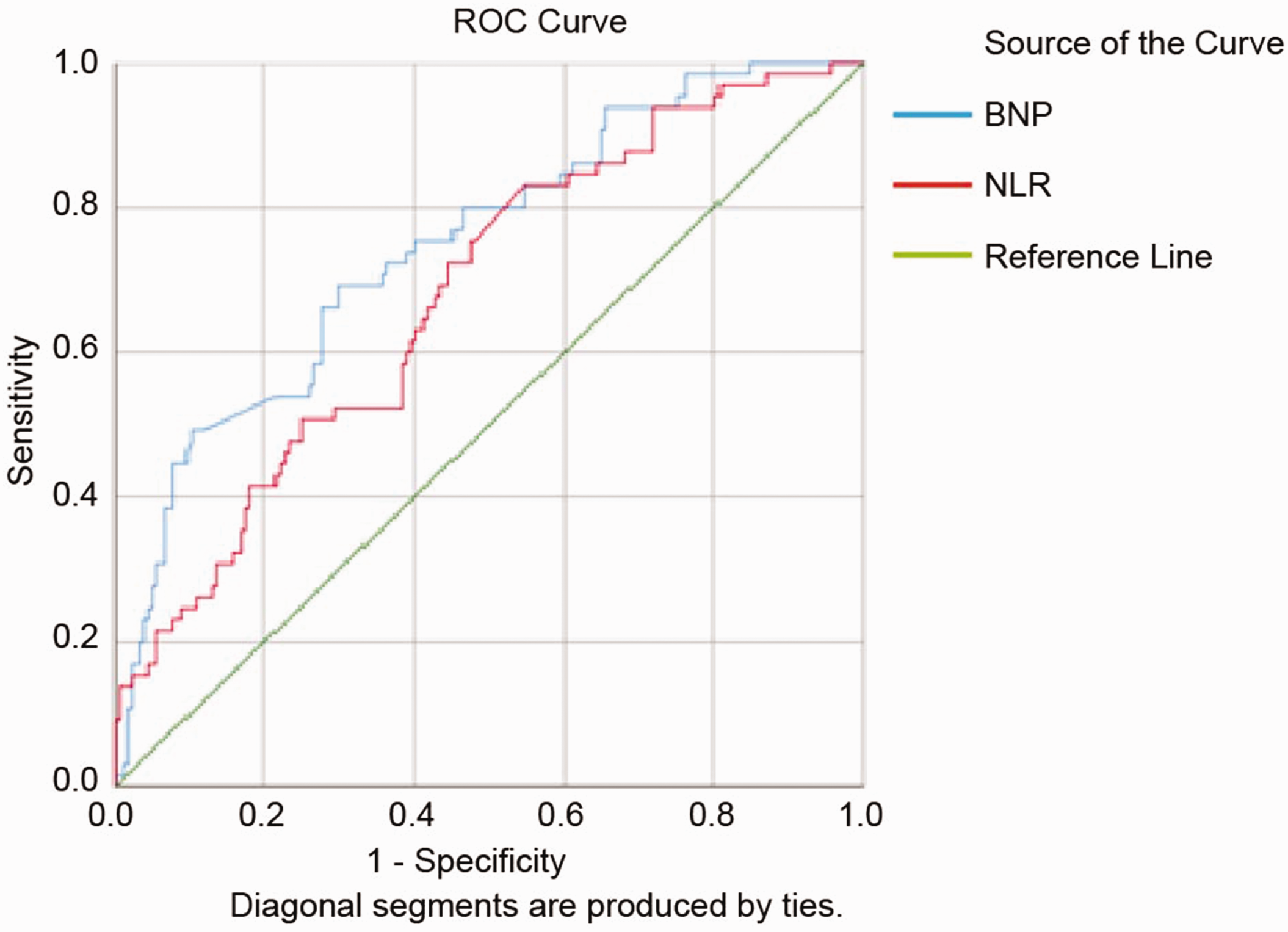
ROC curve for predicting COPD + PH. BNP, N-terminal brain natriuretic peptide; COPD + PH, chronic obstructive pulmonary disease complicated with pulmonary hypertension; NLR, neutrophil-to-lymphocyte ratio; ROC, receiver operating characteristic.
BNP and NLR predictions of PH
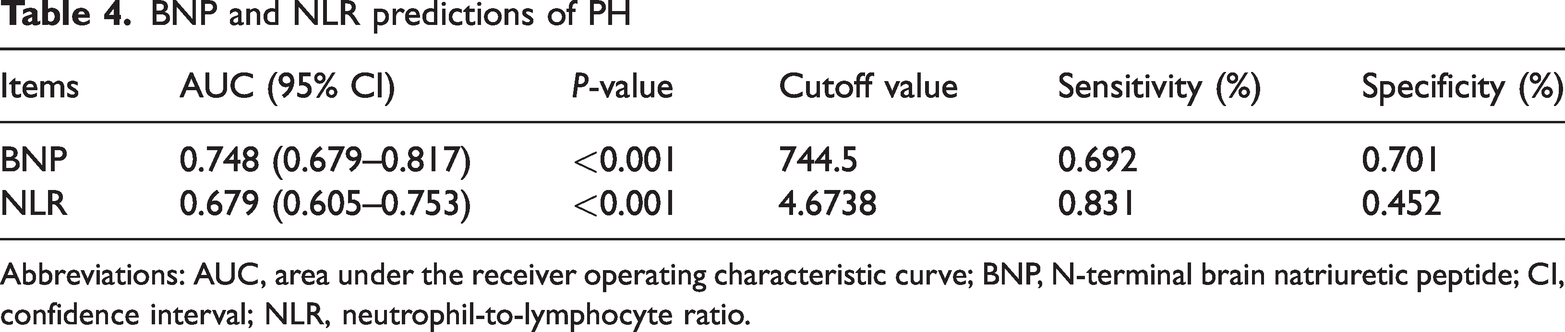
Abbreviations: AUC, area under the receiver operating characteristic curve; BNP, N-terminal brain natriuretic peptide; CI, confidence interval; NLR, neutrophil-to-lymphocyte ratio.
The laboratory parameters of BNP and NLR, which were different between the two groups, were included in the correlation analysis with PASP. Spearman correlation analysis revealed that PH was positively correlated with both BNP (r = 0.374, P < 0.01) and NLR (r = 0.322, P < 0.01) (Table 5).
Correlation analysis between PASP and patient parameters.

Abbreviations: BNP, N-terminal brain natriuretic peptide; NLR, neutrophil-to-lymphocyte ratio; PASP, pulmonary arterial hypertension.
Discussion
In the present study, the NLR of COPD + PH patients was significantly higher than that of patients in the COPD group. After adjusting for potential confounding factors using multivariate analysis, a positive correlation was identified between NLR and COPD + PH. Furthermore, the ROC curve indicated the diagnostic value of NLR for predicting COPD + PH, and correlation analysis revealed a positive correlation between PH and NLR. We therefore believe that NLR may be useful as an auxiliary diagnostic indicator of COPD + PH.
As a systemic inflammatory biomarker, NLR has been widely studied for predicting COPD progression and clinical outcome. Ellingsen et al. 22 reported that NLR is associated with the acute exacerbation of COPD; it is also reportedly associated with the 28-day mortality of patients with acute exacerbation of COPD, and might be an effective indicator for predicting short-term mortality in hospitalized patients. 23 Moreover, NLR > 8.9 (OR = 10.783, 95% CI: 2.069 to 56.194, P = 0.05) was reported as an independent risk factor for non-invasive ventilator treatment failure. 24 We have previously demonstrated that NLR is related to exercise ability in COPD patients, and may reflect cardiopulmonary reserve. 25 In addition, studies have reported that NLR is associated with functional status and adverse outcomes in patients with PH.26–28 However, relatively few studies have explored the relationship between COPD + PH and NLR. Zuo et al. 29 demonstrated that NLR has important diagnostic value in COPD + PH, but their study was limited to patients with acute COPD. The present study is thus the first to show that NLR may be important for the auxiliary diagnosis of patients with stable COPD + PH.
PH is caused by the secretion of various vasomotor factors by damaged epithelial cells, thus leading to vasoconstriction and vascular remodeling. There are many lines of evidence indicating that inflammation plays a decisive role in the development of PH. First, inflammatory pathways in PH are important pathogenesis mechanisms, and the Toll-like receptor family are the pattern recognition receptors of innate immunity. Recognition of pathogens by Toll-like receptors rapidly activates innate immune responses by inducing the production of proinflammatory cytokines—such as interleukin (IL)-1β, IL-6, IL-12, and tumor necrosis factor α—as well as the upregulation of costimulatory molecules such as cluster of differentiation (CD)40, CD80, and CD86. Second, continuous mechanical stimulation of the pulmonary vascular wall leads to an inflammatory response in the pulmonary vascular wall. The release of endothelin and other vasoconstrictive factors by pulmonary vascular endothelial cells then leads to pulmonary vasoconstriction, and ultimately PH. Third, NLR can reflect the non-specific inflammatory response and immune system status of the body, and has been widely studied for predicting COPD disease progression and clinical outcome. NLR can be used to predict the re-acute exacerbation of COPD, and is related to the readmission and mortality rates of patients. Finally, in the present study, BNP and NLR were positively correlated with PH, whereas FVC was negatively correlated with PH. We therefore speculate that NLR may be a useful auxiliary diagnostic indicator for most patients with COPD + PH.
In conclusion, the current study provides evidence that NLR may act as a new inflammatory biomarker for the evaluation of COPD + PH. As a new inflammatory biomarker, NLR testing is advantageous because of its simple operation, low cost, and wide availability; it has particularly large advantages when applied in community and primary medical institutions. This indicator may become an important monitoring method for COPD + PH. However, the present study was limited by its small sample size; large-scale, high-quality studies are needed to further determine the application potential of NLR for COPD + PH detection.
Footnotes
Acknowledgements
We thank all patients for their participation. We thank the medical staff for their assistance in patient recruitment, for performing echocardiography measurements, and for their expert support in the planning of the study protocol. We also thank all medical staff of the Laboratory for Clinical Chemistry (Liaocheng People's Hospital) for their assistance with sample preparation, measurements, and data collection.
Author contributions
Conceptualization and funding acquisition: Zhipeng Zhang, Jiang Tingting. Data curation: Lindong Yuan. Investigation: Qi Wang. Methodology: Jun Qi. Project administration: Ziyun Yang, Qinghe Jiang, and Lindong Yuan. Resources: Jing Wei. Software: Dongming Cao. Supervision: Jun Qi. Validation: Qi Wang. Writing: original draft, review and editing: Lindong Yuan, Zhipeng Zhang, and Jiang Tingting.
Declaration of conflicting interest
The authors declare that there is no conflict of interest
Funding
This study was supported by the 2021 Science and Technology Project of Shandong Geriatrics Society (funding number: LKJGG2021W070) and the Intramural Research Program of the Liaocheng People’s Hospital (funding number: LKJGG2021W070).