
Abstract
Objective
This study was performed to evaluate the effectiveness of intramedullary nailing and a lateral locking plate combined with the reamer-irrigator-aspirator (RIA) bone grafting technique for resistant distal femoral nonunion.
Methods
This retrospective observational study was performed from January 2018 to December 2021 and involved five patients who presented with resistant distal femoral nonunion despite undergoing several surgeries. They were treated with intramedullary nailing and a lateral locking plate combined with the RIA bone grafting technique. Postoperative follow-up was performed to observe the healing time, and functional outcomes were evaluated using the Lower Extremity Functional Scale (LEFS).
Results
After the patients had been monitored for a mean of 17.9 months, complete bone healing was observed in every patient (mean healing time of 4.8 months). Postoperative wound failure in an older patient was successfully treated with resuturing and nutritional assistance. At the last follow-up, the mean LEFS score was 71.2/80 and the mean knee flexion was 109 degrees.
Conclusions
Our study demonstrates that combining intramedullary nailing and a lateral locking plate with the RIA bone grafting technique enhances biological properties, provides good structural support, and achieves good union and functional results in the management of resistant nonunion of the distal femur.
Keywords
Introduction
Distal femoral fractures occur within 9 cm of the femoral condyle joint surface line and account for 0.4% of all fractures1,2 and 4% to 6% of all femoral fractures.2–5 Surgery is the preferred treatment because of its benefits over nonsurgical options.6–8 However, the nonunion rate for distal femoral fractures ranges from 5% to 10% after fixation. Despite adopting modern staged fixation methods, including implants and lateral fixation, the nonhealing rate of distal femoral fractures still ranges from 0% to 6%.9–12 This poses significant challenges for orthopedic surgeons in treating cases of resistant nonunion, which require at least two treatments and often lead to significant morbidity and poor functional outcomes. Additionally, insufficient bone stock, disuse osteopenia, joint contracture, and implant failure can make treating patients with resistant nonunion more difficult.10,11,13
Little research to date has focused on the management of resistant distal femoral nonunion, although several articles have described management techniques for distal femoral nonunion such as medial plate application, biological supplementation procedures, plating over an existing intramedullary nail, lateral fixation with an Ilizarov device, application of a combined nail/plate construct, and use of new prostheses with bone grafting.12–14 Resistant distal femoral nonunion is challenging to treat because it requires reconstruction of postsurgical structural flaws and improvement of the biology to promote fracture healing.13,15 In this study, we present five cases of successful treatment of resistant distal femoral nonunion with a combined nail/plate construct and the reamer-irrigator-aspirator (RIA) technique.
Patients and Methods
Clinical data
This retrospective observational study consecutively enrolled patients who were hospitalized at the 909th Hospital, Zhangzhou, China with a diagnosis of resistant distal femoral nonunion and treated with a combined nail/plate construct and the RIA technique. Written informed consent for treatment was obtained from all patients before surgery. The study protocol followed the Helsinki Declaration and ethical guidelines of the institutional research committee as revised in 2013. From January 2018 to December 2021, a nail/plate construct with the RIA technique was used to treat five patients who presented with resistant distal femoral nonunion, defined as nonunion after at least two fracture healing attempts. The study included four men and one woman with a mean age of 52 years (range, 22–74 years). All patients primarily had closed injuries; three were extra-articular, and two were intra-articular. Two patients underwent all treatment procedures at our hospital, and three patients were referred to our hospital for treatment after multiple surgical procedures had resulted in nonhealing. Table 1 shows the patients’ detailed clinical parameters, and Table 2 summarizes the patients’ medical history and treatment details. Clinical and blood investigations were performed to rule out infection. Written consent for publication of this report was obtained from the patient or caregiver, and the study was approved by the Ethics Committee of Xiamen University (2022-5621). We deidentified all patient details at the end of the study. The reporting of this study conforms to the STROBE guidelines. 16
Patients’ clinical parameters.
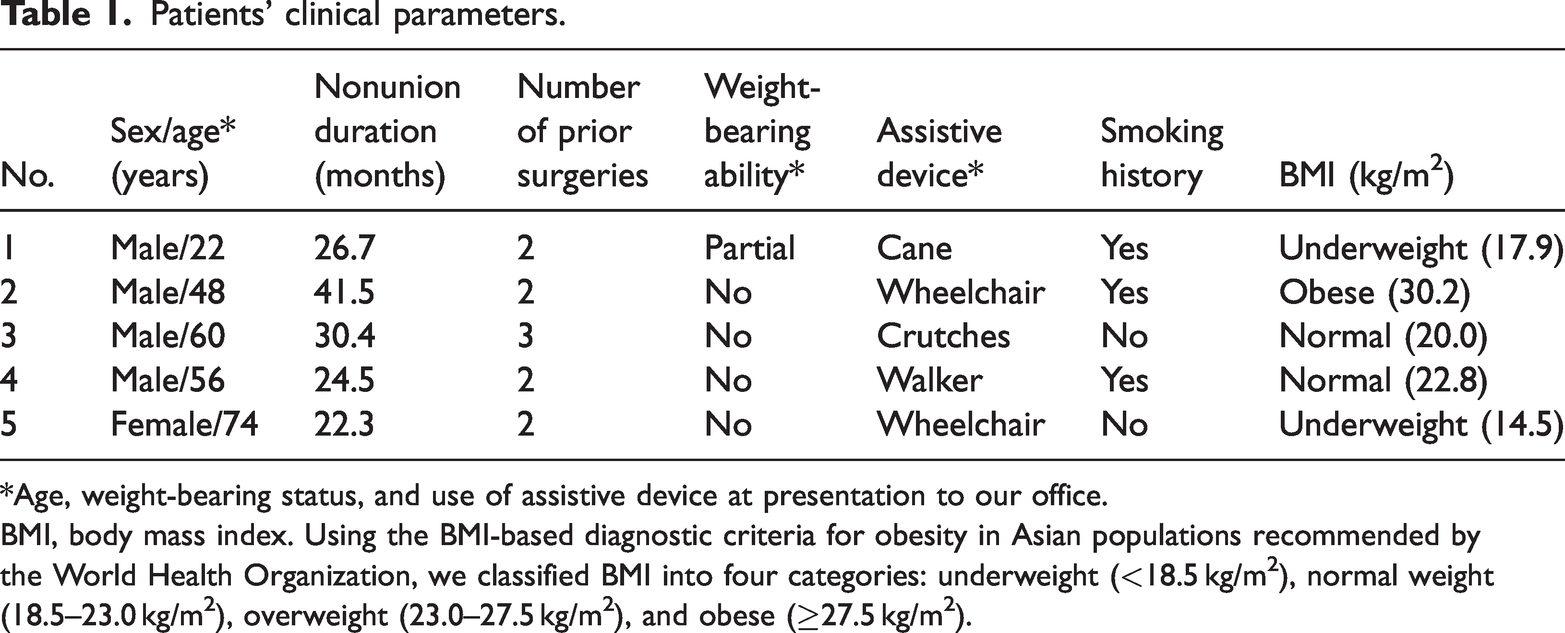
*Age, weight-bearing status, and use of assistive device at presentation to our office.
BMI, body mass index. Using the BMI-based diagnostic criteria for obesity in Asian populations recommended by the World Health Organization, we classified BMI into four categories: underweight (<18.5 kg/m2), normal weight (18.5–23.0 kg/m2), overweight (23.0–27.5 kg/m2), and obese (≥27.5 kg/m2).
Patients’ medical history and treatment details.
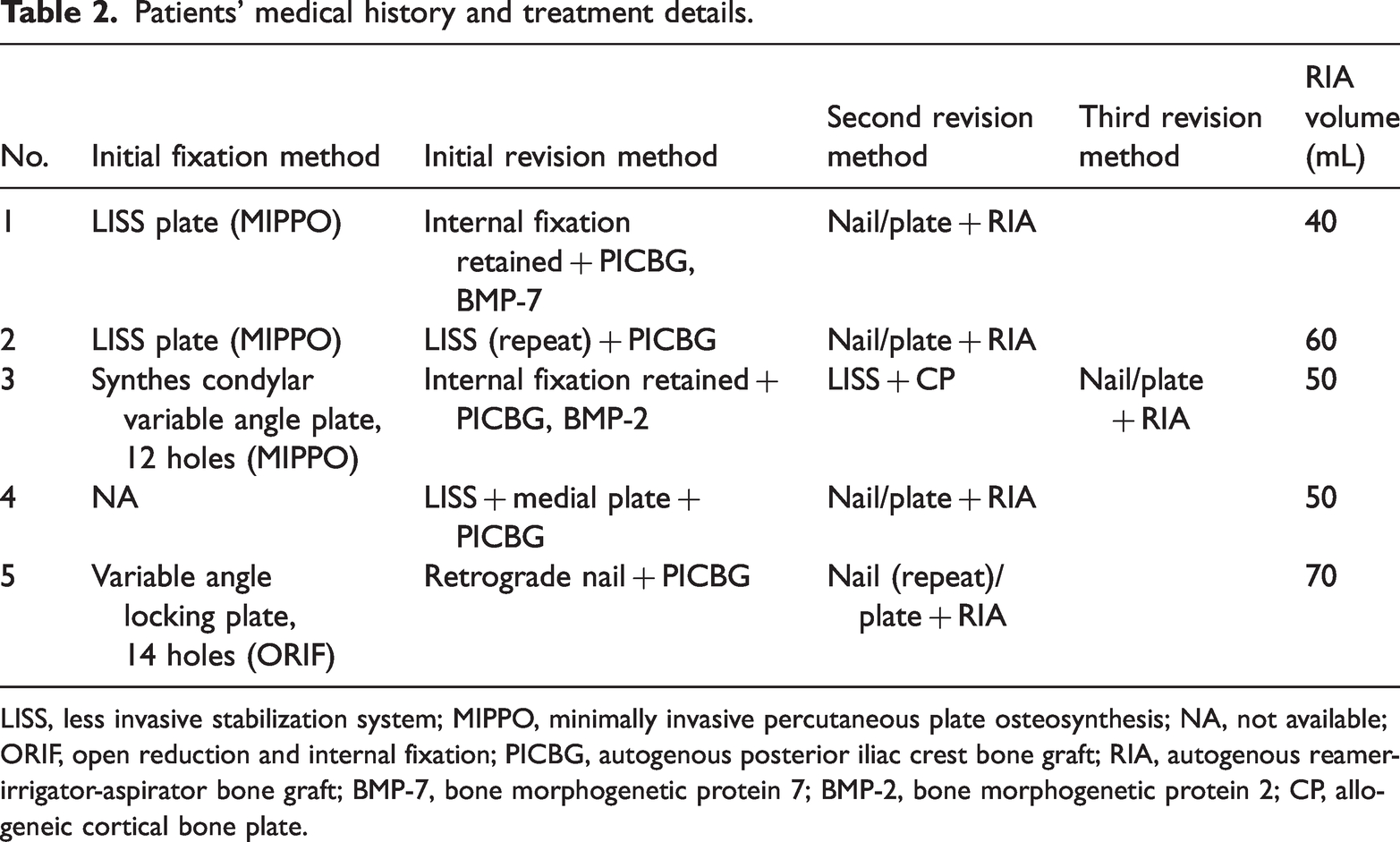
LISS, less invasive stabilization system; MIPPO, minimally invasive percutaneous plate osteosynthesis; NA, not available; ORIF, open reduction and internal fixation; PICBG, autogenous posterior iliac crest bone graft; RIA, autogenous reamer-irrigator-aspirator bone graft; BMP-7, bone morphogenetic protein 7; BMP-2, bone morphogenetic protein 2; CP, allogeneic cortical bone plate.
Surgical techniques
The patients were placed supine on a fluoroscopic surgical bed and received general or epidural anesthesia. First, the nonunion site was exposed using the same incision as in the previous surgery. The prior implant, fibrous scar tissue, and necrotic bone tissue at the fracture site were removed. Two Schanz nails were placed distal and proximal to the fracture, and limb alignment was corrected using bracing under fluoroscopy and compared with the healthy side. A locking plate was then placed on the lateral side of the femur, and three single cortical locking screws were inserted distally and proximally to maintain limb alignment and resist rotation. After restoring the anatomical axis, a retrograde intramedullary nail of appropriate length and diameter was implanted. An appropriately sized retrograde nail was selected according to the diameter of the femoral isthmus. If the retrograde intramedullary nail was hindered by the three proximal screws of the lateral locked plate, the length of the screws was reduced. Finally, an RIA system was used to collect the expanded medullary bone and implant it in the medial cortical defect area.
Results
Continuous passive motion was initiated on the second postoperative day and continued until the patients were able to bear weight. They were instructed to avoid weight-bearing for an average of 2.4 weeks, after which gradual weight-bearing was allowed. Regular follow-up visits were conducted to monitor bone union and assess functional outcomes.
All patients were followed up for a period of 10.5 to 36.0 months after surgery, with a mean follow-up time of 17.9 months. Solid bony union was observed in all cases, with a mean healing time of 4.8 months (range, 2.5–8.5 months). At the last follow-up, the mean knee flexion was 109 degrees (range, 80–130 degrees), and the patients had good functional outcomes with a mean Lower Extremity Functional Scale (LEFS) score of 71.2 (range, 59–80). Poor wound healing occurred in one older patient and was successfully treated with resuturing and nutritional support. At the end of the first year, all patients were able to perform all activities and had good functional outcomes. The surgical outcomes are presented in Table 3, and a typical case is illustrated in Figures 1 to 3 (Case 2).
Operative outcomes.

LEFS, Lower Extremity Functional Scale.
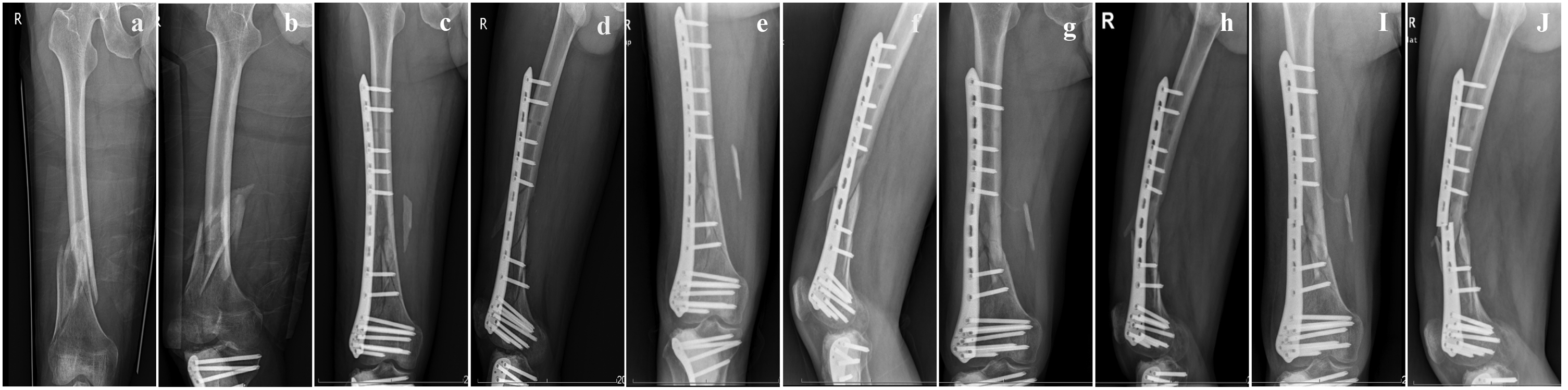
A 48-year-old man with a distal femoral fracture underwent surgery with less invasive stabilization system (LISS) plate fixation (Case 2). (a, b) Preoperative radiographs. (c, d) Radiographs taken 3 days after the operation. (e, f) Radiographs taken 2 months after the surgery, exhibiting a femoral varus deformity. (g, h) Five months after the operation, the femoral varus deformity was significantly worse and (i, j) Six months after the initial surgery, the plate broke.

The patient in Case 2 underwent the first revision surgery with a more extended LISS plate to correct the varus deformity and autogenous iliac bone grafting of the medial femoral defect. (a, b) Radiographs taken 3 days after the renovation. (c–f) Radiographs taken 3 and 6 months after the first revision surgery, revealing resorption of the autogenous iliac bone graft in the medial femoral cortex. (g, h) Radiographs taken 15 months after the first revision surgery, indicating nonunion of the distal femoral fracture that resulted in varus collapse, which caused the plate to break again and (i) Three-dimensional computed tomography scan of a bone defect of >2 cm in length on the medial-side metaphysis.

The patient in Case 2 underwent a second revision surgery with a nail/plate construct and the reamer-irrigator-aspirator technique. (a, b) Radiographs taken 5 days after the second revision surgery and (c–h) Radiographs taken 3, 6, and 9 months after the second revision surgery, revealing fracture union.
Discussion
Numerous surgical options are available for treating extra-articular fractures of the distal femur, and various studies have concluded that there is no discernible superiority among different fixation methods in terms of overall fracture healing rates.17–19 However, nonunion has emerged as the most common postoperative complication associated with distal femoral fractures. Although reported nonunion rates were <6% in the early literature, 8 recent studies have indicated that the rates can be as high as 17% to 21%. 6 Both iatrogenic and noniatrogenic factors contribute to nonunion. Noniatrogenic factors include age, osteoporosis, steroid use, diabetes, smoking, body mass index, comminuted fractures, open fractures, and fracture infection.20,21 In our patients, the mean body mass index was 21.1 kg/m2, which may not have been a significant factor in nonhealing. However, three of the five patients had a smoking history, suggesting that smoking may be a risk factor for nonunion. Iatrogenic factors include open surgery, inadequate medial structural support, use of stainless steel plates, a shorter plate working length, higher construct rigidity scores, and purely locking screw constructs.20,21 In our typical case (Figures 1–3), the initial surgery failed because of inadequate medial structural support, a short plate, higher construct rigidity scores, and a lower average number of unfilled holes adjacent to the fracture. Peschiera et al. 20 found that malreduction associated with unbalanced fixation and medial cortical defects, especially axillary defects, was the main risk factor for nonunion, and stated that structural support should be performed for medial defects of >2 cm in length. In our case, a significant structural defect was present in the medial femoral cortex after the initial surgery. Moreover, the plate length should be three times the fracture length, and the ratio of the number of screws to the number of nail holes in the plate should be 0.4 to 0.5. 8 However, this ratio in the initial surgery in our case was 0.76 (13/17). To address these problems, the initial revision surgery was performed by using a longer lateral locking plate, correcting the varus deformity, and applying autogenous iliac bone for bone grafting of the medial femoral defect. The patient also quit smoking and underwent strict bed rest. Unfortunately, the fracture still did not heal successfully. Our analysis suggests that inadequate medial structural support contributed to the second nonunion. Although an iliac bone graft was resected to fill the medial femoral defect, a medial-posterior structural defect of >2 cm and varus collapse were still visible on the postoperative computed tomography scan (Figure 2(i)). A distal femoral lateral locking plate is an eccentric fixation, and the titanium material has an elastic modulus. Thus, the variables and stresses of compression and bending are relatively small at the fracture end near the plate. However, the fractured end on the other side of the plate (medial femur) is affected by relatively large compressive and bending variables and stresses. In cases of insufficient structural support, the compressive and bending strength of lateral plate fixation alone is defective. Consequently, plate screws are prone to bending, loosening, or fracture.21–24
The management of nonunion in the absence of a unionized workforce focuses on the biological and structural support aspects of fracture union. Various therapeutic techniques have been reported to treat distal femoral nonunion. Varus collapse caused by distal femoral fracture nonunion is possible, given the mechanical axis of the lower extremity. This situation is perfectly suited to medial column support with plating, and medial plating is frequently used to supplement intact indwelling lateral fixation. One study revealed a 95% union rate in 22 patients with distal femoral nonunion after placement of a medial plate. 25 Biological supplementation procedures, such as the use of osteoconductive drugs, autogenous bone grafts, and/or bone graft substitutes, have also been employed. 26 Plating over an existing intramedullary nail is a reliable option for the treatment of metaphyseal and diaphyseal femoral fracture nonunion. In one study, this plate augmentation technique was used over a retained nail in 30 cases, including those involving the distal femur, and union was achieved in every case. 27 Another effective method for treating nonunion is lateral fixation using an Ilizarov device. In one study, a 100% union rate was achieved in cases involving complicated distal femoral fractures and nonunion. 28 Exchange nailing has much lower success rates than the above-mentioned methods for treating distal femoral nonunion. 29 If severe stiffness causes nonunion, switching to an intramedullary nail may be an alternate technique to promote secondary healing. 30 Distal femoral nonunion has also been treated using a nail/plate combination. A combination nail/plate construct with autogenous bone grafting was used in a study of 10 patients with distal femoral nonunion, and all patients achieved union following initial nonunion. 31 Another study achieved a 100% union rate (7 of 7 cases) when diaphyseal femoral fracture nonunion was treated with large fragmented compression plating and bone grafting following intramedullary nail fixation. 32
Treatment of resistant nonunion is a challenge for orthopedic surgeons because of complications such as low bone reserve, disuse osteoporosis, joint contracture, and internal fixation failure.13,15 Two key components need to be considered in addressing this issue: delivering structural support and improving biology. The combined nail/plate construct and RIA technique provide a solution to both. Before performing revision surgery, it is crucial to thoroughly evaluate the patient’s bone reserve, lower extremity alignment, and medial cortical defects to determine the most appropriate technique. In our study, we decided to use a combination of plating and nails to enhance axial loading, fracture alignment, nail reaming, and torsional force resistance. The combination of intramedullary nail fixation and a plate provides additional distal fragment fixation and stiffness, allowing patients to move without complications. Furthermore, this technique reduces the incidence of varus collapse and metaphyseal screw cutout, which commonly occur with intramedullary nailing. RIA bone grafts are bioactive materials that show great promise as an alternative to traditional iliac crest bone grafting. Several studies have supported the use of these bone grafts for treatment of nonunion, 33 and the patients in our study achieved substantial fracture healing at an average of 4.8 months after these modalities were applied. Furthermore, our patients had good functional outcomes with an average LEFS score of 71.2 and average knee flexion of 109 degrees.
In summary, we believe that for successful treatment of distal femoral fractures, it is crucial to perform meticulous initial fixation, choose an appropriate lateral plate length and number and distribution of screws, and achieve optimal repositioning and limb alignment during the operation. Moreover, factors associated with postoperative nonunion should be thoroughly evaluated to determine whether they are iatrogenic or noniatrogenic. After a diagnosis of nonunion, the revision method should be determined based on the patient’s bone reserve, fixation effectiveness, lower limb alignment, and bone defects. Patients should be closely monitored, and timely interventions such as medial plate or bone graft placement should be performed before lateral plate fixation failure.
This study had two main limitations. First, it was retrospective in nature and involved a small number of patients. Second, the diagnosis of union was based on a surgeon’s evaluation of radiographs. To further validate our findings, a long-term randomized controlled trial with a larger patient population and the inclusion of control groups and other revision methods should be conducted.
In conclusion, combining intramedullary nailing and a lateral locking plate with the RIA bone grafting technique enhances biological properties, provides good structural support, and achieves good union and functional outcomes in the management of resistant nonunion of the distal femur. Retrograde intramedullary nailing and a lateral locking plate combined with the RIA technique may be an alternative approach for patients with resistant nonunion.
Footnotes
Acknowledgements
We would like to thank all participants in this study for their enthusiasm, tireless work, and sustained support.
Author contributions
Jin-Hui Zhang: Writing the paper, data collection and analysis.
Hui Liu: Data collection.
Tao-Yi Cai: Writing the paper, data collection and analysis.
Yong-Zhi Lin: Searching related articles and data analysis.
JW: Data collection, performing surgeries, and managing the research team.
All authors have made significant contributions and approved the content of the manuscript. All listed authors meet the authorship criteria according to the latest guidelines of the International Committee of Medical Journal Editors, and all authors are in agreement with the manuscript.
Data availability statement
All data generated or analyzed during this study are included in this published article.
Declaration of competing interests
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. The paper is not based on a previous communication to a society or meeting.
Funding
This work was supported by a grant from the Logistics Research Project (20XSL21).