
Abstract
Objective
This study was performed to evaluate the clinical efficacy of endoscopic endonasal open reduction of fractures of the frontal process of the maxilla (FFPM).
Methods
We performed a retrospective study of patients who underwent endoscopic endonasal open reduction of FFPM from December 2013 to October 2018. The preoperative assessment included nasal endoscopy, computed tomography imaging, and three-dimensional craniofacial reconstruction. The clinical results were evaluated with a visual analog scale at 2 days and 1 year postoperatively.
Results
Thirty-two patients (25 male, 7 female) with an average age of 39 years were included in the study. All patients successfully underwent a surgical operation via the endoscopic endonasal approach with a nasal mucosal incision, and the nasal deformities were corrected. At the 1-year follow-up, six (18.8%) and 26 (81.2%) patients were somewhat satisfied and very satisfied with the aesthetic result, respectively, and five (15.6%) and 27 (84.4%) were somewhat satisfied and very satisfied with the functional result, respectively.
Conclusion
Endoscopic endonasal open reduction can be considered a reliable method for anatomical reduction of FFPM. This technology provides a viable choice for the treatment of FFPM.
Keywords
Introduction
The frontal process of the maxilla (FPM) is an irregularly shaped extension of the maxilla. 1 It is connected medially to the nasal bone by a fibrous aponeurosis, which is also the composite part of the complex structure of the nasal pyramid.2,3 Fractures of the FPM (FFPM) can cause severe facial deformities such as traumatic telecanthus.4,5 The FPM covers the anterior half of the lacrimal sac and contributes to the osseous part of the nasolacrimal duct.1,6 Therefore, severe FFPM have the potential to cause damage to adjacent structures, inducing ophthalmic diseases such as acute dacryocystitis. 7 FFPM may also be combined with nasal bone fractures (NBF).3,8 However, treatment of FFPM has been given less attention than treatment of NBF in the literature. 9
Traditionally, FFPM have been treated by open reduction through the lower lid approach and internal fixation with a wire or bone plate.8,10 However, these operations have some shortcomings, including increased trauma, facial scars, and a prolonged recovery time.
The treatment goals of facial fractures include visualization of anatomical reduction, elimination of deformity, restoration of physiological functions, and the absence of complications.11–13 The FPM is an essential part of the facial bone; therefore, the treatment of FFPM must also meet these criteria. To achieve this goal, we performed a minimally invasive procedure via the endoscopic endonasal approach for treatment of FFPM. In the present study, we evaluated the clinical outcomes of this surgical procedure for fracture reduction and the level of patient satisfaction with their facial profile after surgery.
Patients and methods
Patients
We retrospectively evaluated patients who presented to our hospital for treatment of FFPM from December 2013 to October 2018. FFPM were diagnosed based on a history of trauma and imaging examination findings. Patients with NBF or other facial bone fractures were excluded from the study. All patients included in the study underwent endonasal endoscopic open reduction. The preoperative evaluation included nasal endoscopy (Figure 1(a)), computed tomography (CT) imaging (Figure 2(a)–(c)), and three-dimensional craniofacial reconstruction (Figure 2(d)). This study was approved by the Ethics Committee of the Wuxi Huishan District People’s Hospital. Informed consent was obtained from all individual participants included in the study.

A 43-year-old man sustained a left fracture of the frontal process of the maxilla due to violence. The photographs in this figure show the endoscopic endonasal open reduction procedure. (a) Preoperative 0° endoscopic view showing a mucosal laceration (black arrow) in the superior anterior area of the lateral wall of the nasal cavity. (b) Intraoperative photograph showing the isolated fracture fragments. (c) Intraoperative photograph showing anatomical reduction with a linear fracture of the frontal process of the maxilla (black arrow). (d) Intraoperative photograph showing internal fixation with otological and craniocerebral glue.

A 53-year-old woman presented with a fracture of the frontal process of the maxilla caused by an impact injury at work. She underwent endoscopic endonasal open reduction of the fracture and attained good fracture reduction postoperatively. The green crossed lines and the black arrow show the site of the fracture. (a) Preoperative coronal computed tomography (CT) scan. (b) Preoperative sagittal CT scan. (c) Preoperative axial CT scan. (d) Preoperative three-dimensional CT reconstruction image. (e) Preoperative photograph showing a depressed nasal bridge. (f) Postoperative coronal CT scan. (g) Postoperative sagittal CT scan. (h) Postoperative axial CT scan. (i) Postoperative three-dimensional CT reconstruction image. (j) Postoperative photograph showing a well-corrected nasal bridge 2 days after surgery.
Surgical procedures
All patients were treated under local anesthesia. The procedures were conducted using a 4-mm-diameter rigid endoscope (Stryker Corporation, Kalamazoo, MI, USA) with a viewing angle of 30°. Video monitoring and recording were performed using a Visera Elite Video System (OTV-S190 video processor and CLV-190 light source; Olympus Medical Systems Corp., Tokyo, Japan). The patient was placed in the supine position on the operating table. The nasal cavity was prepared with 1% tetracaine and 1:1000 adrenaline on neurosurgical cottonoids for topical anesthesia and vasoconstriction. The cottonoids were placed in the nasal cavity two or three times for 10 minutes. The mucosa of the superior anterior area on the lateral wall of the nasal cavity was injected with 1% lidocaine and 1:100,000 adrenaline under endoscopic guidance. Additionally, the head of the middle turbinate was injected with the same solutions to block the branches of the anterior ethmoidal nerve and improve the effect of anesthesia and analgesia.
The procedure began with an arc incision in the nasal mucosa in the lateral wall of the nasal cavity. An incision was made from approximately 3 mm over the axilla of the middle turbinate to approximately 5 mm over the head of the inferior turbinate. The bone margin of the piriform aperture was exposed by stripping the mucoperiosteum with a 3-mm-wide elevator along the incision. The next step was to identify the fracture site. Elevation continued along with suction until the fracture site was visible (Figure 1(b)). With adequate exposure and visualization, the fracture fragments were reduced outward and upward by the elevator to achieve anatomical reduction (Figure 1(c), Figure 3). Cottonoids with local anesthetics were applied to the surgical area for 5 minutes to achieve hemostasis. The fractures and nasal mucosa were fixed with 0.3 mL of otological and craniocerebral glue (Guangzhou Baiyun Medical Adhesive Co., Ltd., Guangzhou, China) (Figure 1(d)). A 2-cm-long sponge (Ivalon®, Fabco, New London, CT, USA) was inserted into the anterior and superior clearances of the nasal cavity to provide pressure on the fractures. The nasal packing material was coated with tetracycline and cortisone acetate ointment to minimize the mucosal trauma and reduce mucosal edema. Intravenous antibiotics were administered postoperatively for 48 hours.
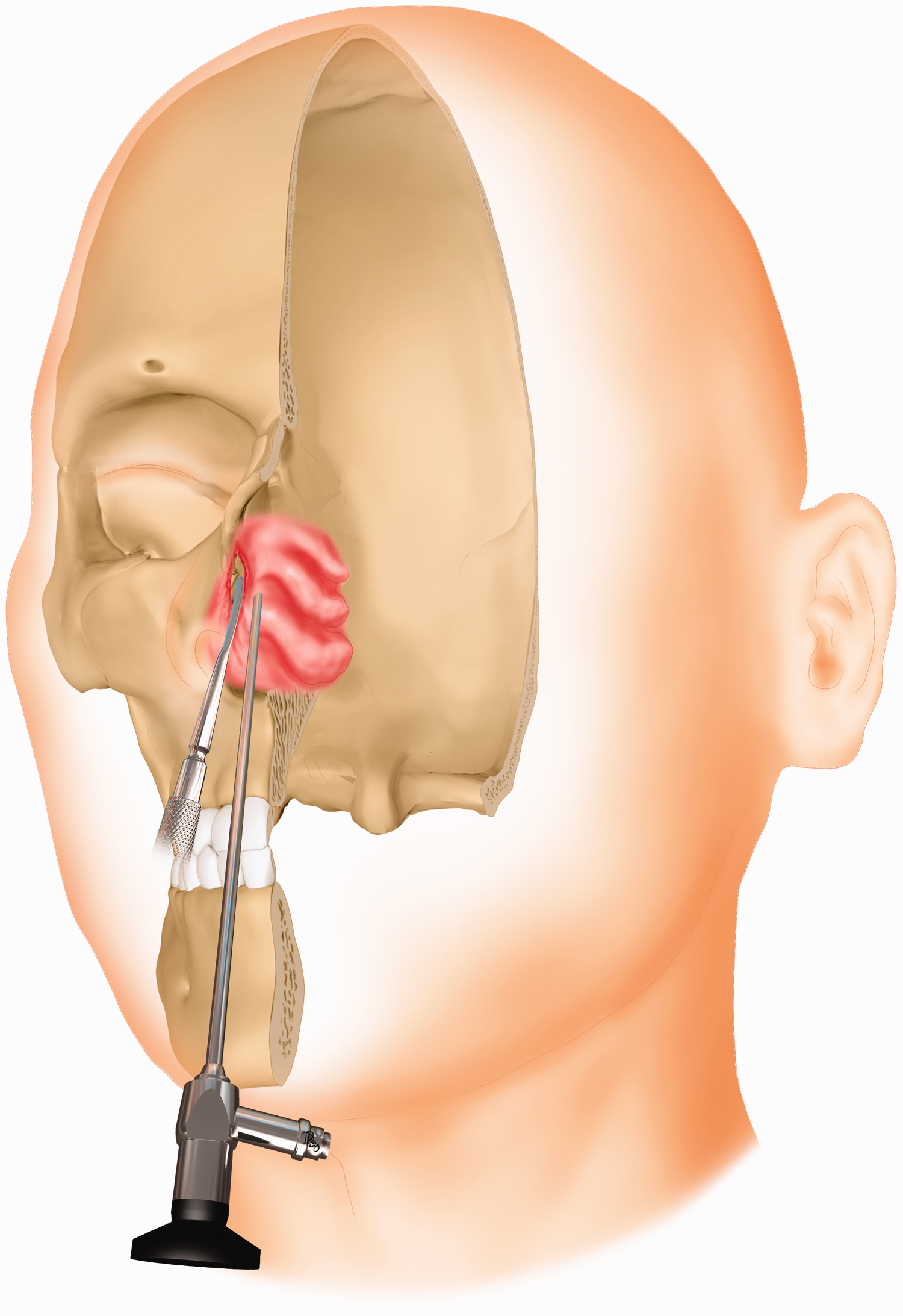
Illustration of endoscopic endonasal open reduction of a fracture of the frontal process of the maxilla through a nasal mucosal incision.
Postoperative evaluations
Two days postoperatively, the sponge was removed and an endoscopic examination was performed. CT was performed to assess the efficacy of the reduction (Figure 2(f)–(i)). The aesthetic and functional results of the nasal cavity were evaluated using a visual analog scale of 0 (worst) to 10 (excellent). The aesthetic result was based on the surgical deformity correction, and the functional result was based on nasal potency, olfactory function, humidification, and other conditions. The patients were asked to rate their overall satisfaction based on their feelings. Responses were defined as dissatisfied (score of <5), somewhat satisfied (score of 6–8), or very satisfied (score of >9). The patients were followed up regularly and reevaluated in the same way 1 year after the operation.
Results
Thirty-two patients with FFPM underwent endonasal endoscopic open reduction, and their nasal deformities were successfully corrected. The patients comprised 25 male and 7 female patients with an average age of 39 years (range, 17–62 years). The most common mechanism of injury was assault with a fist in 13 patients (40.6%), followed by work-related impact injuries in 11 patients (34.4%) and traffic accidents in 8 patients (25.0%). The injured site was on the left side in 21 patients (65.6%) and on the right side in 11 patients (34.4%). The most common clinical symptoms were nasal swelling, nasal obstruction, pain, nasal bleeding, and localized deformity. The time from trauma to surgery ranged from 5 to 10 days, with an average time of 7 days. All patients’ postoperative CT scans showed excellent anatomical reduction with no complications. The patients were dissatisfied (n = 0, 0.0%), somewhat satisfied (n = 9, 28.1%), and very satisfied (n = 23, 71.9%) with the aesthetic result and dissatisfied (n = 3, 9.4%), somewhat satisfied (n = 8, 25.0%), and very satisfied (n = 21, 65.6%) with the functional result.
After the patients had recovered the standard ventilation function of the nasal cavity, they experienced no nasal blockages or other uncomfortable nasal symptoms. At the 1-year follow-up, they were dissatisfied (n = 0, 0.0%), somewhat satisfied (n = 6, 18.8%), and very satisfied (n = 26, 81.2%) with the aesthetic result and dissatisfied (n = 0, 0.0%), somewhat satisfied (n = 5, 15.6%), and very satisfied (n = 27, 84.4%) with the functional result.
Discussion
In this paper, we retrospectively analyzed the results of endoscopic endonasal open reduction for FFPM. All patients achieved anatomical reduction. After the patients had recovered the standard ventilation function of the nasal cavity, they experienced no nasal blockages or other uncomfortable nasal symptoms. The patients were somewhat satisfied (18.8%) and very satisfied (81.2%) with the aesthetic outcome and somewhat satisfied (15.6%) and very satisfied (84.4%) with the functional result.
FFPM alone are poorly described in the literature; they are often mentioned along with an adjacent fracture site, such as the nasal bone or other facial bone.14,15 Hillstrom et al. 14 introduced the concept of medial maxillary fractures in 1991 and defined the upper border of the fracture within the FPM. Yoshioka et al. 15 recently revisited this idea and proposed that medial maxillary fractures are a particular type of nasomaxillary buttress fracture associated with the FPM and other surrounding structures. To the best of our knowledge, the literature contains no accurate reports of the epidemiology of FFPM.
FFPM are usually caused by blunt trauma. The mechanisms of injury in our series were assault, impact injury, and traffic accidents. The male predominance found in the present study is consistent with previously published reports. 16 Most patients were injured on the left side. All assault-induced injuries were present on the left side. This might have been associated with the right-handedness of the assailants. Work-related injuries were always caused by a heavy object such as a metal ball.
Reduction and fixation is a fundamental principle in FFPM surgery. Ellis 8 reduced and stabilized the fracture fragments of the FPM by rigid fixation using wires or bone plates through a lower lid incision or an existing laceration. Patients with markedly displaced canthal tendons were treated with repositioning technology of the FPM to correct the medial canthal deformity. 8 Based on principles similar to wire osteosynthesis, Jeter et al. 10 introduced an open reduction technique with mini-fragment bone plates for stabilization of FFPM. Open reduction and rigid fixation can achieve anatomic reduction. However, these techniques require an additional skin incision, which increases the degree of trauma. Endoscopic-assisted open reduction via a nasal mucosal incision can provide adequate exposure of the fracture with a minimal access approach. The camera system provides a unique surgical field of view with high resolution, facilitating observation of the tissue adjacent to the fracture. This procedure does not require an auxiliary facial incision, which avoids skin scarring. Additionally, otological and craniocerebral glue adhere to the fracture fragments within 30 seconds. Packing the nasal area with sponges can further strengthen the fixation effect to prevent fracture displacement.
All fractures in the present study were linear but comminuted fractures. The procedure is straightforward and can be completed by an experienced otolaryngologist within 30 minutes. Therefore, local anesthesia meets the operative analgesia requirements. Our patients did not appear to experience unbearable pain or discomfort during the operation under local anesthesia. In this way, we reduce the cost to patients.
Identifying the exact fracture site is critical to the success of the operation. We can roughly determine the fracture site based on the following guidelines. First, swelling, congestion, and lacerations are present in or near the local area of the nasal dorsum. This area is usually the fracture site. This site may be associated with collapse of the soft tissues during the early period of trauma. Second, routine endoscopic examinations can also provide clues to identifying the fracture site. When a mucosal tear, bleeding, and collapse occurs in the anterior region of the upper portion of the nasal wall, the fracture site may be located under the mucosa of this area. Third, CT imaging and postprocessing techniques can be used to determine the location, length, and direction of the fracture. With advances in imaging technology, CT can accurately identify the anatomical location of fractures. 8 We studied the patients’ axial, coronal, and sagittal CT images using both three-dimensional interactions and three-dimensional reconstruction images. Accurate recognition of specific imaging features can assist in the differential diagnosis of fractures of the anatomical unit.
The correct timing of surgery is an influential factor in the treatment effect. We performed surgery from 5 to 10 days after trauma, which is consistent with the reduction timing of NBF. 17 If the time from trauma to surgery is too short, the swelling and bleeding of the nasal cavity mucosa can interfere with the field of view, which will affect the operation. If the duration exceeds 10 days, surgical manipulations will become difficult because osteophyte formation and fibrotic adhesion may also affect fracture healing. 9
Open reduction of FFPM requires attention to several areas. Under normal circumstances, we select an arc incision in the anterior region of the lateral wall of the nasal cavity. If a nasal mucosal laceration is present in the fracture zone, we can flexibly amend the location and direction of the incision, allowing for quicker identification of the fracture fragments. When intraoperative localization is complicated, we can identify the fracture fragments using a pair of gun-shaped forceps. When placing one side of the forceps in the deformed area (collapse or laceration) on the lateral side of the nasal dorsum, the other side of the forceps contacts the lateral wall of the nasal cavity, which may be a fracture area.
The present study has some limitations. Because this was a single-center retrospective study, sample selection bias may have been present. Although this group of patients achieved a satisfactory therapeutic effect, the small sample size may have influenced the high success rate. Therefore, a large multicenter study is needed to verify the outcomes of this procedure. Furthermore, patients with FFPM involving NBF were not included in the study. In the future, we will improve the operational technology and broaden the clinical application.
Conclusion
The endoscopic endonasal open reduction described in the present study produced excellent exposure of FFPM. This technique provides an anatomical reduction of FFPM with an excellent cosmetic result and has the advantages of a simple process, a visualized operation, and feasibility in clinical practice. It provides an alternative for the minimally invasive treatment of FFPM.
Footnotes
Acknowledgements
The authors acknowledge all of the working staff of the Radiology Department of Wuxi Huishan District People’s Hospital for their help in the preoperative and postoperative image assessment.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.