
Abstract
Objective
To assess the association between neutrophil percentage-to-albumin ratio (NPAR) and 28-day mortality in severely ill Chinese patients with sepsis.
Methods
In this retrospective, single-centre study, sepsis patients admitted to the ICU of the Affiliated Hospital of Jining Medical University between May 2015 and December 2021 were retrospectively analysed. The relationship between NPAR and 28-day mortality was examined using Cox proportional-hazards model.
Results
In total, 741 patients with sepsis were included. Multivariate analysis, adjusted for age, sex, body mass index (BMI), smoking and alcohol drinking history, showed an association between elevated NPAR and a high risk of 28-day mortality. After removal of additional confounders, moderate and high NPAR values remained significantly associated with 28-day mortality in comparison with low NPAR values (tertile 2 vs 1: HR, 95% CI: 1.42, 1.06–1.90; tertile 3 vs 1: HR, 95% CI: 1.35, 1.00–1.82). Survival curves stratified by NPAR groups showed that high NPAR levels had lower survival probabilities than lower NPAR levels. Subgroup analysis did not show any significant interactions between NPAR and 28-day mortality.
Conclusions
Elevated NPAR values were linked to increased 28-day mortality in severely ill Chinese patients with sepsis. The findings require verification by large, prospective, multi-centre studies.
Introduction
Sepsis is a serious consequence of infection and is characterized by numerous physiological and biochemical aberrations. 1 Septic shock leads to multiple circulatory and metabolic disturbances and often death.2–4 According to guidelines established by the Surviving Sepsis Campaign (SSC), prompt administration of antibiotics are recommended to manage infection, fluid resuscitation should be initiated as early as possible, and vasopressor medications used as required to maintain an average arterial blood pressure (BP) of ≥65 mmHg. 5 In addition, the provision of adequate respiratory and nutritional support is crucial and the source of the infection should be identified and eliminated as soon as possible. 6 It has been reported that, despite adequate treatment progression of sepsis to septic shock is associated with an increase in mortality from 25% to 52%.7,8 This poor prognosis has encouraged research into the identification of risk factors that can be used to predict morbidity and mortality.9,10
Neutrophils have a key role in innate immunity, and neutrophil levels can reflect the severity of an infection in the body.11,12 Albumin is the most abundant plasma protein, and its levels are controlled by its rate of synthesis in the liver, the volume of blood distribution, and its catabolism and degradation.13,14 During Systemic Inflammatory Response Syndrome (SIRS), inflammation increases capillary permeability and escape of serum albumin, that leads to expansion of interstitial space and an increase in the distribution volume of albumin. 15 When albumin leaks out of the capillaries during SIRS, it can contribute to the development of oedema in the affected tissues. 16 Indeed, hypoalbuminemia can be caused by a variety of mechanisms including inflammation, malnutrition, oxidative stress, changes in colloid osmolarity, and/or liver failure.17,18
Recent studies have shown that the neutrophil percentage/albumin ratio (NPAR) is correlated with the prognosis of various diseases, including, acute kidney injury (AKI), stroke, cardiovascular disease, cardiogenic shock, and encephalitis.17–22 There have been few studies on the association between NPAR levels and mortality from all causes in patients with sepsis, 23 and as far as we know, none involving Chinese patients. Therefore, in this retrospective study, we investigated the association of NPAR levels on admission and 28-day mortality in Chinese patients with sepsis admitted to ICU.
Methods
Study population and definition of NPAR
This was a retrospective cohort study. Patients with sepsis who had been admitted to the ICU of the Affiliated Hospital of Jining Medical University between May 2015 and December 2021 were identified. The diagnosis of sepsis was consistent with the Sepsis-3 definition, (i.e., patients with documented or suspected infection and an acute change in total Sequential Organ Failure Assessment (SOFA) score ≥2 points). 1 Eligible patients were ≥18 years of age with a confirmed diagnosis of sepsis. Patients with no measurements of neutrophil percentages or albumin levels during their ICU hospitalization, those with cancer, haematological malignancies, virus infection, and/or ≥10% missing data were excluded from the study. NPAR was calculated as neutrophil percentage divided by serum albumin concentration. Neutrophil percentage and serum albumin concentration were obtained from the first blood test following admission to ICU and were measured at the same time. The reporting of this study conforms to STROBE guidelines, 24 and was approved by the Medical Ethics Committee of Affiliated Hospital of Jining Medical University (2020C018). Written/verbal consent was not required because it was a retrospective study and patient data were anonymized prior to analysis.
Data collection
Patients’ data were obtained from the hospital’s electronic medical records. Demographic, clinical, and laboratory data, as well as information on comorbidities and death were extracted. The laboratory data included measurements of: neutrophils; albumin; creatinine; brain natriuretic peptide (BNP); C-reactive protein (CRP); total bilirubin; alkaline phosphatase; blood urea nitrogen (BUN); lactate; platelets (PLT); white blood cell (WBC); prothrombin time (PT); activated partial thromboplastin time (APTT); fibrinogen; serum uric acid; β2 microglobulin. SOFA scores and Acute Physiology and Chronic Health Score II (APACHE II) scores were assessed for each patient. The patients’ age, sex, body mass index (BMI), mean blood pressure (MBP), body temperature, heart rate, oxygenation index, renal replacement therapy, noradrenaline use, and length of ICU stay were recorded. All baseline information was obtained during the first 24 h of ICU stay. The endpoint of the study was 28-day mortality.
Statistical analysis
All analyses were performed using the R statistical software package (http://www.R-project.org, The R Foundation for Statistical Computing, Vienna, Austria), EmpowerStats (http://www.empowerstats.com, X&Y Solution, Inc., Boston, MA, USA) and Free Statistics software versions 1.5. All tests were two-sided and statistical significance was set at P < 0.05.
Referring to previous literature, the study participants were separated into three groups based on their NPAR values at baseline (tertile 1: <2.75 [low]; tertile 2: ≥2.75, <3.38 [medium]; tertile 3: ≥3.38 [high]), 14,23 Baseline characteristics were stratified by NPAR tertiles.19,25 Continuous variables were expressed as mean ± SD or medians and interquartile ranges (IQR), and differences were analysed using one-way ANOVA (data with normal distributions) and Kruskal-Wallis tests (data with skewed distributions). Categorical variables were represented as numbers and percentages and were analysed using χ2 tests. Cox proportional-hazard models were applied for the examination of NPAR-mortality association. Multivariate analysis results were shown as hazard ratios (HRs) with 95% confidence intervals (CIs) and tertile 1 group served as the reference group.
The associations of NPAR and 28-day mortality were fitted and presented as smoothing splines using generalized additive models. Kaplan-Meier methods were used for survival curve plotting. Survival differences between groups were compared using the log-rank test. Interaction and subgroup analyses were also performed to investigate the association between the NPAR and 28-day mortality according to age, sex, smoking, alcohol drinking history, BMI, APACHE II scores, SOFA scores, noradrenaline use, mechanical ventilation, and lactate levels.
Results
Patient characteristics
Of the 1000 patients identified, 741 patients with sepsis were included (Figure 1). Their characteristics stratified according to NPAR tertiles are listed in Table 1. Each group included 247 patients. Overall mean ± SD age was 65 ± 16 years and 445 (60%) of patients were male. The high-NPAR tertile had lower rates of hypertension, MBP, BMI albumin and urinary tract infections compared with the other two groups, but higher rates of soft tissue infections, and higher values for WBC, neutrophils, CRP, PT, APTT and 28-day mortality.
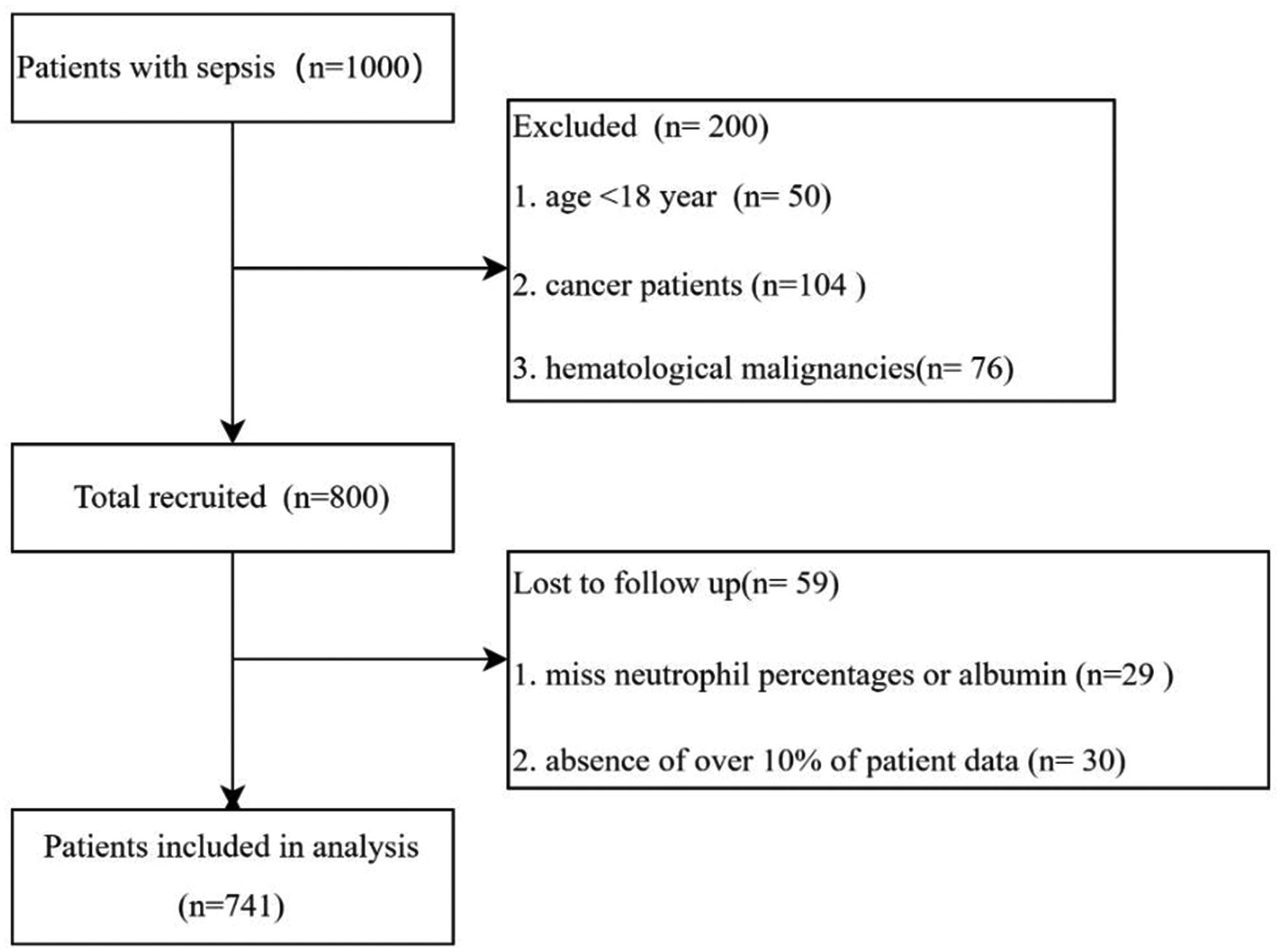
Flow chart of study population.
Characteristics of study patients by neutrophil percentage-to-albumin ratio (NPAR) tertiles.

Data are expressed as, mean ± standard deviation, median (interquartile range), or n (%).
AKI, acute kidney injury; ALT, alanine aminotransferase; APACHE II, Acute Physiology and Chronic Health Score II; APTT, activated partial thromboplastin time; BMI, body mass index; BNP, Brain natriuretic peptide; BUN, blood urea nitrogen; COPD, chronic obstructive pulmonary disease; CRP, C-reactive protein; CRRT, continuous renal replacement therapy; FiO2, fraction of inspiratory oxygen concentration; ICU, intensive care unit; LOS, length of stay; MBP, mean blood pressure; NPAR, neutrophil percentage-to-albumin ratio; ns, not statistically significant; PaO2, partial pressure of oxygen in arterial blood; PCT, procalcitonin; PLT, platelets; PT, prothrombin time; SOFA, sequential organ failure assessment score; TBIL, total bilirubin; WBC, white blood cells.
NPAR and mortality
We used multivariate analysis to examine associations between NPAR and 28-day mortality (Table 2). Model I showed that raised NPAR values were linked with an elevated risk of mortality after correction for age, sex, BMI, and smoking and alcohol drinking history. Model II applied adjustments for: age; sex; BMI; smoking; alcohol drinking history; APACHE II scores; SOFA scores; heart rate; PAO2/FIO2 (partial pressure of oxygen in arterial blood/ fraction of inspiratory oxygen concentration); MBP; lactate; temperature; PLT; PT; APTT; BUN; fibrinogen; mechanical ventilation; noradrenaline use; infection (i.e., soft tissue, lung, abdominal, urinary tract, bloodstream); hypertension; creatinine; β2 microglobulin. There was a significant association between moderate and high NPAR values and 28-day mortality (tertile 2 vs 1: HR, 95% CI: 1.42, 1.06–1.90, P = 0.019; tertile 3 vs 1: HR, 95% CI: 1.35, 1.00–1.82, P = 0.0478).
The association between 28-day mortality and neutrophil percentage-to-albumin ratio (NPAR).
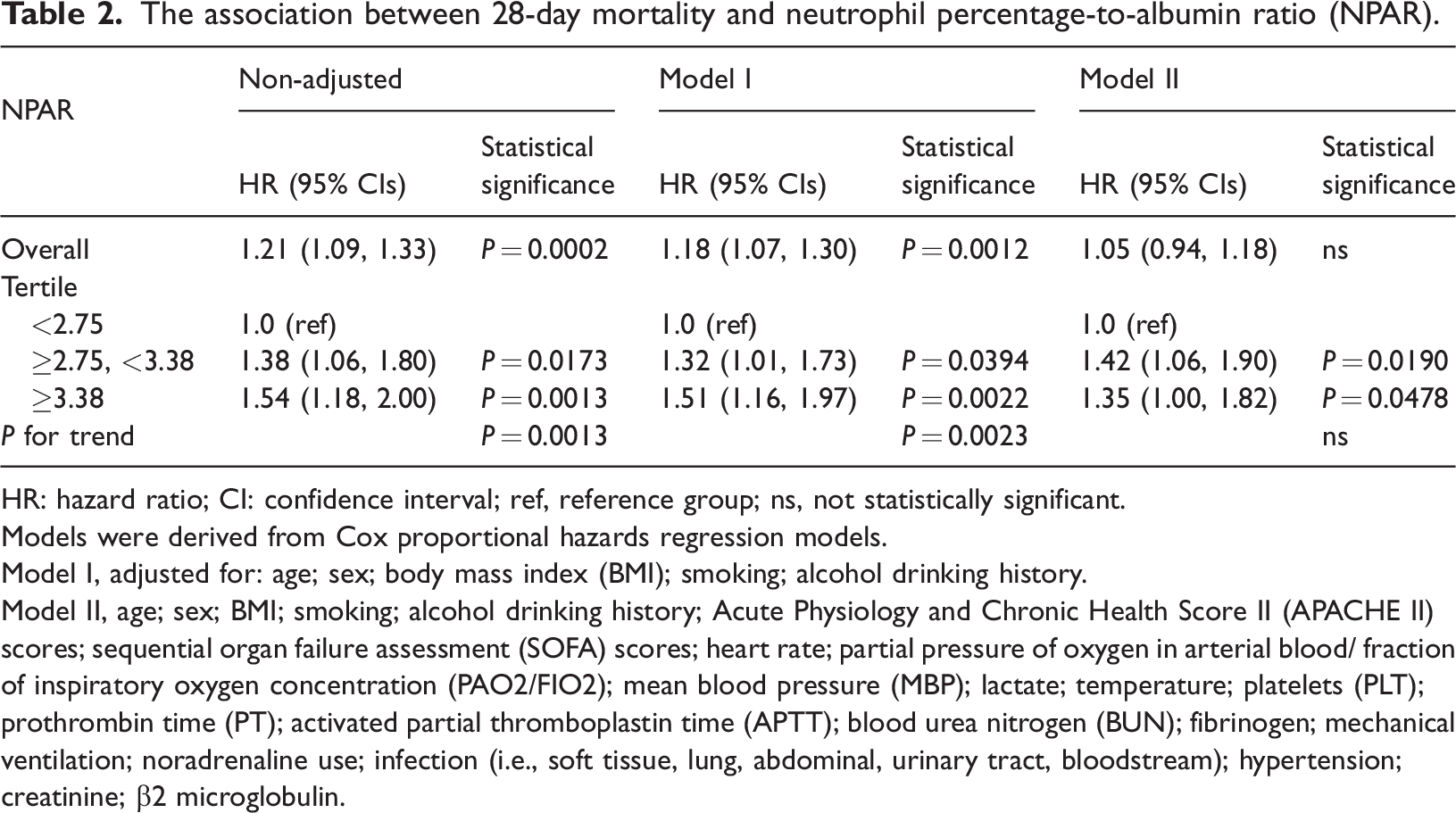
HR: hazard ratio; CI: confidence interval; ref, reference group; ns, not statistically significant.
Models were derived from Cox proportional hazards regression models.
Model I, adjusted for: age; sex; body mass index (BMI); smoking; alcohol drinking history.
Model II, age; sex; BMI; smoking; alcohol drinking history; Acute Physiology and Chronic Health Score II (APACHE II) scores; sequential organ failure assessment (SOFA) scores; heart rate; partial pressure of oxygen in arterial blood/ fraction of inspiratory oxygen concentration (PAO2/FIO2); mean blood pressure (MBP); lactate; temperature; platelets (PLT); prothrombin time (PT); activated partial thromboplastin time (APTT); blood urea nitrogen (BUN); fibrinogen; mechanical ventilation; noradrenaline use; infection (i.e., soft tissue, lung, abdominal, urinary tract, bloodstream); hypertension; creatinine; β2 microglobulin.
Smooth line analysis of the generalized additive model showed a linear relationship between NPAR and 28-day mortality (Figure 2).

Association of neutrophil percentage-to-albumin ratio (NPAR) with 28-day mortality. Smoothing splines were generated by generalized additive models.
Among the 741 patients with sepsis, 49% (363/741) died during the 28-day follow-up period (Table 1, Figure 3). Significantly (P = 0.026) more patients died in tertile 3 (57%) compared with tertile 2 (49%) and tertile 1 (41%). Kaplan-Meier curves for the low, medium, and high NPAR groups showed that a higher NPAR was significantly associated with an enhanced risk of 28-day mortality compared with other NPAR groups (log-rank test: P = 0:011 for all clinical outcomes) (Figure 3). Analysis of subgroups did not show any significant interaction between NPAR and 28-day mortality (Table 3).

Kaplan–Meier analysis of 28-day survival according to neutrophil percentage-to-albumin ratio (NPAR) group.
Subgroup analysis of the associations between 28-day mortality and neutrophil percentage-to-albumin ratio (NPAR).

HR: hazard ratio; CI: confidence interval; BMI: body mass index; SOFA: sequential organ failure assessment score; APACHE II: Acute Physiology and Chronic Health Score II scores; SOFA, sequential organ failure assessment score; ns, not statistically significant.
Discussion
To our knowledge, this is the first report demonstrating an association between NPAR values and 28-day mortality in Chinese patients with sepsis. This study showed that high NPAR values were related to increased mortality in patients with sepsis after adjusting for age, sex, BMI, smoking and alcohol drinking history. This relationship remained significant after adjusting for other potentially confounding factors. Smooth line analysis of the generalized additive model showed a linear relationship between NPAR and 28-day mortality. Kaplan-Meier curves showed that a higher NPAR was significantly associated with an enhanced risk of 28-day mortality compared with lower NPAR values. The subgroup analysis did not show any obvious interactions that affected the association between NPAR and 28-day mortality.
Our findings are similar to those from a study using data from MIMIC-III database which was derived from approximately 40,000 critical care patients at the Beth Israel Deaconess Medical Centre (Boston, USA) registered from 2001 to 2012.23,27 The authors of that retrospective study concluded that by comparison with low and medium NPAR groups, the higher NPAR group was associated with increased risk of all-cause mortality in critically ill patients with severe sepsis or septic shock. However, the MIMIC-III database had used an old definition of sepsis and only included US population. By contrast, our data were derived from patients admitted to an ICU unit in China between May 2015 and December 2021 and we used the most recent definition of sepsis for our diagnostic criteria (sepsis 3.0).1,26
Neutrophils are vital to the systemic inflammatory response to infection and are key cellular components of the innate immune system.28–30 In addition to their role as an immune cell mediator, neutrophils have other important roles during infection; 31 they are closely involved in immune thrombosis and septic shock-induced coagulopathy.32,33 Serum albumin levels are a reflection of both nutritional status and organ function, 34 with inflammation leading to reduced hepatic secretion of albumin and increased production of pro-inflammatory factors, resulting in hypoalbuminemia during the early stages of sepsis.35–38 The use of the neutrophil-albumin ratio as an inflammatory biomarker has been proposed in several previous studies.19,23,39 Moreover, in developing countries, where the management of patients with sepsis is affected by disproportionate medical resources, 40 the monitoring of neutrophil percentage and albumin would be fast, simple, and inexpensive. Monitoring NPAR, would help clinicians monitor the progress of their patients with sepsis.
The study had some limitations. For example, it was a single-centre, retrospective study and so selection bias may have occurred. In addition, NPAR assessments were based on data collected on admission and were not re-assessed during the patients’ stay in ICU. Furthermore, despite the use of multivariate analysis for controlling bias, it was possible that other potential confounding factors were present. Therefore, to substantiate our findings, further prospective. multi-centre studies are required. In conclusion, we found that elevated NPAR values were linked with an increased risk of 28-day mortality in patients with sepsis. Mores studies are required to verify our results.
Supplemental Material
sj-pdf-1-imr-10.1177_03000605231178512 - Supplemental material for Association between neutrophil percentage-to-albumin ratio and 28-day mortality in Chinese patients with sepsis
Supplemental material, sj-pdf-1-imr-10.1177_03000605231178512 for Association between neutrophil percentage-to-albumin ratio and 28-day mortality in Chinese patients with sepsis by Chunying Hu, Yinyan He, Jinfeng Li, Cuicui Zhang, Qinghe Hu, Wei Li and Cuiping Hao in Journal of International Medical Research
Supplemental Material
sj-pdf-2-imr-10.1177_03000605231178512 - Supplemental material for Association between neutrophil percentage-to-albumin ratio and 28-day mortality in Chinese patients with sepsis
Supplemental material, sj-pdf-2-imr-10.1177_03000605231178512 for Association between neutrophil percentage-to-albumin ratio and 28-day mortality in Chinese patients with sepsis by Chunying Hu, Yinyan He, Jinfeng Li, Cuicui Zhang, Qinghe Hu, Wei Li and Cuiping Hao in Journal of International Medical Research
Footnotes
Acknowledgments
We thank all the study participants and clinical staff for their support and contribution to this project.
Declaration of conflicting interests
The authors declare that there are no conflicts of interest.
Funding
This research was supported by the Shandong Medical and Health Science and Technology Development Project (grants No. 2018WSB34007) and Development Program Soft Science Project of Shandong Province of Shandong Province (grants No.2021JNZC016).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.