
Abstract
Alveolar adenoma is an extremely rare and benign pulmonary neoplasm; it is always asymptomatic and is usually detected incidentally on routine chest X-radiography. Typically on imaging examinations, alveolar adenoma exhibits as a peripheral, solitary, cystic nodule in the lung, which may easily imitate other lung lesions, consequently leading to difficulties in the differential diagnosis of this condition. Surgical resection is the primary treatment option. The diagnosis of alveolar adenoma is mainly based on postoperative histopathology, with features of proliferative type 2 alveolar epithelial cells and septal mesenchyme. The present case was a 60-year-old woman with alveolar adenoma, combined with systemic mutifocal cystic lesions. She underwent surgery following the obvious enlargement of this mass and a cystic nodule 7 cm in maximum diameter was resected. Postoperative histopathology confirmed a diagnosis of alveolar adenoma; her prognosis was favourable. In addition to reporting a rare case of alveolar adenoma coexisting with multifocal cysts, the English-language literature was reviewed for similar cases of alveolar adenoma.
Introduction
Alveolar adenoma is a rare pulmonary disease of uncertain histogenesis. Few sporadic cases have been reported since its first description in 1986. 1 Alveolar adenoma represents a type of pulmonary adenoma, according to the World Health Organization histological classification of lung tumours. 2 Other types of pulmonary adenoma include papillary adenoma, adenomas of salivary gland type (such as mucous gland adenoma or pleomorphic adenoma) and mucinous cystadenoma. 2 Alveolar adenoma typically presents as a solitary, circumscribed and peripheral nodule ,composed of a network of cystic spaces lined by type 2 alveolar epithelial cells. 3 Most patients are asymptomatic and are diagnosed incidentally on routine chest X-radiography. 4 Alveolar adenoma represents a slow-growing benign neoplasm with a good prognosis. 4 The current report presents a case of alveolar adenoma combined with multifocal cysts, along with a review of the relevant English-language literature on alveolar adenoma.
Case report
Approval for the publication of this case report was obtained from the Committee on Ethics of Biomedicine Research, The Second Military Medical University, Shanghai, China. Written informed consent was obtained from the patient concerned.
A 60-year-old woman presented to the Department of Thoracic Surgery in Changzheng Hospital, Shanghai, China, in May 2012. She informed the doctors that she had a 10-year history of a pulmonary mass of the right lung, with a diameter of ∼6 cm at initial diagnosis; the mass had shown enlargement on a recent chest X-radiography. At initial diagnosis, the patient was asymptomatic in terms of the respiratory system, therefore she received no treatment. In the only follow-up visit, which took place ∼3 months before admission to the study hospital, computed tomography (CT) of the patient’s lung had been undertaken at the outpatient clinic of the Department of Respiratory Medicine, at a local hospital in Hongkou District. This examination showed that the mass had increased in size from her initial diagnosis, and was now ∼7 cm in maximum diameter.
The patient had a history of hypertension (2 years), type 2 diabetes (1 year), and left renal calculus (1 month) before admission to the authors’ hospital. She had been receiving 0.15 g irbesartan (once daily, orally, for 2 years) and 0.1 g acarbose (three times daily, orally, for 1 year) for the treatment of her hypertension and diabetes, respectively; her blood pressure and blood glucose levels were well controlled. The patient did not smoke and reported no family history of smoking or lung disease. The patient also had no family history of polycystic disease, such as polycystic kidney disease. Her physical examination was unremarkable. Routine urine analyses, (which included white and red blood cell counts, and protein, creatinine and urea nitrogen levels) were all within normal range. Chest X-radiography showed a nodular opacity in the right lower lobe, near the spine. Magnetic resonance imaging (MRI) of the chest and abdomen revealed a well-circumscribed solitary pulmonary nodule in the right lower lobe, with a maximum diameter of ∼7 cm. The nodule showed low-signal intensity on T1-weighted MRI (Figure 1A), high-signal intensity on T2-weighted MRI (Figure 1B), and thin rim-enhancement on gadolinium-enhanced T1-weighted MRI (Figure 1C), all of which are characteristic of cysts. In addition, MRI revealed other cysts involving multiple organs, including a 2-cm cyst in the right breast (Figure 1D), a 1.5-cm cyst in the right lobe of the liver (Figure 1E), and several small cysts in the left kidney (Figure 1F).
Magnetic resonance imaging (MRI) findings for a 60-year-old female with alveolar adenoma in the right lung, combined with systemic mutifocal cystic lesions. Lung MRI demonstrated a well-circumscribed solitary pulmonary nodule in the right lower lobe with a maximum diameter of ∼7 cm: the lesion was: (A) in low-signal intensity on a T1-weighted image; (B) in high-signal intensity on a T2-weighted image; showing (C) thin rim-enhancement on a gadolinium-enhanced T1-weighted image. Systemic cysts involving other organs: (D) 2-cm cyst in the right breast on a T2-weighted image (black arrow); (E) 1.5-cm cyst in the right lobe of the liver on a T2-weighted image (white arrow); (F) multiple cysts in the left kidney on a T2-weighted image (black arrow).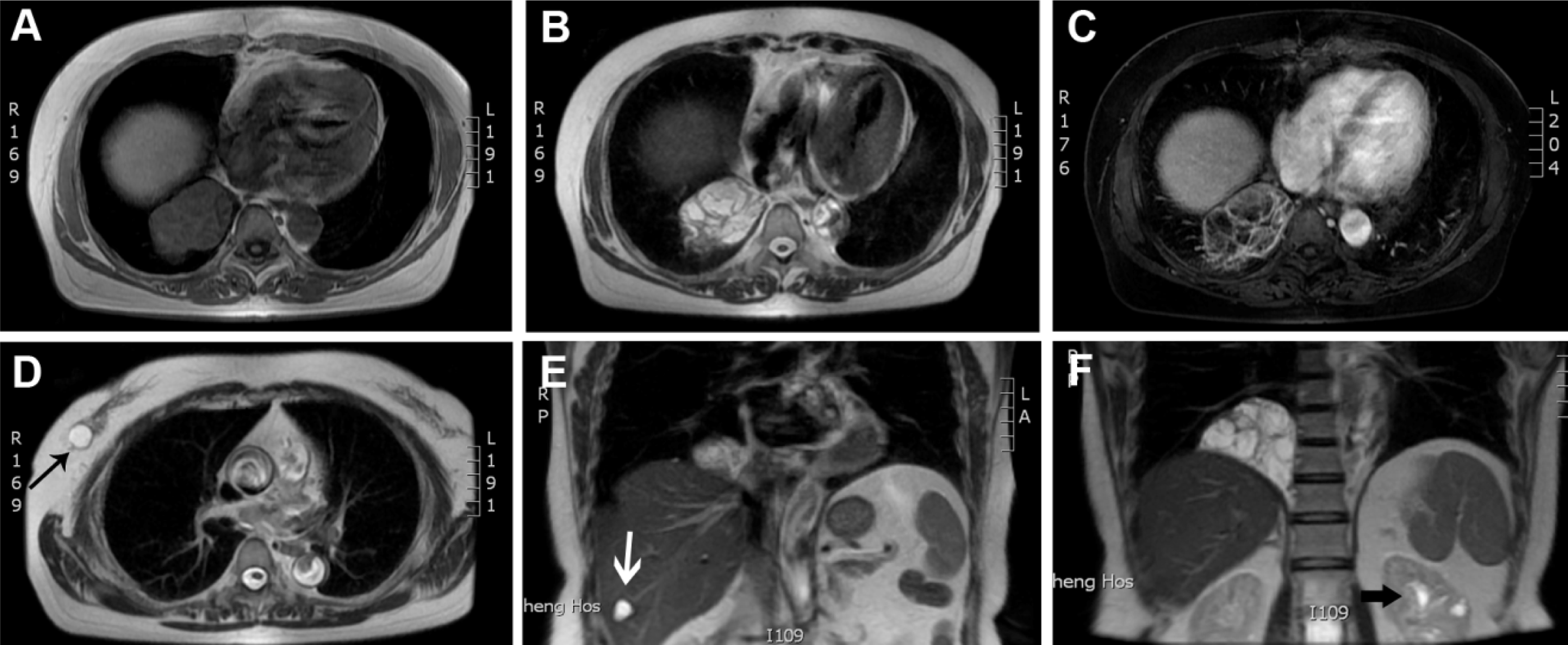
Considering the apparent enlargement of the pulmonary nodule and its uncertain histopathology, the patient was referred for surgical excision of the mass 3 days after admission, and a huge cyst in the right lower lobe of the lung was removed by thoracotomy. During surgery, a biopsy was taken and immediately underwent cryosection and histological analysis, which revealed a benign lesion with cystic spaces. Following this procedure, a wedge resection of the right lower lobe with the cystic mass was performed. Resected tissues contained a yellowish, soft, globular mass measuring ∼7 cm in diameter that was well circumscribed from the surrounding lung parenchyma (Figure 2A). The surgical procedure and the postoperative course were uneventful. The patient was discharged 1 week after surgery and remained in good condition at follow up, 6 months after surgery.
Pathological findings for a 60-year-old female with alveolar adenoma of the right lung combined with systemic mutifocal cystic lesions. (A) Gross surgical specimen (∼7 cm maximum diameter) showing a well-demarcated multicystic lesion from the right lung. Histology (haematoxylin and eosin staining) of well-demarcated and multicystic lesions of the right lung: (B) × 40 original magnification; (C) × 100 original magnification; (D) alveolar spaces lined by hyperplastic, cuboldal type 2 pneumocytes and intra-alveolar eosinophilic granular material – the interstitial stroma consists of abundant myxoid connective tissue with prominent spindle-shaped cells (×400 origtinal magnification). Immunohistochemistry staining showing positive staining of: (E) thyroid transcription factor-1 in epithelial cells lining the cysts; (F) epithelial membrane antigen in the epithelial cells lining the cysts; (G) vimentin in the vascular endothelial cells in the mesenchymal elements; (H) smooth muscle antigen) in mesenchymal elements; (I) CD31 in vascular endothelial cells scattered in mesenchymal elements; × 100 original magnification; scale bars, 100 µm.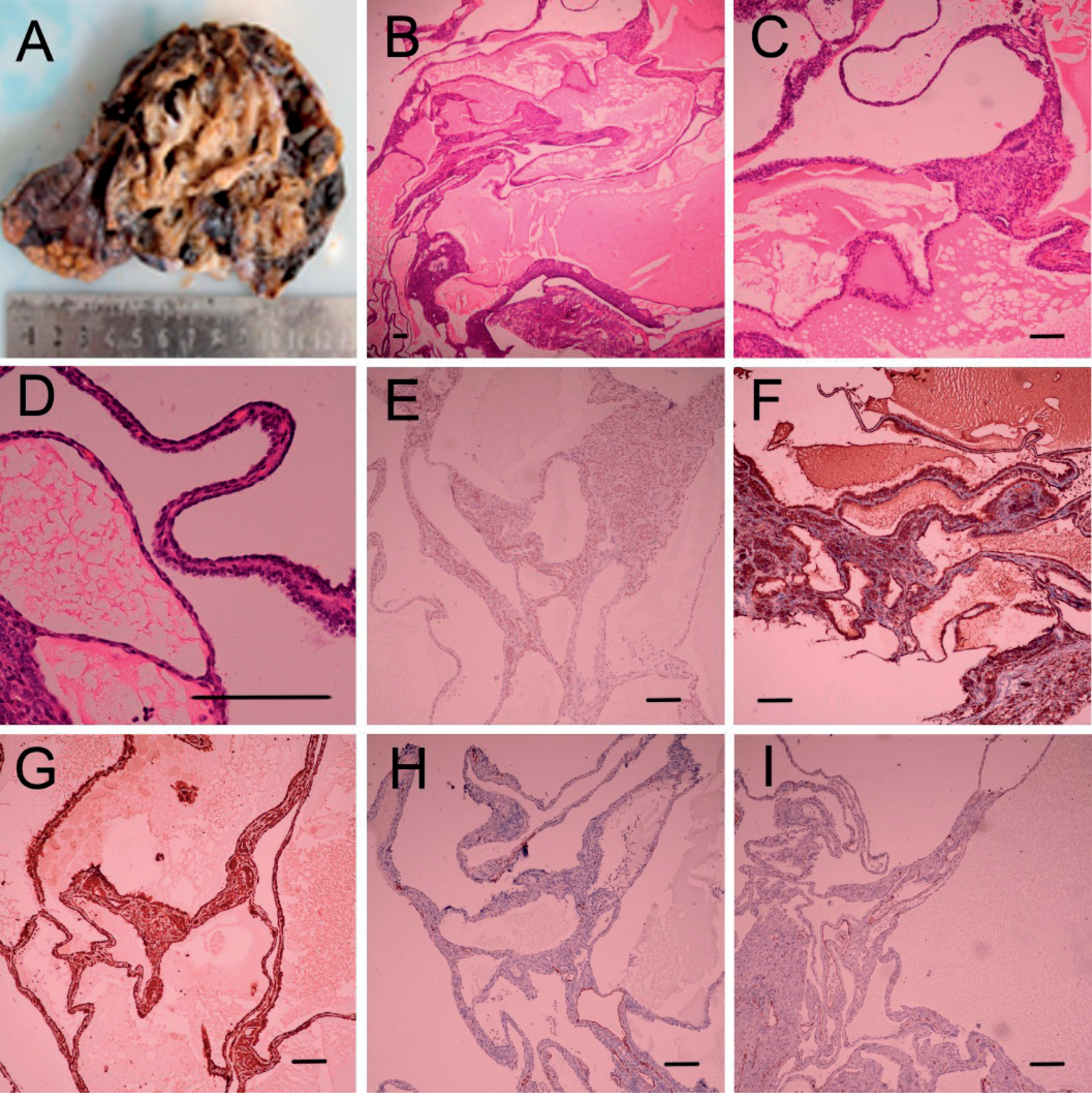
The biopsied specimen was fixed in buffered formalin (10%, pH 7.0), subjected to routine paraffin-wax embedding and sectioning (5-µm thick sections), and stained with haematoxylin and eosin. Histopathological analysis showed that the mass was well-demarcated and multicystic, with spaces filled with eosinophilic granular material and some foamy macrophages (Figures 2B and 2C). The cystic spaces were lined with a single layer of neoplastic epithelial cells, mainly comprising cuboidal or hobnail-shaped type 2 pneumocytes. No nuclear atypia, mitosis or invasive growth was revealed in these cells. Neither ciliated nor Clara cells were observed in the inner layer of the cystic spaces (Figure 2D).
Immunohistochemical analysis of sections, prepared as described above, showed that the neoplastic epithelial cells were diffusely positive for thyroid transcription factor-1 (TTF-1; Figure 2E) and epithelial membrane antigen (Figure 2F), which both suggested that the tumour was an alveolar adenoma that originated from type 2 alveolar epithelial cells. The mesenchymal elements were focally positive for vitenmin (Figure 2G) and smooth muscle antigen (Figure 2H). Only the vascular endothelial cells were positive for CD31 (Figure 2I), factor FVIII and CD34 (data not shown). In addition, immunohistochemical analysis of Ki-67 levels showed similar cellular proliferation in the alveolar epithelium and the septal mesenchyme; 3% and 4%, respectively (data not shown).
Discussion
Review of published alveolar adenoma cases reported in the English-language literature.

Few case reports clarified whether these were mean or maximum diameters.
A, asymptomatic; COPD, chronic obstructive pulmonary disease; CT, computed tomography; F, female; LLL, left lower lobe; LML, left middle lobe; LUL, left upper lobe; M, male; MRI, magnetic resonance imaging; NA, not available; PET, positron emission tomography; RLL, right lower lobe; RML, right middle lobe; RUL, right upper lobe.
In radiographic studies, alveolar adenoma typically exhibits as a well-circumscribed, solitary, pulmonary nodule. 20 Only one case, with three nodules, was reported to have more than a single solitary pulmonary nodule. 3 The mean ± SD diameter of alveolar adenoma was calculated as being 2.4 ± 1.7 cm (range 0.2–9.1 cm; Table 1), with the mass size of the current case was the second largest to be reported. Most nodules were located in the left lower lobe (16/40), followed by the right upper lobe (nine patients), left upper lobe (five patients) and right lower lobe (five patients). All cases underwent surgical resection, and had a good prognosis without recurrence at follow-up.
In addition to the cystic lesion in the lung, the present patient also had cysts in the kidneys, liver and breast. Polycystic kidney disease (PKD) was inferred initially after MRI scan; however, given the patient’s negative family history of PKD and the fact that the number of renal cysts did not meet the basic criteria for PKD, 26 a diagnosis of PKD could not be established. To the authors’ knowledge, however, no previously reported case of alveolar adenoma has been associated with multifocal cysts.
Routine chest X-radiography serves as the most useful initial screening tool for alveolar adenoma, as most cases are asymptomatic and their pulmonary nodules are detected incidentally. CT commonly shows a well-defined, circumscribed nodule with homogeneous density for alveolar adenoma. MRI appears to be more sensitive in the detection of cystic lesions in the lung, compared with other imaging techniques. On MRI, in general, nodules of alveolar adenoma always demonstrate low-signal intensity on T1-weighted images, high-signal intensity on T2-weighted images and no marked enhancement on contrast. 3 It is, however, very difficult to establish the origin of the cyst by MRI, with the differential diagnoses of bronchogenic cysts, abscesses or postinflammatory granulomas also being made. 3 Bronchoscopy is unlikely to be useful in this condition: no diagnosis of alveolar adenoma has been established using this method, owing to the subpleural location of the lesions. 19
Alveolar adenoma is also difficult to diagnose on small biopsy specimens and frozen sections as the tissue can appear similar to normal lung parenchyma, or in some cases can simulate a malignancy, with small glandular spaces lined by regular glandular epithelium. 4 Although cytology can be useful to exclude malignancy, it is difficult to recognize the specific type of benign lesions. 16 Characteristics of alveolar adenoma include a network of spaces lined by simple low-cuboidal epithelial cells with the interstitial component varying from sparse to abundant; such adenomas also show collagen fibrils and spindle-shaped or oval cells. 19 It is recognized that spindle cells in the interstitium are mainly fibroblasts or fibroblast-like cells, 4 and that the lining cells are mainly type 2 alveolar epithelial cells. 3 Immunohistochemistry of epithelial cell markers in alveolar adenoma are helpful for confirming a diagnosis. These epithelial cells are mainly alveolar type 2 cells, which are characterized by positive immunohistochemical staining of TTF-1, prosurfactant protein B (pro-SP-B) and prosurfactant protein C (pro-SP-C). TTF-1 is a homeodomain-containing transcription factor that plays critical roles in lung-specific expression of surfactant proteins and is expressed selectively in thyroid, diencephalon and lung tissue. 4 Pro-SP-B and Pro-SP-C are the precursors for surfactant proteins B and C. Alveolar adenoma is always negative in CC10 staining, which represents the marker of Clara cells. 4 A correlation between alveolar adenoma and some genetic abnormalities has also been suggested; a clonal cytogenetic translocation of der(16)t(10;16)(q23:24) was observed in 19% of cells in the lesions of one case. 25
Differential diagnoses of alveolar adenoma.

Similarities apply to all benign and malignant diseases.
Alveolar adenoma is a rare benign neoplasm of uncertain histogenesis. Its rarity hampers characterization of its epithelial and mesenchymal elements. Most of the studies targeted at apoproteins B and C of human surfactant demonstrate that the epithelial element is derived from type 2 alveolar epithelial cells. 27 Some authors argue, however, that the cell of origin in alveolar adenoma is probably a primitive mesenchymal cell that has the capacity to differentiate towards a type 2 alveolar epithelial cell. 19 Given the predominant characteristic of alveolar epithelial cells in the present case, we agree with the inference that mesenchymal proliferation is most likely secondary to epithelial proliferation and is stimulated by epithelial-cell growth. 19 It is unclear whether both the epithelial and mesenchymal components are neoplastic. Some authors regard alveolar adenoma as being a benign proliferation of both the alveolar epithelium and the septal mesenchyme, wherease others believe that the proliferation is predominantly mesenchymal with alveolar entrapment, although it is possible that the epithelial component is also neoplastic.4,8 With respect to the present case, we favour the former idea, as both components demonstrated similarly low Ki-67 proliferation.
If all the preoperative diagnostic procedures implicate a benign lesion, clinical and radiological follow-up serves as a reasonable option at initial evaluation. Once progressive enlargement of the lesion is detected, however, surgical resection is indicated (to rule out malignancy and to confirm the diagnosis by postoperative pathology). All previous cases of alveolar adenoma had a good postoperative prognosis; none have reported recurrence or metastasis.
In conclusion, the present report describes an unusual case of alveolar adenoma, which is a rare cause of solitary pulmonary nodules. It is difficult to distinguish alveolar adenoma from other lesions through imaging and, although helpful in the exclusion of malignancies, bronchoscopy and frozen sectioning are of limited diagnostic value. Surgical excision is the principal treatment, and the final diagnosis depends on postoperative histopathology and immunohistochemistry findings. Alveolar adenoma is a benign neoplasm with a favourable prognosis. The histopathogenesis of alveolar adenoma remains to be clarified, however. The present case also had systemic multifocal cysts, and, although these were deemed to be incidental to the primary tumour, this requires further investigation.
Declaration of conflicting interest
The authors declare that there are no conflicts of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.