
Abstract
Erythema multiforme is a widespread hypersensitivity reaction, its pathogenesis is related to a variety of factors, including drugs and viral and bacterial infections. It is true that erythema multiforme is often caused by viruses while current studies suggest that it is mostly associated with herpes simplex virus infection, rarely associated with varicella-zoster virus infection. Here, we report a 50-year-old man admitted to our hospital because of rashes on the left rib with pain for 9 days and on limbs and hands for 2 days. Laboratory data showed that varicella-zoster virus (VZV-DNA) test was negative in blood by qualitative polymerase chain reaction. Herpes zoster virus IgM (VZV-IgM) enzyme linked immune sorbent assay was negative, and herpes zoster virus IgG (VZV-IgG) enzyme linked immune sorbent assay was positive. Herpes zoster and erythema multiforme was diagnosed. After treatment with antiviral, antiallergic, and topical drugs, the rashes was significantly improved. Our case report contributes to the pathogenesis of erythema multiforme.
Introduction
Erythema multiforme (EM) is an immune-mediated mucous skin disorder which is self-limited and often acute at the onset. The rash is symmetrically distributed on the limbs and trunk which is polymorphous and can be manifested as erythema, papules, wheals, and blisters. The characteristic skin lesions are the target-shaped lesions, which can also involve mucous membrane, and a few patients can even suffer visceral damage.1,2 EM mainly includes three types: classic EM, recurrent EM, and persistent erythema. 3
About 90% of EM cases are associated with infection, and herpes simplex virus (HSV) infection plays a major role in 70%–80% of cases.4,5 The most common cause of EM was HSV-1 and HSV-2 infection, with HSV-1 playing a major role in 66.7% of cases, HSV-2 in 27.8%, and both types in 5.6%. 6 Followed by Mycoplasma infection and other viruses such as adenovirus, Coxsackie virus, parvovirus B19, 7 and enterovirus,1,8 which were also reported. There have also been reports of erythema multiform rashes caused by COVID-19 infection. 5 Another type of causes is drugs, such as allopurinol, phenobarbital, phenytoin, valproic acid, antibacterial sulfa, penicillin, erythromycin, nitro nitrofurantoin, tetracycline, chlorine, ketone, acetyl salicylic acid, statin and different type of TNF-α inhibitors, such as Adalimumab, Infliximab, and Etanercept. 9 The article reports a case of male patient who developed EM pleomorphic erythematous rash appeared on his limbs and hands 1 week after the onset of a typical skin lesions of herpes zoster. We consider it is a case of EM caused by varicella-zoster virus (VZV). VZV-associated EM is a rare condition.
Case presentation
A 50-year-old male was admitted to the hospital with “rashes on the left rib with pain for 9 days and rashes on limbs and hands for 2 days.” Nine days ago, the patient developed erythema and blisters on the left rib with pain without any obvious reasons. He visited a health clinic and was diagnosed with “herpes zoster” and was suggested to take “Vitamin B1, mecobalamin tablets, acyclovir tablets,” and “Liushen pills” for external use. Six days ago, the patient was relieved of pain and stopped taking the drugs. Several new erythema were found on the extremities and palms 2 days ago. For further diagnosis and treatment, the patient was admitted to our department. The patient had received chickenpox vaccination when he was 2 years old. He has a history of sinusitis for 3 years, hypertension for 1 year, and takes 2.5 mg Leamlodipine maleate tablets once a day regularly since diagnosis.
Dermatological examination found that there were flaky clusters of red pimple herpes and blisters in the size of millet grains to rice grains on the left side of rib, some of the blisters dried up and crusted with dark red crusted skin and red base, without exceeding the midline of the body (Figure 1). Scattered erythema and papules of different sizes could be seen on the trunk and limbs. Some lesions were in the shape of targets (Figure 2).
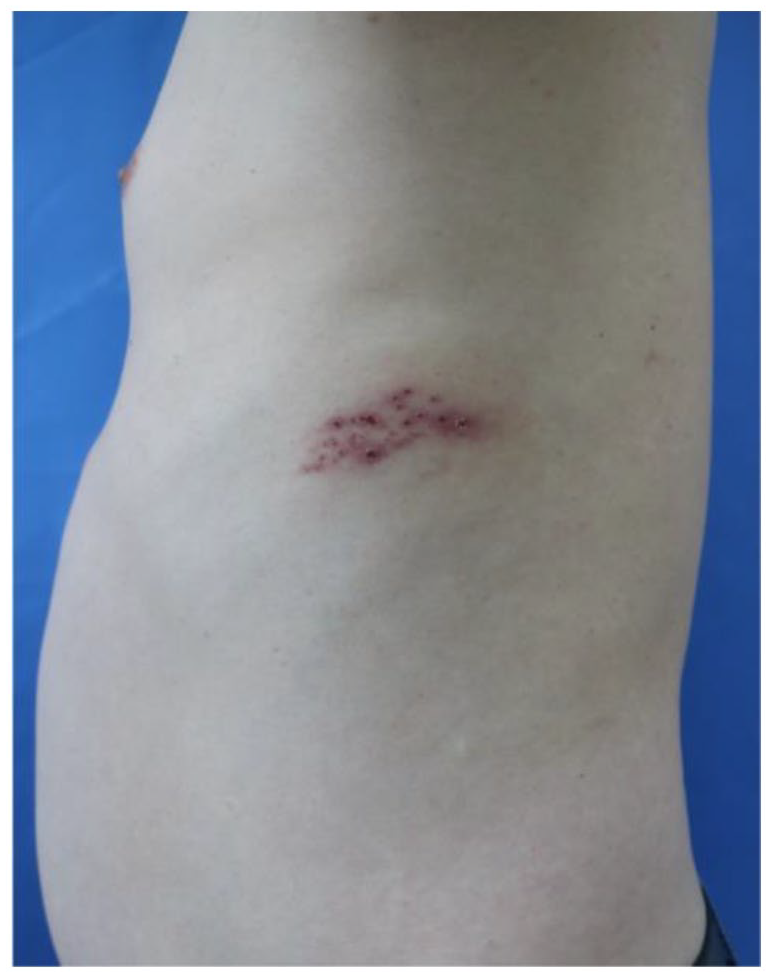
On the left side of the rib, there were clusters of herpes and vesicles, some of which dried up and formed scabs, with dark red scabs on the surface and red halo around the periphery.
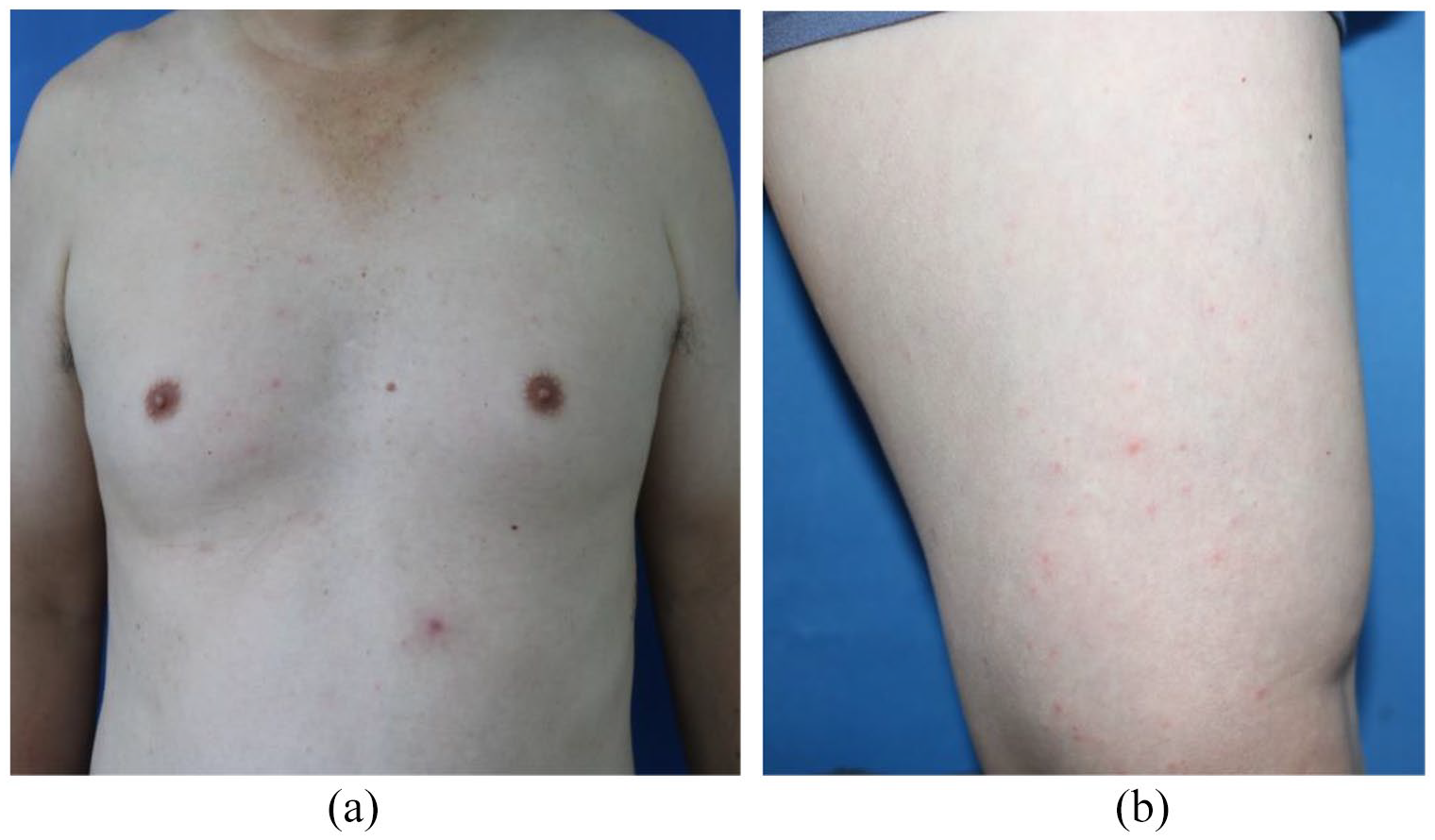
(a) Erythema and papules in trunk, and some lesions were in the shape of targets. (b) Erythema and papules in lower limbs.
Laboratory examination demonstrates Complement C1q 144↓mg/L (normal range 159–233), cytokines: interleukin 8 24.23 pg/ml↑ (0–20.60); blood lymphocyte subsets: NK cells 13.46% (6.40–12.50), NKT cells 6.76% (1.05–6.05), absolute values of T cells 778/uL↓ (955–2860), absolute values of CD4+ T cells 423/uL↓ (550–1440); respiratory pathogens: anti-influenza B virus IgM antibody positive; Rubella virus IgG 4.68 AU/mL↑(0.00–2.00). HSV-1 and HSV-2 IgG 16.36 AU/mL↑ (0.00–2.00); HSV-1 nucleic acid and HSV-2 nucleic acid were tested negative. VZV-DNA was negative in blood by qualitative polymerase chain reaction (PCR), while we did not perform the PCR of the skin lesions for VZV-DNA. Herpes zoster virus IgM (VZV-IgM) enzyme linked immune sorbent assay (ELISA) was negative, and herpes zoster virus IgG (VZV-IgG) ELISA was positive. Blood routine examination, erythrocyte sedimentation rate, urine and stool routine examination, infectious disease examination, procalcitonin, chest computed tomography (CT), and electrocardiograph showed no obvious abnormalities. A biopsy was performed on the lesions of the left lower limbs, and the pathological examination showed epidermal hyperkeratosis, spongy edema, focal liquefied degeneration of basal cells, infiltration of lymphocytes, and tissue cells around adjuncts of dermis and subcutaneous tissues, and no apoptotic keratinocytes were observed (Figure 3).
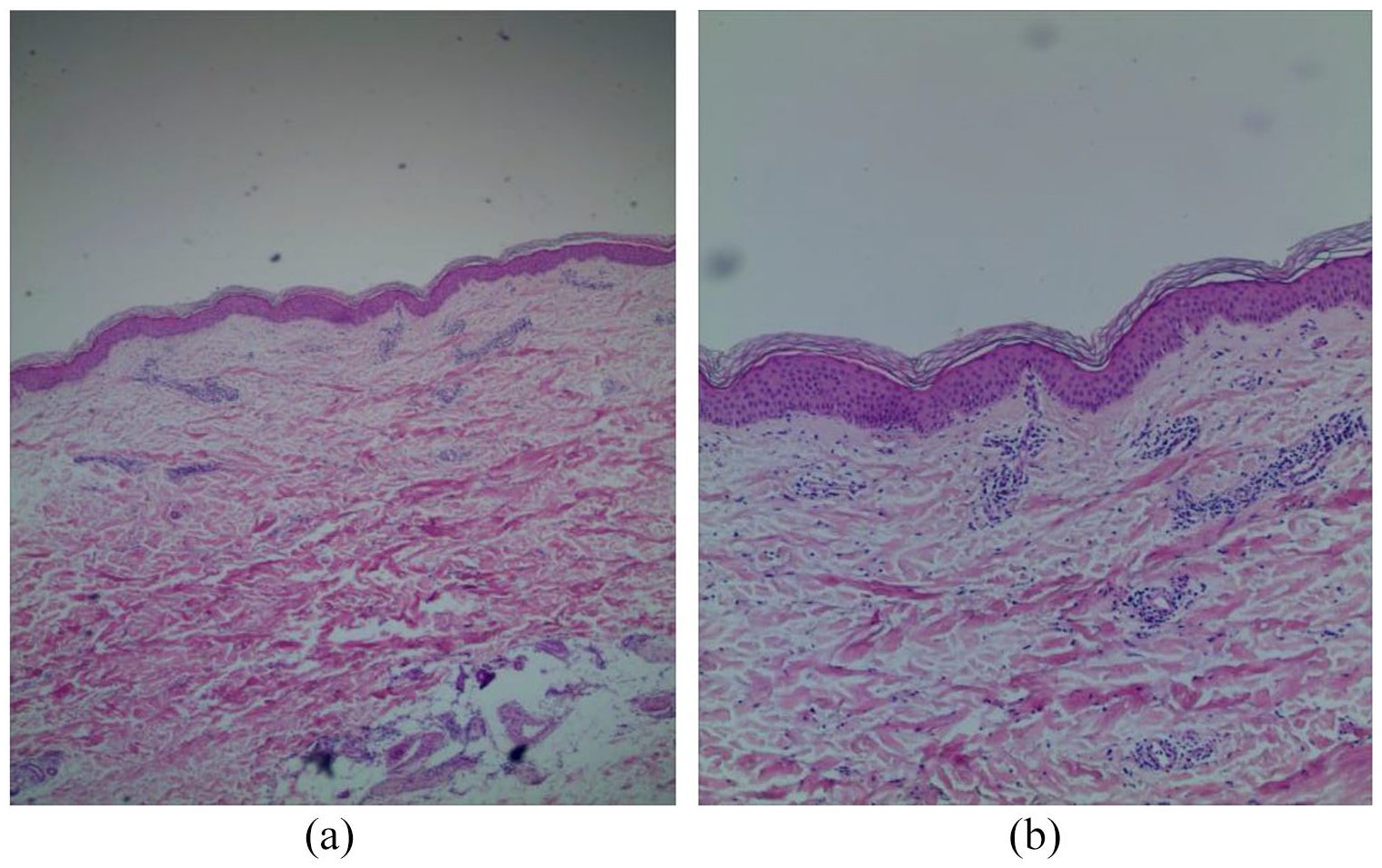
(a) Epidermal hyperkeratosis, spongy edema, focal liquefied degeneration of basal cells (H&E staining, 40×). (b) Infiltration of lymphocytes and histocytes behind adjuncts of dermis and subcutaneous tissues, and no apoptotic keratinocytes (H&E staining, 100×).
After he was admitted to the hospital, he was diagnosed with herpes zoster and EM. The patient was treated with Peniclovir, compound glycyrrhizin injection 60 mL/day, Mecobalamin tablets, Vitamin B1 tablets, Gabapentin capsules, Ebastin tablets, and Levocetirizine hydrochloride tablets, and topical mometasone furoate gel. After 10 days, the herpes dried and crusted, and the rashes on the trunk and limbs darkened. The patient was discharged after improvement. At a follow-up of 2 months after discharge, the patient reported complete resolution of the rash with no discomfort and no recurrence.
Discussion
At present, the diagnosis of EM is mainly based on the medical history and clinical manifestations; histopathological features and laboratory examination have no obvious specificity. Song et al. 10 found that the positive rate of herpes simplex IgG antibody was higher than that of IgM antibody among healthy people, which may be due to a certain interval between the asymptomatic HSV infection and detection of herpes virus antibody. The titer of IgM antibody would decrease significantly if the infection event of IgM antibody was longer than 2 weeks after the infection, while IgG could exist for a long time. In this case, although the IgG antibodies of HSV-1 and HSV-2 were elevated, the nucleic acids of HSV-1 and HSV-2 were tested negative, which could rule out EM caused by HSV infection. The patient showed typical herpes zoster at first, 1 week after a typical target-shaped rash of EM emerged. VZV IgG antibody was positive, and test results showed that the absolute values of T cells and CD4+ T cells were lower than the normal range, suggesting that there may be T lymphocyte damage resulting in decreased immunity of patients. The patient had immune dysfunction; viral infection and immune problems may be the etiology. After antiviral therapy, the patient’s symptoms improved. In addition to the pathological results, it can be speculated that the VZV caused EM. It is known that EM caused by HSV infection is the most common, and there are few reports about EM caused by VZV. At present, only a few cases of EM secondary to or combined with herpes zoster have been reported abroad.11–13
Treatment of acute EM is based on the self-limiting nature of the disease. The pathogeny should be confirmed before treatment, and if there is evidence of recent infection, the infection should be treated according to the cause first. Similarly, if there is evidence of drug involvement, the suspect drugs should be discontinued first. 14 Once the cause is under control, steroids or antihistamines can be administered, or glucocorticoids can be systematically administered to improve symptoms, and immunoglobulin can be used as an alternative in severe cases. For this patient, we gave antiviral, neurotrophic, and analgesic treatment for herpes zoster. The rash was significantly improved after treatment with compound glycyrrhizin, oral Ebastin tablets, Levocetirizine hydrochloride tablets, and topical mometasone furoate gel.
Conclusion
In summary, we reported a case of EM caused by VZV. It is rare, and such cases should be actively treated with antiviral, antiallergic drugs at the same time.
Footnotes
Acknowledgements
The study has obtained the written patient consent, and we thank the patient’s cooperation during the treatment. The authors also thank the editors and reviewers for the valuable comments and suggestions.
Author contributions
DW, DP, and XX performed the pathological studies and clinical data collection. QZ was in charge of patient care and drafted this manuscript. GZ revised the manuscript critically for important intellectual content. All authors contributed to the article and approved the submitted version.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval to report this case was obtained from *Ethics Committee of The First Hospital of Hebei Medical University (No. 20220217).
Informed consent
Written informed consent was obtained from the patient for his anonymized information to be published in this article.