
Abstract
Primary hepatic lymphoma is a rare disease, and primary hepatic mucosa-associated lymphoid tissue (MALT) lymphoma accounts for only 0.3% of all primary hepatic lymphomas. Herein, we report a case of primary hepatic MALT lymphoma in a male patient in his mid-40 s with chronic hepatitis B infection. The patient visited our department for further examination of a hepatic nodule initially visualized through abdominal pelvic computed tomography (CT). Based on imaging studies and elevated levels of tumor markers, the tumor was suspected to be hepatocellular carcinoma. A laparoscopic inferior sectionectomy (segment 5 and 6) was performed, and immunohistochemical staining revealed that the tumor was positive for CD20, B-cell lymphoma 2, pan-cytokeratin (CK), and CK19 markers. Pathological findings revealed it to be a primary hepatic MALT lymphoma. After surgery, bone marrow biopsies and fluorodeoxyglucose-positron emission tomography integrated with CT scanning confirmed that there was no other involvement. The patient did not receive chemotherapy, and there was no recurrence during the 24-month follow-up period. Hepatocellular carcinoma is the most common malignancy in patients with chronic hepatitis B, but rare tumors such as primary MALT lymphoma can also occur, so a careful approach is required for their differentiation.
Keywords
Introduction
Primary hepatic lymphoma without extrahepatic infiltration occurs rarely, accounting for 1.1% of all primary hepatic tumors and 0.4% of extranodal non-Hodgkin lymphomas (NHL).1,2 The most common histological type of primary hepatic lymphoma is diffuse large B cell lymphoma, and primary hepatic mucosa-associated lymphoid tissue (MALT) lymphoma accounts for only 3% of primary hepatic lymphomas. 3
Certain viral infections have been associated with the development of primary hepatic lymphomas, including hepatitis B virus (HBV) and hepatitis C virus (HCV).4,5 However, the relationship between viral infection and hepatic MALT lymphoma is unclear.
Primary hepatic MALT lymphoma is frequently misdiagnosed because it rarely presents with hepatic tumors and has non-specific clinical manifestations. Primary hepatic MALT lymphomas are often assumed to be other hepatic tumors, such as hepatocellular carcinoma (HCC), hepatic hemangioma, hepatic adenoma, and focal hyperplasia of the liver. In this case report, we describe a patient with chronic HBV infection and a hepatic tumor that was initially suspected to be HCC, but which was then diagnosed as primary hepatic MALT lymphoma based on pathologic confirmation.
Case report
A male patient in his mid-40 s with chronic hepatitis B visited our department for further examination of a hepatic nodule seen on an abdominal pelvic computed tomography (CT) scan (Figure 1). He had no symptoms, including nausea, vomiting, abdominal pain, or fever, and no history of weight loss or night sweats. A physical examination revealed no obvious abnormalities, and an endoscopic biopsy of the stomach revealed no Helicobacter pylori infection.
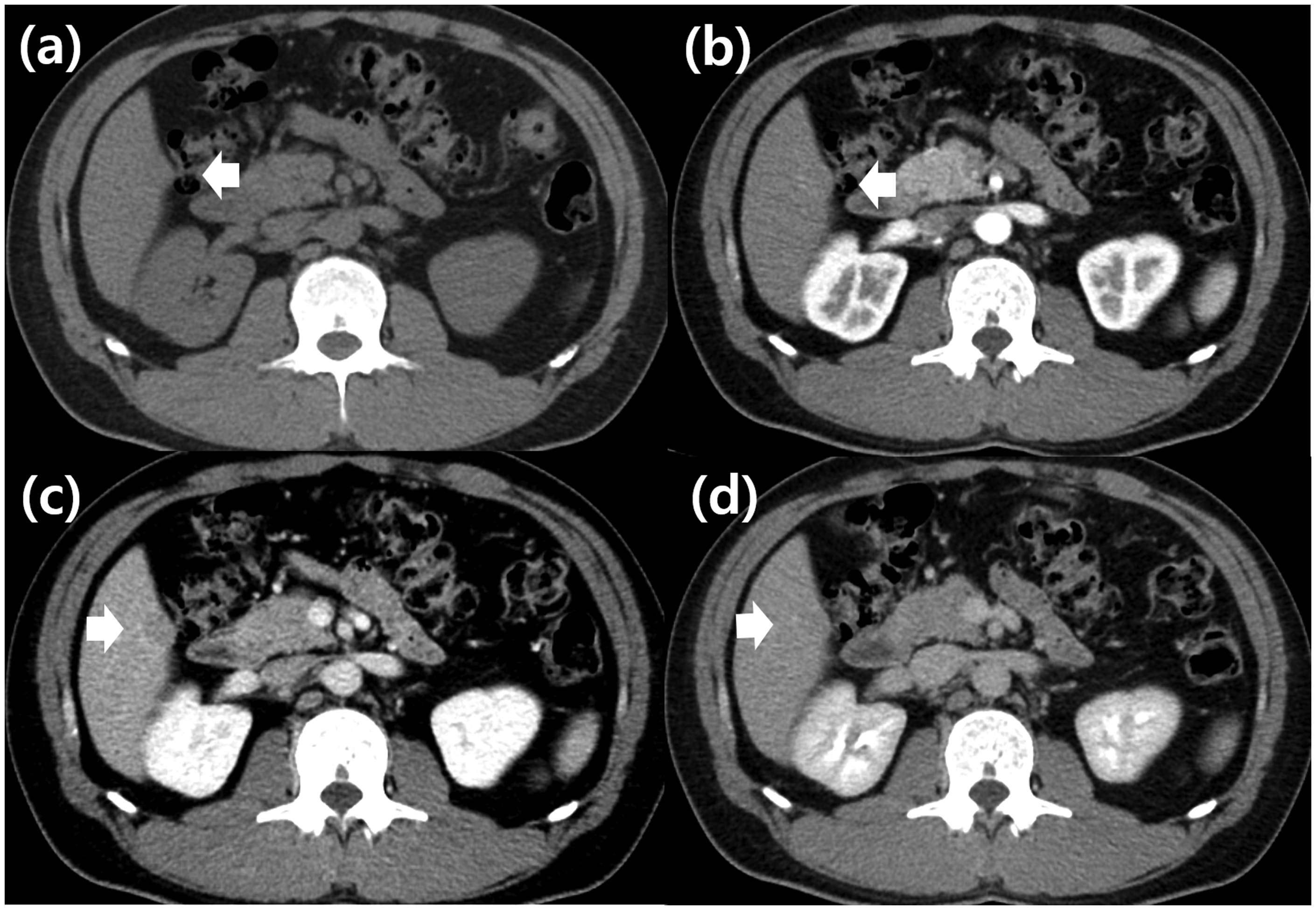
Initial CT images of the patient confirming primary hepatic MALT lymphoma. (a) Axial precontrast CT showing a 1.8-cm isodense bulging mass in segment 5. (b) Contrast-enhanced CT showing no enhancement in the arterial phase. (c) Low-density attenuation in the portal vein phase (arrow) and (d) Contrast-enhanced CT showing low attenuation in the delayed phase.
Laboratory findings showed a hemoglobin level of 16.5 g/dL, leukocyte count of 4,410/mm3, platelet count of 176,000/mm3, aspartate aminotransferase/alanine aminotransferase levels of 146/263 IU/mL, total bilirubin level of 1.17 mg/dL, prothrombin time (international normalized ratio) of 1.00, and albumin level of 42.0 g/dL. Tumor markers were alpha-fetoprotein (AFP) 40.9 ng/mL, protein induced by vitamin K absence-II 14 mAU/mL, and carcinoembryonic antigen (CEA) 2.3 ng/mL. Viral markers were hepatitis B surface (Hbs) antigen (Ag)-positive, anti-Hbs antibody (Ab)-negative, anti-HCV-negative, hepatitis E (Hbe)Ag-positive, anti-HbeAb-negative, and HBV DNA levels of 1,820,000 IU/mL.
He was started on tenofovir 300 mg daily to treat the HBV infection. The hepatic tumor was 1.8 cm in diameter; it appeared isodense in the pre-contrast phase, not enhanced in the arterial phase, and had low attenuation in the portal vein phase and delayed phase on the CT scan (Figure 1a–d). Liver magnetic resonance imaging (MRI) was performed to evaluate hepatic nodules (Figure 2a–d). T1-weighted MRI showed a 2.5-cm arterial enhancing and portal washout lesion in segment 5 of the liver. The nodule showed diffusion restriction and mild hypersignals on T2-weighted imaging. These findings suggested a 2.5-cm HCC. Borderline lymph nodes were found in the portacaval space and along the common hepatic artery, and seemed to be reactive lymphadenopathy. The spleen was normal.
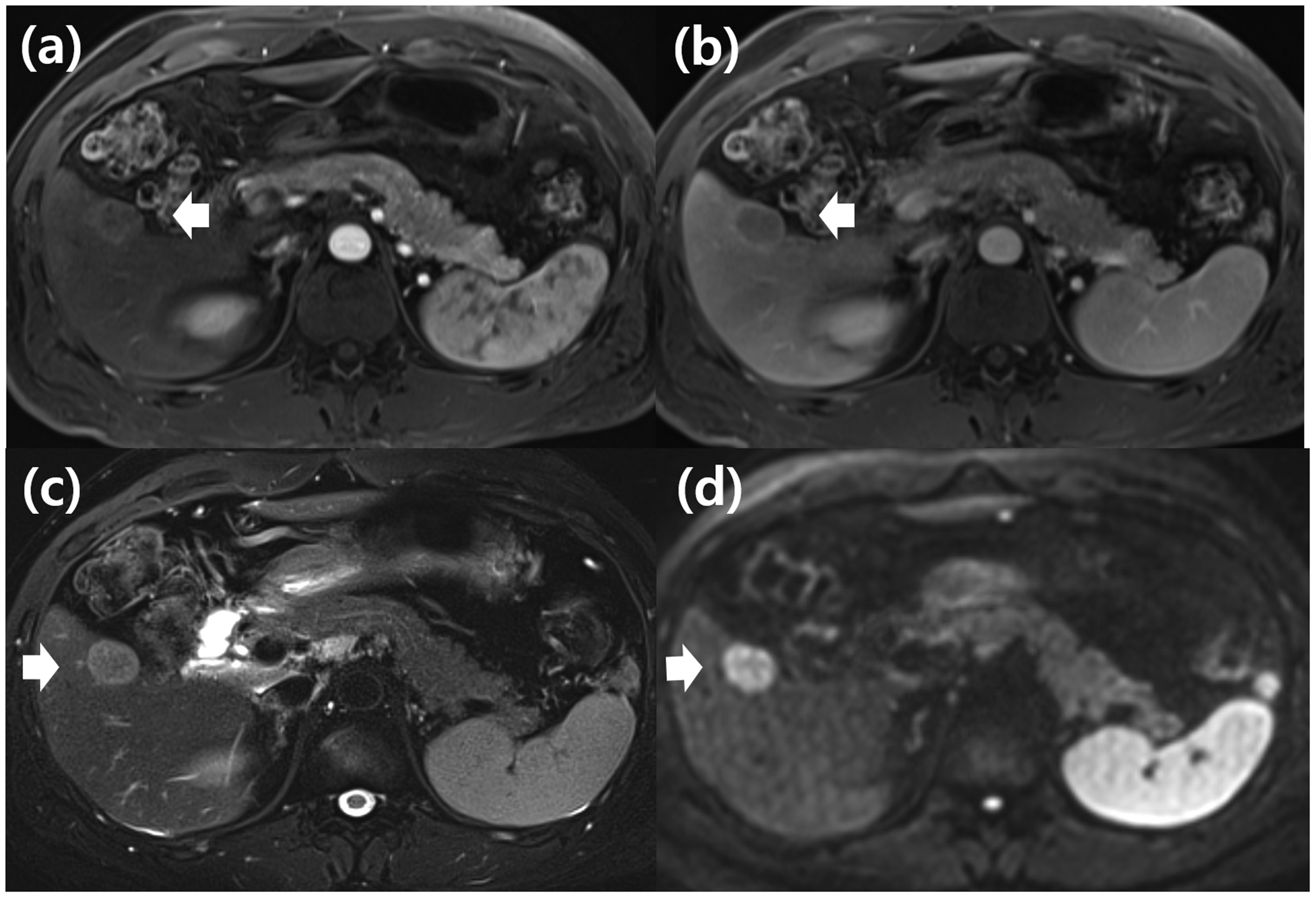
Initial MRI images of the patient. (a) Axial T1-weighted MRI showing a 2.5-cm arterial enhancing lesion in segment 5. The lesion appears slightly larger than when observed during the CT scan. (b) T1-weighted MRI showing a washout lesion in the portal vein phase. (c) T2-weighted MRI with fat suppression showing a high signal intensity and (d) Diffusion restriction is noted in the b900 DWI image.
HCC was considered a preferential diagnosis because the patient had an HBV infection, elevated levels of tumor marker AFP, and suspicious MRI findings. He was admitted for surgical resection of the hepatic nodule, which was suspected to be HCC. Laparoscopic inferior sectionectomy (segments 5 and 6) was performed using the Glissonian approach, and a 2.5-cm × 2.0-cm expanding nodular tumor was documented in the pathology report (Figure 3a).

Pathology and immunohistochemical stains of primary hepatic MALT lymphoma. (a) Cut section of the resected liver showing a well-defined tan mass composed of densely proliferated lymphoid cells (hematoxylin and eosin staining, 10 × magnification). (b) Under high power view, small lymphoid (tumor) cells are shown mixed with plasma cells (100× magnification). (c) Tumor cells are positive for CD20 immunohistochemical staining (100 × magnification) and (d) Cytokeratin (AE1/AE3) immunohistochemical staining showing prominent lymphoepithelial lesions (100 × magnification).
Immunohistochemical staining results were: CD20-positive, B-cell lymphoma 2-positive, CD3-negative, CD10-negative, cyclin D1-negative, CD30-negative, and pan cytokeratin (CK)- and CK19-positive in lymphoepithelial lesions, with no kappa and lambda light chain restriction, a Ki-67 index of 15% to 20%, and negative Epstein-Barr virus-encoded RNA in situ hybridization (Figure 3b–d). The final pathologic diagnosis was a single lesion of external marginal zone lymphoma of MALT in the liver.
Two weeks later, bone marrow biopsies and fluorodeoxyglucose-positron emission tomography examination integrated with computed tomography scanning (FDG-PET CT) were performed, and no other involvement of MALT lymphoma was observed. Immunofixation was suspected to be lambda-type monoclonal gammopathy. The patient had stage I external marginal zone lymphoma of the MALT and did not undergo chemotherapy. No recurrence or complication was observed during the 24-month follow-up period.
Consent for treatment was obtained from the patient, and all identifying patient details have been removed from this case report, which is written according to CARE guidelines. 6 This study was conducted in accordance with the guidelines of the Declaration of Helsinki and approved by the Research Ethics Committee of Ilsan Hospital (protocol code: NHIMC 2022-08-027; date of approval: 1 September 2022). Informed consent was waivered on approval by the National Health Insurance Corporation Ilsan Hospital Institutional Review Board.
Discussion
We describe a case of primary hepatic MALT lymphoma, initially suggestive of HCC, in a patient with chronic hepatitis B. Primary hepatic lymphoma is defined as a lymphoma confined to the liver without the involvement of lymph nodes, bone marrow, or other organs. 4 It is a rare type of primary hepatic tumor, with primary hepatic MALT lymphoma accounting for only 3% of primary hepatic lymphomas.1–3
MALT lymphoma usually occurs in cases of chronic inflammation associated with infections such as H. pylori or autoimmune diseases.5,7,8 However, the etiology of primary hepatic MALT lymphoma remains unknown and further research is needed to determine whether chronic inflammation contributes to its development. Most hepatic MALT lymphomas arise in cases of liver disease such as primary biliary cirrhosis, HCV, HBV, or hepatitis associated with other causes. 9 In the present case, our patient had a medical history of HBV infection, but there was no evidence of H. pylori infection.
Several epidemiologic studies have demonstrated that HBV and HCV might be causative of NHL,10,11 and these infections have also been reported to be associated with the development of primary hepatic lymphoma.12,13 HBV is thought to stimulate B cells, leading to monoclonal B cell expression. 14 Moreover, an association between HBV DNA expression and NHL has been reported, with patients with indolent NHL having significantly higher HBV DNA levels at the time of initial NHL diagnosis than patients with aggressive NHL. 15
A diagnosis of lymphoma is mainly based on histopathological and immunohistochemical findings combined with clinical and imaging data; however, primary hepatic lymphoma can be misdiagnosed as HCC, hepatic adenoma, or other hepatic tumors. In the present case, the hepatic lesion was initially suspected to be HCC because the patient had chronic liver disease and elevated AFP levels; however, a final diagnosis of primary hepatic MALT lymphoma was confirmed by surgical pathology. The diagnostic accuracy of traditional percutaneous liver biopsies is not high, so a diagnosis of primary hepatic lymphoma is often achieved via a surgical biopsy. 16 Additionally, according to practice guidelines for HCC, high-risk patients such as those with chronic HBV or HCV infections, or, liver cirrosis, HCC can be diagnosed without biopsy based on typical findings of HCC >1 cm on multiphase MRI. 17 Because this case was suspected to be HCC, percutaneous liver biopsy was not considered before surgical resection.
Most patients with primary hepatic lymphoma show symptoms such as nausea, vomiting, and abdominal discomfort, and one-third show constitutional symptoms including fever, myalgia, and weight loss.18,19 However, most patients (85.4%) with primary hepatic MALT lymphoma in a previous study were asymptomatic, 79.6% had solitary hepatic lesions, and 88.9% were stage IE. 9 Nevertheless, many primary hepatic MALT lymphomas are diagnosed at an early stage. 9 In the present case, no clinical symptoms were observed, and elevated transaminase levels were thought to reflect active HBV infection. Therefore, clinical and laboratory data did not help differentiate hepatic nodules from primary hepatic MALT lymphoma in this instance. Although primary hepatic MALT lymphoma was diagnosed in a clinically unsuspected state, the diagnosis was still made at an early stage (Ann Arbor stage I).
In primary hepatic MALT lymphoma, levels of tumor markers such as AFP, CEA, and CA19-9 are usually normal. In our patient, AFP levels were elevated to 40.9 ng/mL, representative of inflammation associated with active chronic hepatitis B; this is similar to a previously reported patient who demonstrated high AFP levels representative of chronic inflammation associated with chronic hepatitis C. 20 Therefore, elevated AFP levels contributed to the initial exclusion of a diagnosis other than HCC in this case.
Primary hepatic MALT lymphoma previously appeared as a low-density lesion on the CT scan with no or slightly enhanced contrast,21,22 while MRI revealed a similar enhancement pattern, and a low signal intensity on the T1-weighted image and moderately high signal intensity on the T2-weighted image.23,24 The CT scan of our patient similarly showed low attenuation in the portal vein phase and mild hypersignal density in T2-weighted MRI images. However, these imaging findings are similar to those of other solid tumors in the liver, so it was difficult to differentiate these from HCC. The value of FDG-PET CT in diagnosing MALT lymphoma is not yet clear. A 71% detection rate for MALT lymphoma has been reported using FDG-PET CT, but rates vary depending on the primary site. 25 The accuracy of FDG-PET CT is unknown for primary hepatic MALT lymphoma, but definite FDG uptake has been reported in a case series. 24 However, a literature review showed that only 15.2% of patients with primary hepatic MALT lymphoma underwent FDG-PET CT, so its diagnostic value remains controversial. 26
There are no standard guidelines for the treatment of primary hepatic MALT lymphoma because of the small number of patients worldwide. In this case, only surgical resection was performed. It has been reported that 88.9% of patients with primary hepatic MALT lymphoma were diagnosed at Ann Arbor stage I, and the surveillance for HCC was helpful for early stage diagnosis of hepatic MALT lymphoma in chronic hepatitis B. 9 In primary hepatic MALT lymphoma, the recurrence rate was reported to be 11% (from 12 to 96 months). 27 In this case, there was no recurrence during the 2-year follow-up. Chemotherapy such as rituximab, which was shown to achieve long-term remission, 28 may be considered in the event of recurrence.
The clinical features and optimal treatment for primary hepatic MALT lymphoma are unclear. We therefore suggest that hepatologists should consider the rare possibility of primary hepatic MALT lymphoma when approaching a diagnosis of hepatic tumor, especially in cases of chronic hepatitis B. The establishment of diagnostic strategies for rare hepatic tumors such as primary hepatic MALT lymphoma will avoid unnecessary hepatic resections, so additional research is needed to develop these.
Research Data
Research Data for Primary hepatic mucosa-associated lymphoid tissue lymphoma mimicking hepatocellular carcinoma in a patient with chronic hepatitis B: a case report
Research Data for Primary hepatic mucosa-associated lymphoid tissue lymphoma mimicking hepatocellular carcinoma in a patient with chronic hepatitis B: a case report by Hee Dong Koh, Jong Won Choi, Eun Kyung Kim, Sumi Park, Min Ji Kim and Chun Kyon Lee in Journal of International Medical Research
Footnotes
Availability of data and materials
All information about the patients came from the Department of Gastroenterology, Ilsan Hospital.
Authors’ contributions
Hee Dong Koh wrote the manuscript and obtained patient information. Jong Won Choi contributed to the project concept and design. Hee Dong Koh and Jong Won Choi reviewed the literature and drafted the manuscript. Eun Kyung Kim and Sumi Park were responsible for the acquisition and analysis of imaging data. Min Ji Kim and Chun Kyun Lee revised the manuscript accordingly. All authors approved the final manuscript and agreed to publish it as a case report.
Declaration of conflicting interests
The authors declare that they have no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.