
Abstract
Primary hepatic mucosa-associated lymphoid tissue (MALT) lymphoma is an extremely rare liver malignancy that usually lacks characteristic imaging findings and which is often misdiagnosed. We report a 63-year-old woman diagnosed with primary hepatic extranodal marginal zone B-cell lymphoma, MALT type. The patient underwent needle biopsy and radiofrequency ablation (RFA), and showed no signs of relapse during the 12-month postoperative follow-up. This case stresses the rarity of primary hepatic MALT-type lymphoma and the unique and effective treatment for this patient. Our patient received RFA, which showed good efficacy and which provides a new option for the treatment of hepatic MALT lymphoma. We also present our findings from a systematic review to improve the current understanding of this disease.
Keywords
Background
Primary hepatic lymphoma (PHL) is a rare disease that accounts for only 0.1% of liver malignancies, 0.4% of extranodal lymphomas, and 0.016% of non-Hodgkin's lymphomas (NHL).1,2 Primary hepatic marginal zone B-cell mucosa-associated lymphoid tissue (MALT) lymphoma accounts for only 3% of all cases of PHL. 3 The concept of MALT lymphoma was first proposed by Isaacson and Wright in 1983 to describe extranodal malignant lymphoma of marginal zone B-cell origin. 4 MALT lymphoma can involve the gastrointestinal tract, salivary gland, conjunctiva, thyroid, lung, breast, and liver. 5 Primary hepatic MALT lymphomas are extremely rare, and there are only a few reports of the clinical characteristics and the best treatment methods. Increasing early recognition of hepatic MALT lymphomas can avoid unnecessary liver resection or reduce the scope of liver resection if the cancer is responsive to preoperative chemotherapy. 6 Herein, we report a case of primary hepatic MALT lymphoma with a review of the relevant literature to provide detailed understanding of primary hepatic MALT lymphoma.
Case presentation
A 63-year-old woman was admitted to the hospital following an incidental discovery of a focal liver mass on ultrasonography. The patient reported no symptoms other than upper abdominal discomfort, and she had no significant medical history. Her physical examination findings were unremarkable, without splenomegaly or superficial lymph node enlargement. All clinical laboratory parameters, namely blood routine examination, hepatic and renal function, alpha-fetoprotein (AFP), carcinoembryonic antigen (CEA), and carbohydrate antigen 19-9 (CA19-9), were within the reference ranges. No hepatitis B virus (HBV), hepatitis C virus (HCV), or human immunodeficiency virus (HIV) infection was found, and no abnormal rheumatic and immunity indices were identified. In addition, no Helicobacter pylori (HP) infection or tumor was observed by upper gastrointestinal endoscopy.
Abdominal ultrasonography showed a hypoechoic liver mass in segment VI (S6). Enhanced magnetic resonance imaging (MRI) showed a 1.6- × 1.7-cm solitary mass with T1 hypointensity and T2 hyperintensity (Figure 1a). The mass was enhanced in the arterial phase and washed out in the portal phase (Figure 1b, c), and the lesion showed low signal intensity in the hepatocyte-specific phase (Figure 1d). No extrahepatic mass was discovered by MRI. Contrast-enhanced ultrasonography (CEUS) showed that the nodular lesion had mild heterogeneous hyperenhancement in the arterial phase, which was washed out in the portal phase (Figure 1e, f). According to the results of the imaging examinations, the tumor was suspected to be hepatocellular carcinoma (HCC). According to the guidelines for the diagnosis and treatment of primary liver cancer in China (2019 edition), when a tumor measures less than 2 cm, the tumor-free survival rate and overall survival rate after radiofrequency ablation (RFA) are similar to rates following surgical resection, but the incidence of complications and the length of hospital stay are lower than with surgical resection. The patient consented to undergo needle biopsy and RFA.

Enhanced magnetic resonance imaging findings.
Histological analysis revealed diffuse and uniform infiltration of typical centrocyte-like lymphoid cells, and lymphoepithelial lesions could be observed in some bile ducts infiltrated with these small-to medium-sized lymphocytes. Immunohistochemical staining was positive for CD20, B-cell lymphoma-2 (BCL-2), and CD21 (irregular expansion of the follicular dendritic cell (FDC) network). Histological evidence of bile duct injury and ductal proliferation was highlighted by cytokeratin AE1/AE3 immunostaining. Moreover, CD3, CD5, CD10, CD23, CD43, BCL-6, and cyclin D1 activity were negative, and the Ki-67 index was approximately 5% (Figure 2). According to the pathological findings, the patient was diagnosed with primary hepatic extranodal marginal zone B-cell MALT type lymphoma.
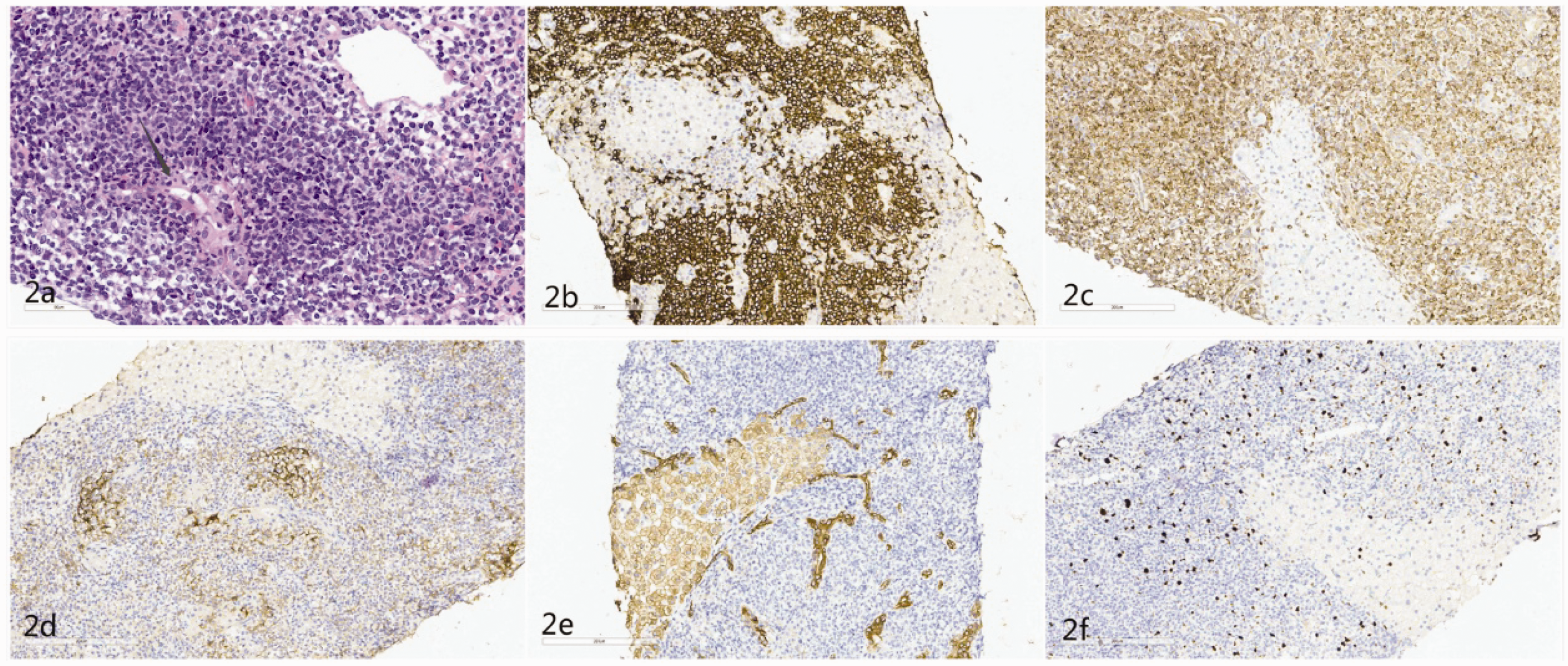
Histological examination findings.
The patient’s disease was classified as Ann Arbor stage IE. No additional treatment was performed, and close follow-up was recommended. Postoperative computed tomography (CT) of the abdomen showed effective results of the ablation (Figure 3a). The patient underwent fluorine-18-fluorodeoxyglucose positron emission tomography/CT (18F-FDG PET/CT) after discharge, and no signs of hypermetabolic tumors were found. No abnormal indicators were found in blood routine examination and liver biochemistry examination of the patient at the follow-up evaluations, which were performed every 3 months. No abnormal MRI findings were observed 1 year after operation (Figure 3b, c, d), and the patient remains well, and has shown no signs of relapse for 12 months postoperation.

Postoperative abdominal computed tomography showing effective results of ablation position (a). Enhanced MRI findings 12 months after radiofrequency ablation (RFA) were as follows: no abnormal signal on T2-weighted imaging (b), and no wash-in in either the arterial phase (c) or portal phase (d).
Discussion
MALT lymphomas are low-grade B-cell lymphomas, among which HP-related gastric MALT lymphoma is the most common. Currently, there are generally recognized unified standards for the diagnosis and treatment of gastric MALT lymphoma. However, primary hepatic MALT lymphoma is extremely rare, and its etiology, clinical characteristics, and the best treatment methods remain unclear. Therefore, we summarized our case, with a review of the relevant literature to improve the understanding of the disease and to provide clinical evidence for future diagnosis and treatment.
To the best of our knowledge, 113 cases of primary hepatic MALT lymphoma have been reported in 71 articles to date,7–37 of which 80 cases (including our case) had relatively detailed clinical data (Table 1). Among the patients in these 113 cases, 43 patients were men (38%) and 48 were women (42%) (the sex was not indicated in the remaining cases), with an age range of 30 to 89 years and a median age of 63.5 years. Most patients (58.8%) were asymptomatic, and most (72.8%) had a single tumor, with a diameter of 0.7 cm to 20 cm.
Summary of the clinical features of cases of primary hepatic MALT lymphoma (including the present case).

The median (range) for age, tumor diameter, and follow-up time is shown. NA: not available; HBV: hepatitis B virus; HCV: hepatitis C virus; PBC: primary biliary cirrhosis; AIH: autoimmune hepatitis; MRI: magnetic resonance imaging; CEUS: contrast-enhanced ultrasonography; 18F-FDG PET/CT: fluorine-18-fluorodeoxyglucose positron emission tomography/computed tomography; SUV: standardized uptake value.
MALT lymphoma usually develops in chronic inflammation accompanied by infectious pathogens, such as HP-related chronic gastritis and autoimmune diseases. Nevertheless, the cause of primary hepatic MALT lymphoma is not fully understood. Some scholars believe that continuous inflammatory stimulation may induce development of the disease. 5 In previous case reports, primary hepatic MALT lymphoma was considered to be related to primary biliary cirrhosis (PBC), 38 HCV,39–42 HBV,43,44 HP infection, 45 non-alcoholic steatohepatitis (NASH), 31 and Epstein–Barr virus. 46 However, a meta-analysis involving approximately 16,300 patients with PBC found no significant correlation between PBC and NHL. 47 In the literature review, we identified 22 cases of HBV (19.3%), 16 cases of HCV (14.0%), 8 cases of PBC (7.0%), 2 cases of autoimmune hepatitis (AIH) (1.8%), and 12 cases of HP infection (10.5%). In our case, the patient had no history of HBV, HCV, autoimmune disease, or HP infection. Owing to the rarity of the disease, the exact role of related risk factors in the occurrence of primary hepatic MALT lymphoma requires further investigation.
Imaging findings in PHL have been reported extensively. However, more than 90% of the PHL cases were diffuse large B-cell lymphomas (DLBCL), and there is no characteristic description of hepatic MALT lymphoma imaging findings. Dong et al. 11 recommended that the possibility of hepatic MALT lymphoma should not be excluded when liver tumors have no obvious space-occupying effect on CT imaging, and the blood vessels and bile ducts in the liver are running normally. In the literature review, there were 36 comprehensive MRI descriptions. Almost all cases showed T1 low signal intensity and T2 high signal intensity, but there was no regular pattern in the arterial and portal phases. CEUS guidelines suggest that CEUS can help in the differential diagnosis of rare liver tumors. 48 However, the guidelines do not discuss the imaging findings of primary hepatic MALT lymphoma because of the limited number of cases. According to our review of the relevant literature, five cases of primary hepatic MALT lymphoma were diagnosed and analyzed by CEUS (four cases were described in detail), of which two cases showed uneven enhancement in the arterial phase and uneven regression in the portal phase. 13 Our case showed the same characteristics. The other two cases showed uniform wash-in and wash-out in the arterial and portal phases, respectively, suggesting susceptibility to HCC.14,49 It is atypical to see uneven enhancement in the arterial phase of HCC. Therefore, when the tumor shows uneven wash-in and wash-out during enhanced imaging, hepatic MALT lymphoma should be included in the differential diagnosis. Shiozawa et al. 49 suggested that the feature of no blood vessels penetrating the tumor may distinguish primary hepatic MALT lymphoma from other malignant lymphomas. Compared with dynamic CT and MRI, CEUS can evaluate intratumoral hemodynamics in real time, which is easier and more accurate for visualizing penetrating blood vessels. 49
The role of 18F-FDG PET/CT in the detection rate, diagnosis, and follow-up of MALT lymphoma remains controversial. Certain types of MALT lymphoma, such as pulmonary, 50 breast, 51 and head and neck, 52 are 18F-FDG avid in most cases, while others, such as gastric MALT lymphoma are less avid because of the physiological or inflammatory activity resulting in 18F-FDG uptake that can mask oncological lesions. 53 However, the diagnosis of primary hepatic MALT lymphoma by 18F-FDG PET/CT has not been clearly described. In previous reports, PET-CT was performed in 18 cases, and all hepatic MALT lymphomas showed high metabolism with 18F-FDG.7,9,11,19,23,26,32,35,40,54–57 Although the standardized uptake value (SUV) is the most widely used parameter in MALT lymphoma, this measurement is easily affected by many factors. Albano et al. 52 recommended that other metabolic parameters (such as metabolic tumor volume (MTV) and total lesion glycolysis (TLG)), which include both morphological and metabolic characteristics, may be useful in predicting treatment response and prognosis. The relevant parameters can be further refined to effectively assess the prognosis of hepatic MALT lymphoma. A recent study proposed that the 18-FDG metabolic rate of extragastric MALT lymphoma is significantly related to Ki-67 proliferation. 58 When Ki-67 was >15%, the 18-FDG uptake in the lesions was significantly increased; however, only four cases of related hepatic MALT lymphoma were evaluated in the study. Hence, this result needs further study, but is valuable for postoperative prognostic evaluation and follow-up. Importantly, compared with other aggressive lymphomas such as DLBCL, MALT lymphoma has a relatively low FDG uptake intensity.59,60 In our patient, 18F-FDG PET/CT was not performed before surgery; however, postoperative 18F-FDG PET/CT showed no hypermetabolic lesions. This not only indicated no extrahepatic lesions but also proved that the RFA was very successful. Whether 18F-FDG PET/CT can also be used for early diagnosis, staging, and treatment of hepatic MALT lymphoma remains unclear, and large samples are necessary for analysis. However, 18F-FDG PET/CT is helpful in the diagnosis of primary hepatic MALT lymphoma when there are no high-uptake lesions in other parts of the body. 18F-FDG PET/CT may become a new method for staging, follow-up, and prognostic evaluation in the future.
Most MALT lymphoma masses are discovered incidentally and lack extrahepatic manifestations, and are often misdiagnosed. Among the retrieved cases from the literature, almost all cases could not be clearly diagnosed before pathological diagnosis. Some cases were diagnosed as other malignant tumors or even benign tumors before surgery or biopsy. We initially diagnosed our case as HCC before surgery; therefore, the diagnosis of primary hepatic MALT lymphoma requires pathological biopsy for confirmation. Pathological biopsy of primary hepatic MALT lymphoma shows that the marginal zone cells infiltrate the epithelium, which can cause the formation of lymphoepithelial lesions. Lymphoepithelial lesions of the bile duct are typical manifestations of primary hepatic MALT lymphoma, 61 which is consistent with our case. Marginal zone B-cell lymphomas are usually positive for CD20 and CD79a, but not for CD5, CD10, CD23, and CD43, and usually express immunoglobulin M (IgM) and Bcl-2. Ki67, p53, and Bcl-6 expression may help distinguish liver marginal zone B-cell lymphoma from DLBCL. Typical liver marginal zone B-cell lymphomas grow slowly, and if these markers are diffusely expressed, the mass is closer to DLBCL. 61 Therefore, extensive immunohistochemical and molecular studies are essential to distinguish lymphoma from other malignant tumors as well as to judge the immunophenotype of the lymphoma.
The treatment recommendations of the United States National Comprehensive Cancer Network for non-gastric MALT lymphomas are radiotherapy, surgery, chemotherapy, and comprehensive treatment. However, it is not possible to design prospective randomized clinical trials to determine the optimal treatment of this cancer because of its rarity. According to the reported literature, 48.2% of the patients underwent surgical resection or liver transplantation after diagnosis, accompanied by adjuvant chemotherapy, and achieved satisfactory postoperative effect. Most patients were cured; however, there were two cases of tumor recurrence during long-term follow-up after surgical resection,20,62 suggesting the importance of regular follow-up after treatment. Obiorah et al. 23 reported a case of primary hepatic MALT lymphoma that developed pulmonary MALT lymphoma 1 year after surgical resection and parotid MALT lymphoma after 7 years. Chen et al. 63 reported a patient with primary hepatic MALT lymphoma who developed pulmonary MALT lymphoma 8 years after surgery. Although the disease usually progresses slowly, 64 it may relapse after many years and involve other common external nodes. Therefore, clinicians should be alert to the possibility of distant metastasis, and regular follow-up is recommended even after 5 years postoperatively.
To the best of our knowledge, only one Japanese patient with primary hepatic MALT lymphoma has received RFA treatment. 17 In our case, RFA was performed after confirming a malignant liver tumor. Postoperative imaging results indicated good efficacy with surgery. The patient was regularly followed-up for 1 year after surgery, and showed no signs of recurrence. Our case indicates that RFA is safe and effective in the treatment of primary hepatic MALT lymphoma in the short-term, while avoiding unnecessary liver resection. However, long-term follow-up and more relevant cases are needed to observe the effect of RFA on long-term survival. As seen in our case, when the tumor is confirmed by pathological biopsy, non-resection therapies, such as RFA, can be selected. Our case indicates a new option for the treatment of hepatic MALT lymphoma.
Conclusions
According to our case and the previous literature, primary hepatic MALT lymphoma is usually identified incidentally, and the disease has no characteristic imaging manifestations. Hence, preoperative diagnosis remains a great challenge. Although there is no standard management model for this rare disease, patients who undergo surgery, chemotherapy, or radiotherapy experience good efficacy and prognosis. Our case received RFA for primary hepatic MALT lymphoma, which showed good efficacy. The effect of RFA on long-term survival requires further follow-up observation, and greater numbers of case reports and multi-center studies are needed to provide detailed clinical information to improve the current understanding of the disease.
Footnotes
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Ethics statement
The study protocol was approved by the Ethics Committee of The Second Hospital of Dalian Medical University (approval no: 2020. 050). The patient provided written informed consent.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.