
Abstract
Objective
This study was performed assess the clinical outcomes of elderly patients with osteoporotic femoral neck fractures (FNFs) (AO/OTA: 31B/C) treated by initial uncemented total hip arthroplasty (UTA) or cemented total hip arthroplasty (CTA).
Methods
This study involved consecutive elderly patients with osteoporotic FNFs (AO/OTA: 31B/C) treated by initial UTA or CTA in our medical centre from 2010 to 2015. The primary outcomes were the Harris hip score (HHS) and the rates of revision, loosening, periprosthetic fracture, and dislocation.
Results
In total, 224 patients were included in the final analysis (UTA, n = 114; CTA, n = 110). The mean follow-up duration was 60 months (range, 32–68 months). The mean HHS was 75.34 ± 18.82 for UTA and 80.12 ± 17.83 for CTA. Significant dissimilarities were detected in the rates of revision, loosening, and periprosthetic fracture between UTA and CTA (14.0% vs. 5.5%, 20.2% vs. 10.0%, and 12.3% vs. 4.5%, respectively). A significant difference was also detected in the probability of revision between the two groups.
Conclusion
Elderly patients with osteoporotic FNFs (AO/OTA: 31B/C) treated with CTA show greater improvements in functional outcomes and key orthopaedic complications than those treated with UTA.
Introduction
Management of femoral neck fractures (FNFs) (AO/OTA: 31B/C) in elderly patients is still undergoing considerable research. 1 , 2 Uncemented total hip arthroplasty (UTA) or cemented total hip arthroplasty (CTA) for displaced FNFs tends to be a recognised surgical strategy.3–5 Comparisons between UTA and CTA for elderly individuals with an FNF generally favour CTA; this is primarily attributed to the exceptional clinical outcomes of CTA in terms of relieving pain and improving daily activities as well as the higher rate of major orthopaedic complications (i.e., revision, loosening, periprosthetic fracture, and dislocation) associated with UTA. 4 However, recent studies of UTA in elderly individuals have demonstrated encouraging short-term clinical outcomes.6,7 Moreover, cemented prosthesis syndrome tends to occur more frequently in CTA than UTA. 8 Cemented prosthesis syndrome theoretically poses a significant threat to the patient’s life, although the specific probability of this threat has not been calculated.8,9 Hence, whether to utilise CTA for elderly individuals may present the clinician with a dilemma. 9 The lack of consensus regarding which technique (UTA or CTA) is preferable for treating FNFs (AO/OTA: 31B/C) in elderly individuals is related to the remarkable distinction in clinical outcomes between the two types of implants.6,10
Most previous studies have involved highly concentrated medical centres and several brands of prostheses.3,5,6 Additionally, short-term follow-up is commonplace in these studies. To overcome these drawbacks of previous studies and to compare the mid-term results of the two prostheses, we assessed the clinical outcomes of elderly patients with osteoporotic FNFs (AO/OTA: 31B/C) treated with initial UTA or CTA with a mean follow-up of 5 years.
Materials and methods
Study population
Ethical approval was obtained from the First Affiliated Hospital of Sun Yat-sen University, and the requirement for informed consent was waived by the Investigational Review Board. Consecutive elderly individuals with the principle diagnosis of an FNF (AO/OTA: 31B/C) who underwent initial UTA or CTA from 1 March 2010 to 31 March 2015 and for whom detailed information was available throughout follow-up were identified from the orthopaedics department of the First Affiliated Hospital, Sun Yat-sen University. The manufacturer details of the stems and cups employed in the arthroplasty are shown in Table 1. The surgical procedure and postoperative rehabilitation protocol were described in our previously published study. 11 The inclusion criteria were closed FNFs (AO/OTA: 31B/C), active and cognitively intact patients, age of ≥65 years, independently mobile prior to the injury, and a bone mineral density T-score of <−2.5 at the femoral neck. The major exclusion criteria were multiple fractures or contralateral limb fractures, pathological FNFs, lower limb dyskinesia prior to surgery, cancer, planned surgery, polytrauma, severe comorbidities (e.g., thyroid disorder with calcium and phosphorus metabolism disorder, diabetes with complications), drug abuse affecting bone healing or bone metabolism, early interruption of follow-up (<12 months), and cognitive impairment. Clinical and radiographic assessments were performed at 3, 6, and 12 months after surgery and every 12 months thereafter. The primary outcomes were the Harris hip score (HHS) and the rates of revision, loosening, periprosthetic fracture, and dislocation.
Manufacturer details of stems and cups employed in the arthroplasty procedures.
1DePuy Synthes, Warsaw, IN, USA.
2Smith & Nephew, London, UK.
3Stryker Corporation, Kalamazoo, MI, USA.
UTA, uncemented total hip arthroplasty; CTA, cemented total hip arthroplasty.
Statistical analysis
Revision was defined as partial or complete replacement of the prosthesis. 12 Loosening of the acetabulum and/or stem components as well as dislocation were defined based on a previous description. 13 Periprosthetic fracture was confirmed by X-ray or computed tomography examination. Continuous data (i.e., age, bone mineral density, body mass index, follow-up time, and HHS) were compared using an independent-samples t test, and categorical variables (i.e., sex, side [left/right], fracture type, comorbidities, mechanism of injury, American Society of Anesthesiologists classification, and major orthopaedic complications) were compared using the chi-square test or the Mann–Whitney test. A Kaplan–Meier survival curve was used to assess the probability of revision. Hazard ratios were calculated using a Cox proportional hazards model. The significance threshold was set at p < 0.05. The statistical analysis was performed using SPSS 25 (IBM Corp., Armonk, NY, USA).
Results
In total, 224 consecutive patients (224 arthroplasties) with an FNF (AO/OTA: 31B/C) who underwent initial UTA or CTA met our inclusion criteria and were included for analysis (Figure 1). The mean follow-up duration was 60 months (range, 32–68 months). The patients’ mean age was 68.52 ± 7.79 years for UTA and 68.88 ± 8.15 for CTA. The mean body mass index was 25.78 ± 5.64 kg/m2 for UTA and 25.91 ± 6.22 kg/m2 for CTA. The patients’ baseline characteristics were similar between the two groups (Table 2).

Flow diagram exhibiting methods for identifying patients with FNFs (AO/OTA: 31B/C) who underwent an initial UTA or CTA.
Patient demographics and outcomes.

Data are presented as n, n (%), or mean ± standard deviation.
UTA, uncemented total hip arthroplasty; CTA, cemented total hip arthroplasty; HHS, Harris hip score; ASA, American Society of Anesthesiologists; BMI, body mass index; BMD, bone mineral density; FNFs, femoral neck fractures.
Primary outcomes
Improved functional outcomes were noted in both groups as indicated by the HHS (UTA: 57.22 ± 16.78 prior to surgery vs. 75.34 ± 18.82 at final analysis, p < 0.001; CTA: 57.54 ± 17.68 prior to surgery vs. 80.12 ± 17.83 at final analysis, p < 0.001). At the end of follow-up, the HHS was significantly different between the two groups (UTA: 75.34 ± 18.82 vs. CTA: 80.12 ± 17.83, p = 0.007), and patients who underwent CTA had higher functional scores than those who underwent UTA. No distinct between-group differences were observed at any time point before 24 months postoperatively (Table 3).
Comparison of hip functional scores.

Data are presented as mean ± standard deviation.
*Statistically significant
UTA, uncemented total hip arthroplasty; CTA, cemented total hip arthroplasty.
No early (<1 year) postoperative complications were detected, including revision, loosening, periprosthetic fracture, or dislocation. The rate of key orthopaedic complications was 52.6% (60/114) for UTA and 24.5% (27/110) for CTA (p < 0.001) (Table 4). In the UTA group, 16 (14.0%) patients underwent revision UTA, 23 (20.2%) developed prosthesis loosening, 14 (12.3%) developed periprosthetic fractures, and 7 (6.1%) developed prosthesis dislocation. In the CTA group, 6 (5.5%) patients underwent revision UTA, 11 (10.0%) developed prosthesis loosening, 5 (4.5%) developed periprosthetic fractures, and 5 (4.5%) developed prosthesis dislocation. The average time interval from the initial surgery to revision UTA was 27 months (range, 18–56 months) for UTA and 32 months (range, 23–54 months) for CTA (p = 0.012). Significant differences in revision, loosening, and periprosthetic fracture were observed between the UTA and CTA groups (revision: 14.0% vs. 5.5%, p = 0.031; loosening: 20.2% vs. 10.0%, p = 0.034; and periprosthetic fracture: 12.3% vs. 4.5%, p = 0.038, respectively). A significant difference in the probability of revision was also detected between the groups (hazard ratio, 0.35; 95% confidence interval, 0.16–0.79; p = 0.0203) (Figure 2). No significant difference was found in the rate of prosthesis dislocation between the UTA and CTA groups (6.1% vs. 4.5%, respectively).
Rates of key orthopaedic complications.

Data are presented as n (%).
*Statistically significant.
UTA, uncemented total hip arthroplasty; CTA, cemented total hip arthroplasty.
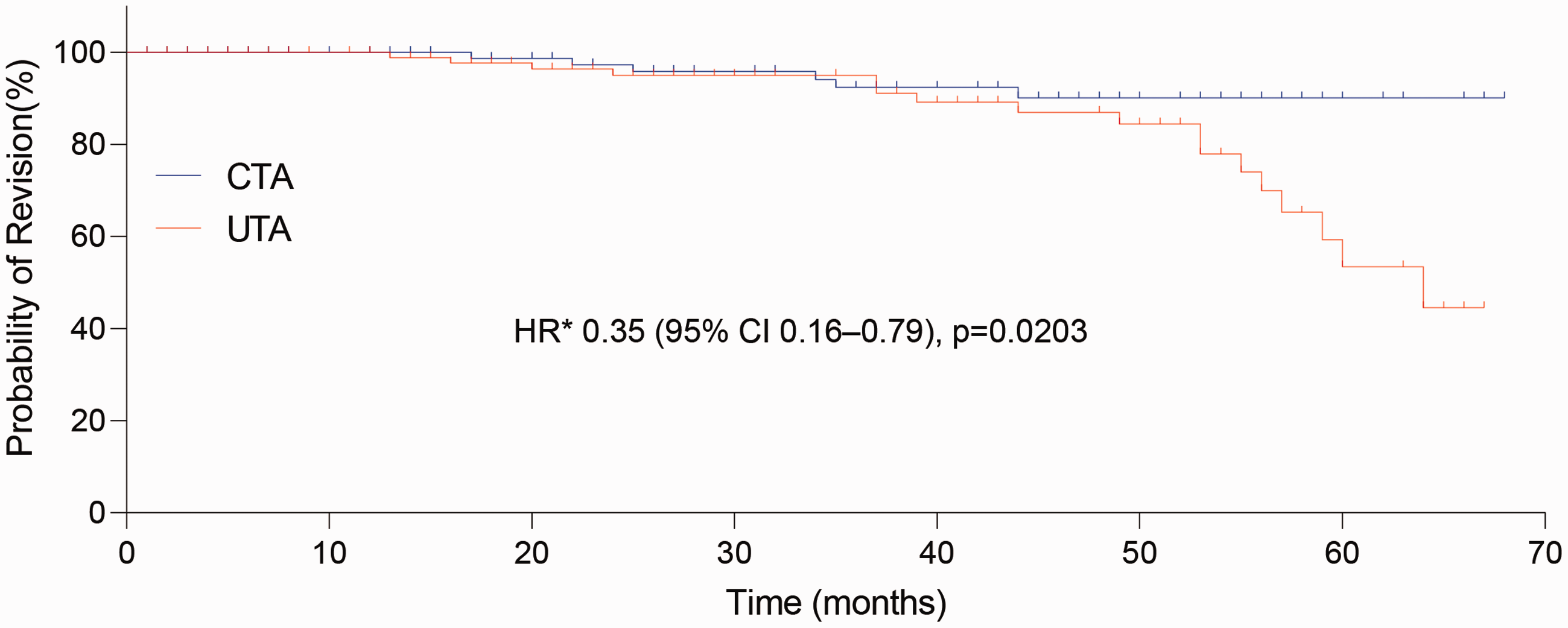
Kaplan–Meier curves showing probability of revision after primary surgery. *HR was calculated per the Cox proportional hazards model, with age, sex, American Society of Anesthesiologists classification, body mass index, bone mineral density, and femoral neck fracture type as covariates and surgery as the time-dependent factor.
Discussion
This review characterised the outcomes of a solitary brand of a total hip arthroplasty implant during a mean follow-up of 5 years in elderly patients with osteoporotic FNFs (AO/OTA: 31B/C). The data demonstrated that patients treated with CTA showed better improvements in functional outcomes and key orthopaedic complications than those treated with UTA.
The current findings are consistent with previous studies.3,6,14,15 Although the better functional outcomes and lower rates of revision, loosening, periprosthetic fracture, and dislocation are apt to favour CTA, no significant between-group differences in the HHS were detected during the initial 2 years after surgery. Probable explanations include the time-dependent clinical efficacy of the implants and the properties of the prostheses.3,4,6,16 Whether UTA or CTA is preferable in elderly patients with a displaced FNF remains controversial.6,9,17 A recent retrospective study involving 324 patients with an FNF (AO/OTA, 31B) who underwent primary unilateral UTA or CTA showed that the mean HHS was 74.09 ± 6.23 for CTA and 79.01 ± 10.21 for UTA (p = 0.012). 17 A single-blinded randomised controlled trial (CHANCE-trial) involving 140 individuals treated with an uncemented or cemented tapered hydroxyapatite-coated femoral stem and a cemented cup demonstrated that the cemented tapered hydroxyapatite-coated femoral stem and cemented cup provided better functional results than the uncemented tapered hydroxyapatite-coated femoral stem and cemented cup. 16
In the present study, the Kaplan–Meier survival curve demonstrated that at the 2-year analysis, neither group showed evidence of a target event, and no significant between-group differences were found in the rates of revision, loosening, periprosthetic fracture, or dislocation. Nevertheless, it would be interesting to explore whether the prosthesis material influences the bone microstructure, the peak effect, and the duration of the effect, and if so, what mechanisms affect the bone microstructure and whether there is a way to change the outcome by blocking this effect during a >2-year follow-up. We currently have one option for prevention or avoidance of adverse events, and these changes in treatment strategies may play a key role in improving the clinical results (if the effects of the prosthesis material itself cannot be blocked). 18 There is still a lack of consensus on standards for prosthesis revision in this context. 19
When assessing the impact of CTA on the target events, we did not observe an increased incidence of severe orthopaedic complications other than the complications mentioned in this study. In one systematic review, the authors presumed that CTA was superior to UTA with respect to functional scores and tolerable orthopaedic complications 20 We obtained analogous results in terms of hip-related complications and functional scores. Multi-centre hip arthroplasty data indicate that UTA remains a high-risk factor for late revision, loosening, and periprosthetic fractures.8,10 The notable dissimilarities in the results of these various studies on hip-related complications may be largely attributed to the design of the prosthesis (prosthesis size and material selection) and the surgeon’s experience.4,6
This study has several limitations. It had a small sample, and its retrospective design is association with some inherent disadvantages. We did not stratify the patients according to fracture type or sex. In addition, the potential comorbidities between groups were not well exposed and compared. The statistical power used to address differences between the groups was insufficient. Differences in the patients’ baseline data may have affected the results. Furthermore, our analysis did not determine whether the deaths were instigated by bone cement. The risk of hip-related complications was not analysed. The survival curve of other prosthesis-related complications was estimated using the Kaplan–Meier method, and competitive risks (i.e., death) could have affected the survival of the prosthesis. Patients who died lost the opportunity for revision. Hence, the revision rate might have been underestimated during this long follow-up with a fairly high mortality rate.
In conclusion, the findings described in the current review uphold an increasing body of evidence that CTA provides higher functional scores and lower rates of hip-related complications than does UTA in elderly patients with osteoporotic displaced FNFs (AO/OTA: 31B/C). In this context, we recommend CTA for the treatment of such FNFs. Our findings may be conducive to alleviating continuing debate regarding which prosthesis (UTA or CTA) is more suitable for the elderly population. A future prospective study may be essential to confirm whether our conclusion continues to be acceptable as the follow-up time increases.