
Abstract
Objective
To undertake a meta-analysis to investigate if there is an association between the glutathione S-transferase mu 1 (GSTM1) gene polymorphism, coronary artery disease (CAD) susceptibility and smoking.
Methods
Electronic databases, including PubMed®, Web of Science and Embase®, were searched for relevant case–control studies. Data were extracted and the odds ratio (OR) was calculated and appropriate statistical methods were used for the meta-analysis.
Results
The analysis included eight studies with a total of 1880 cases with CAD and 1758 control subjects. The results of this meta-analysis demonstrated that there is no association between the GSTM1 null and CAD (OR 1.24, 95% confidence interval [CI] 1.00, 1.55). An increased risk of CAD was observed in the smoking population with the GSTM1 null genotype (OR 1.48, 95% CI 1.02, 2.15). Subgroup analyses of geographical region, genotyping method and publication language category demonstrated potential relationships among gene polymorphism, smoking and CAD.
Conclusions
Based on the current literature, the GSTM1 null genotype was associated to CAD in the smoking population. The interaction between smoking and GSTM1 polymorphism may contribute to the susceptibility of CAD.
Keywords
Introduction
Coronary artery disease (CAD) is one of the leading causes of death worldwide.1,2 It is well known that the development of CAD is influenced by many factors such as hypertension, an unbalanced diet, ageing, smoking, diabetes mellitus and dyslipidaemia.3,4 Among these factors, smoking is a recognized risk factor for CAD, which has been confirmed by many studies.5–7 Chemicals in cigarette smoke can lead to oxidative stress, an inflammatory reaction of the coronary artery tissues, increased levels of DNA adducts and acceleration of the progression of atherosclerotic lesions.4,8 However, not all heavy smokers suffer from CAD.9–11 During cigarette combustion, compounds are released and cause a toxic reaction. 12 Glutathione S-transferase (GST) genes can interfere in the binding of chemical compounds to DNA.13,14 The GST gene family consists of a group of phase II metabolism genes and they play an important protective role in cells. 15 Glutathione S-transferase mu 1 (GSTM1) is the most widely expressed metabolic gene in the GST gene family. 16 Activation of the GSTM1 gene protects cells against toxic substances. 17 In humans, it is reported that the GSTM1 null genotype is related to a group of diseases.18–21
Various studies have been performed to explore the association between GSTM1 gene polymorphisms and CAD.22–29 Of these, some studies reported that the GSTM1 null genotype was related to CAD in a smoking population,24,26 while several reports showed no significant association between the two factors.22,23,25,27–29 Based on existing studies,22–29 a meta-analysis was conducted to investigate if there is an association between GSTM1 gene polymorphism, CAD susceptibility and smoking.
Materials and methods
Search strategy
Electronic databases, including PubMed®, Web of Science and Embase®, were searched from inception to 31 October 2021 to identify relevant studies using the following keywords: “coronary artery disease (CAD)”, “coronary atherosclerotic lesions”, “myocardial infarction (MI)”, “glutathione S-transferase M1 (GSTM1)”, “polymorphism” and “smoking”. Two independent investigators (M.L. & Y.G.) screened the relevant studies according to the standardized screening guide. Articles meeting the inclusion and exclusion criteria were included in this meta-analysis.
Inclusion and exclusion criteria
The inclusion criteria were as follows: (i) studies on the relationship between GSTM1 and CAD; (ii) case–control studies; (iii) CAD was diagnosed by angiography; (iv) published in English; (v) sufficient data to calculate odds ratio (OR) and the corresponding 95% confidence intervals (CIs). The exclusion criteria were as follows: (i) abstracts, comments, letters, case reports and family-based studies were excluded; (ii) articles with insufficient data.
Quality assessment
A modified scoring system (range, 0–10 points) was used to evaluate the quality of eligible studies (Table 1).13,30 High quality articles received a higher score. The mean score of all the enrolled studies was 7.375 points.
Quality criteria for eligible studies included in a meta-analysis to evaluate the relationship between glutathione S-transferase mu 1 (GSTM1) gene polymorphism, coronary artery disease (CAD) and smoking.
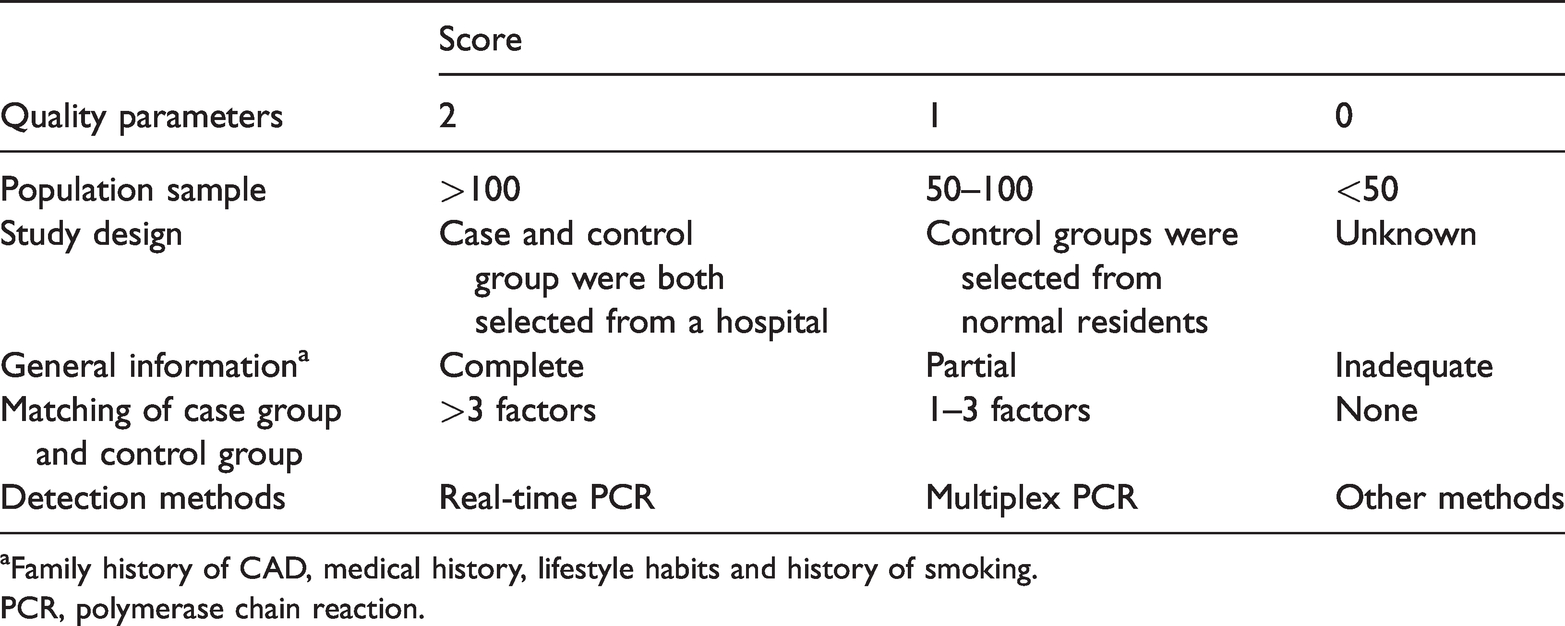
Family history of CAD, medical history, lifestyle habits and history of smoking.
PCR, polymerase chain reaction.
Data extraction
Data were extracted by two investigators (M.L. & Y.G.) independently and any disagreement was settled by discussion. Data extracted included: last name of the first author, published year, country, ethnicity, number of cases and controls, genotyping method, control sources and genotype distribution.
Statistical analyses
Statistical analyses were performed with STATA® version 12.0 software (STATA Corp., College Station, TX, USA). Pooled ORs and 95% CIs were calculated using the data from the included articles using a random-effect model (Mantel–Haenszel method heterogeneity method) or a fixed-effect model (Mantel–Haenszel method). The heterogeneity among the included studies was assessed with the I2 index. The χ2-test and P-value were the main evaluation parameters. 31 ORs were estimated by the random-effect model if significant heterogeneity existed (P < 0.05 and/or I2 > 50%), 32 while the fixed-effect model was used if there was no significant heterogeneity. 33 A P-value <0.05 was considered statistically significant. The influence of individual studies was assessed by a sensitivity analysis and publication bias was evaluated by Begg’s test. 34
Results
A flow chart showing the study selection process is presented in Figure 1. Eight studies were enrolled into this meta-analysis according to the inclusion and exclusion criteria.22–29 A total of 1880 cases with CAD and 1758 controls were included in the meta-analysis. The clinical characteristics and the GSTM1 genotype distribution of cases with CAD and controls are shown in Table 2.
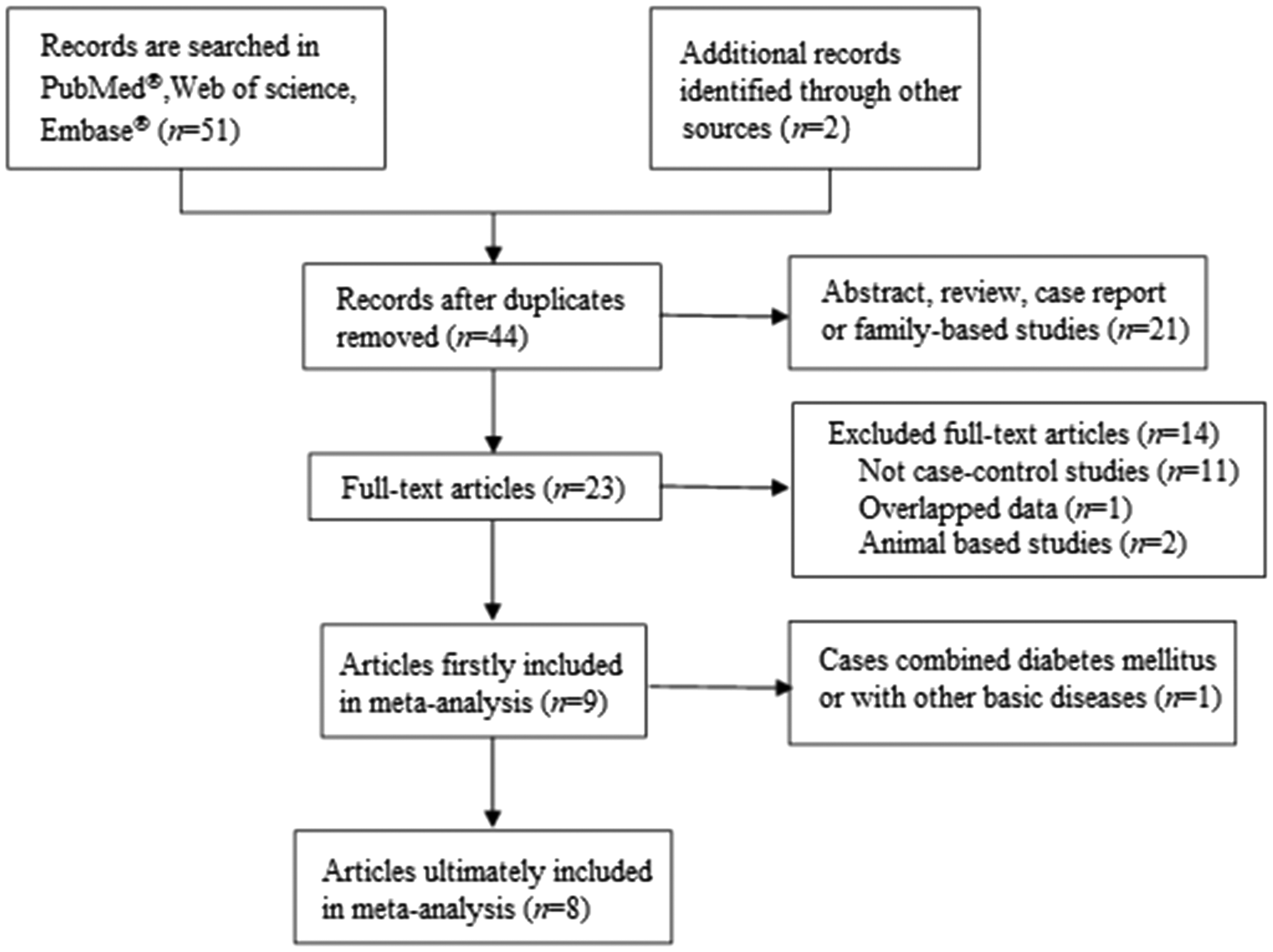
Flow chart of the eligible studies included in this meta-analysis.
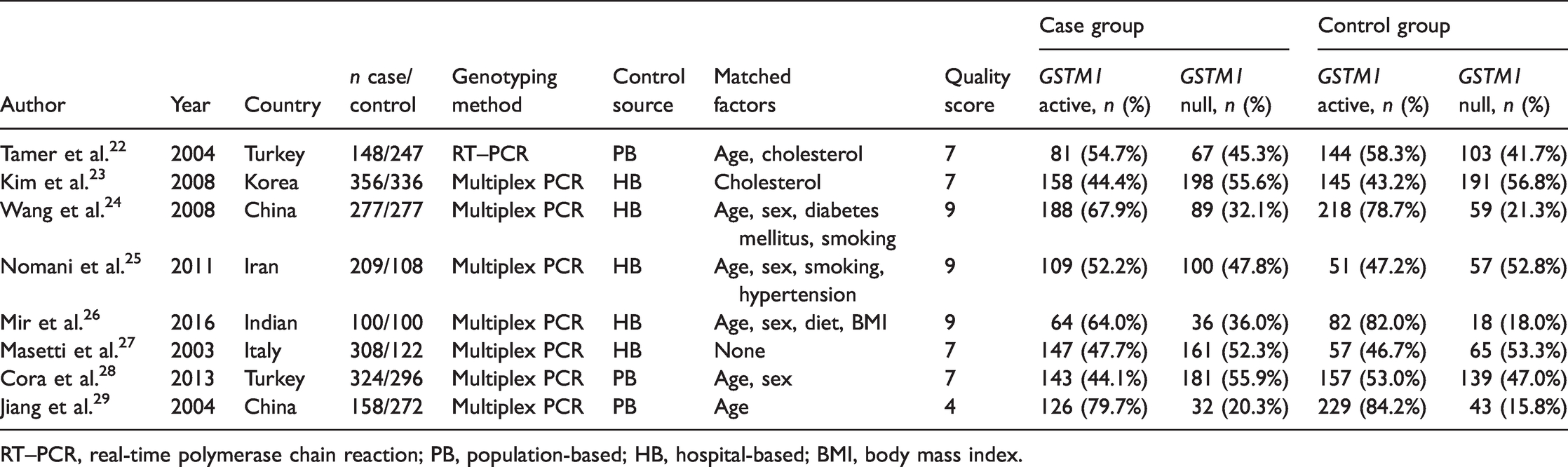
RT–PCR, real-time polymerase chain reaction; PB, population-based; HB, hospital-based; BMI, body mass index.
There was a significant difference in the between-study heterogeneity of the eight enrolled studies (P = 0.023, I2 = 56.8%; Figure 2), so the strength of the relationship between GSTM1 null genotype and CAD risk was assessed by the random-effect model. The pooled OR of GSTM1 null in patients with CAD was 1.24 compared with the control group (95% CI 1.00, 1.55, Figure 2), which indicated that GSTM1 null was not necessarily associated with CAD. The pooled OR of GSTM1 null in the smoking population was calculated (OR 1.48). An increased risk of CAD was found in the smoking population with the GSTM1 null genotype (95% CI 1.02, 2.15, P = 0.040, Figure 3A). The risk of CAD did not increase in the non-smoking population with the null genotype of GSTM1 (OR 1.13, 95% CI 0.86, 1.50; Figure 3B).


Subgroup analyses were conducted by region, genotyping method and publishing language in both the smoking and non-smoking populations (Table 3). Results from the subgroup analysis stratified by region indicated that the GSTM1 null genotype was associated with CAD susceptibility in non-eastern Asian people that currently smoke or ever smoked (OR 1.467, 95% CI 1.008, 2.135, P = 0.045), but it was not associated in smokers in eastern Asia (OR 1.427, 95% CI 0.589, 3.458, P = 0.431). With regard to the genotyping method subgroup analysis, using multiplex polymerase chain reaction (PCR) in the smoking population increased the risk of CAD (OR 1.784, 95% CI 1.136, 2.801, P = 0.012), while GSTM1 null non-smoking patients were not at a higher risk of CAD if multiplex PCR was used (OR 1.509, 95% CI 0.767, 1.436, P = 0.728). When publishing language was considered, results from studies published in English showed a significant association between the GSTM1 null genotype and CAD risk in smokers (OR 1.607, 95% CI 1.084, 2.381, P = 0.018). When subgroup analyses were conducted by region, genotyping method and publishing language in the non-smoking population, no statistical correlation was found between GSTM1 polymorphism and CAD.
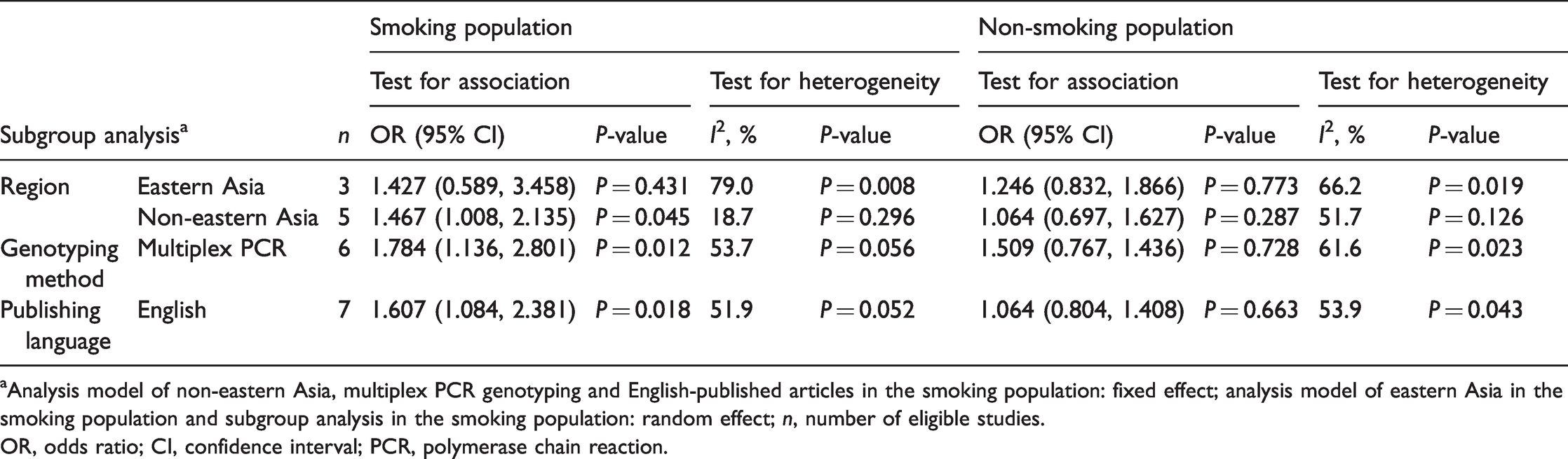
aAnalysis model of non-eastern Asia, multiplex PCR genotyping and English-published articles in the smoking population: fixed effect; analysis model of eastern Asia in the smoking population and subgroup analysis in the smoking population: random effect; n, number of eligible studies.
OR, odds ratio; CI, confidence interval; PCR, polymerase chain reaction.
Begg’s test showed that there was no obvious evidence of publication bias (P = 0.417) (Figure 4). Sensitivity analysis was conducted using the command “metaninf” of the STATA® version 12.0 software to evaluate the effects of each study on the pooled OR. New combined ORs were produced after each study was removed from the pooled analysis. Compared with the original pooled ORs, the results showed no significant differences (Figure 5).


Discussion
The association of CAD and gene polymorphism has been researched in the past three decades,35,36 but this is the first meta-analysis to focus on the association of GSTM1 gene polymorphism, CAD susceptibility and smoking. The development of CAD is affected by many factors. Among these risk factors, genetic polymorphism has become a focus of research. A large number of studies show that GST genes play a crucial role in the aetiology of CAD.37,38 GSTM1 is the most common type of GST gene.39,40 Some research reported that the GSTM1 polymorphism was associated with increased risk of CAD.24,26,28 However, other reports suggested that there was no relationship between GSTM1 polymorphism and CAD.22,23,25,27,29 After comprehensively analysing the data retrieved from these studies, the results of this meta-analysis revealed that GSTM1 null is not associated with an increased risk of CAD. However, this current meta-analysis also demonstrated that GSTM1 null was significantly associated with CAD risk in smokers, but not in non-smokers. Cigarette combustion increases the formation of chemicals associated with the development of CAD. 8 However, individual susceptibility to CAD varies. For example, only 30–50% of smokers develop CAD, suggesting that genetic factors play an important role.9–11 GSTM1 active is involved in the metabolism of xenobiotics and facilitates the protection of cells from oxidative reactions. 17 Furthermore, some non-smokers with GSTM1 null develop CAD.26,29 This indicates that exogenous chemical exposure is also very important to the incidence of CAD. Smokers with the GSTM1 active genotype and non-smokers with the GSTM1 null genotype are less likely to have CAD.22,23 However, CAD incidence increases significantly when the null genotype of GSTM1 interacts with smoking.24,26
This meta-analysis was up-to-date and the search strategy was designed carefully. Studies focused on GSTM1 polymorphism, smoking and the risk of CAD were selected from three databases (PubMed®, Web of Science and Embase®). Two investigators also screened the grey literature to eliminate publication bias. The number of participants in the recruited studies was large. The results were generated through appropriate statistical analyses. Sensitivity and subgroup analyses were also performed to control the confounding factors. However, there were some limitations in this current meta-analysis. First, the quality of the articles was variable. Secondly, different geographical regions were analysed in the subgroup analysis, but few studies of eastern Asian participants were found in the search process and the unbalanced ethnic proportion may have affected the results of this work. The identified Master's dissertation belongs to the grey literature and it was included in this meta-analysis. 29 Since this grey literature has not been reviewed by experts, its authority, validity and quality are uncertain, which may have an impact on the results of this meta-analysis. This shortcoming of the grey literature cannot be ignored. Thus, further well-designed studies focusing on eastern Asian populations with larger sample sizes are needed to clarify the present findings.
In conclusion, this updated meta-analysis found that GSTM1 null was associated with an increased risk of CAD in the smoking population. Subgroup analysis of geographical region, genotyping method and publishing language also suggested that GSTM1 null was a prominent risk factor of CAD in smokers. Therefore, GSTM1 polymorphism is related to the development of CAD when humans are exposed to smoking.
Footnotes
Author contributions
M.L. and Y.G. were responsible for the conception, study design and acquisition of data; Y.G. and X.N. drafted the initial manuscript and revised it critically for important intellectual content; M.L., J.M., K.B. and L.A. analysed and interpreted the data. M.L. wrote the final draft. All authors read and approved the final manuscript.
Declaration of conflicting interest
The authors declare that there are no conflicts of interest.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the Key Subjects of Jiading District (no. 2020-jdyxzdxk-04) and Shanghai Municipal Jiading District Health Commission Foundation (no. 2020-QN-07).