
Abstract
Objective
To analyze the clinical features, efficacy of antibiotic treatment, and outcome of neonatal listeriosis.
Methods
This was a retrospective study that included all neonates diagnosed with listeriosis between January 2010 and December 2021.
Results
Nine male patients and five female patients were analyzed, including 11 preterm and 3 term infants. The mean gestational age was 34 ± 2.6 weeks (29 + 2–40 + 2 weeks), and the mean birth weight was 2392 ± 603 g (1370–3580 g). The maternal clinical manifestations included fever (13/14 [92.9%]), meconium-stained amniotic fluid (12/14 [85.7%]), and intrauterine fetal distress (11/14 [78.6%]). The neonates presented with fever (14/14 [100%]), generalized maculopapular rash (7/14 [50%]), and convulsions (8/14 [57.1%]). Laboratory tests showed leukocytosis (11/14 [78.6%]), monocytosis (9/14 [64.3%]), elevated C-reactive protein levels (13/14 [92.9%]), and thrombocytopenia (6/14 [42.9%]). Eight patients had central nervous system involvement, and Listeria monocytogenes was isolated from the blood in all cases. Empiric antibiotic therapy consisted of a combination of third-generation cephalosporins and penicillin or vancomycin. Four patients died, and 10 patients were cured.
Conclusions
Preterm infants were more susceptible to listeria infection than term infants, with most having multiple organ injuries. Combined antibiotic application improved the effectiveness of treatment.
Introduction
Neonatal listeriosis is the most common form of human listeriosis and is associated with a high case fatality rate of up to 50%.1–3 It is the third leading cause of neonatal meningitis worldwide.3,4 Neonatal listeriosis is characterized by early presentation and manifests as bacteremia, pneumonia, and, rarely, meningitis. The late-onset form is mostly observed in term infants born to asymptomatic mothers and presents as meningitis rather than sepsis.5–8
Ampicillin combined with an aminoglycoside is recommended for the treatment of listeriosis. Listeria monocytogenes (L. monocytogenes) is not susceptible to cephalosporins commonly used for empiric treatment of bacterial infections. 9 Consequently, penicillin or ampicillin is generally included in the empiric antibiotic therapy for infants with bacterial sepsis or meningitis to combat pathogens of most concern, including L. monocytogenes.1,10 Despite appropriate antibiotic treatment, mortality caused by listeriosis remains high among neonates. Here, we retrospectively analyzed the treatment process and prognosis of neonatal listeriosis to describe the clinical characteristics and relevant treatment experience of this disease.
Methods
This retrospective study was conducted at the First Affiliated Hospital of Xi'an Jiaotong University, Shaanxi, China. Cases of neonatal listeriosis treated between January 2010 and December 2021 were extracted from computerized medical records in the hospital information system using a standardized data collection form. The reporting of this study conforms to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines. 11 All patients were diagnosed in accordance with the diagnostic criteria for neonatal early-onset sepsis established by the Neonatal Group of the Pediatrics Society of the Chinese Medical Association in 2003 for clinical manifestations of infection and L. monocytogenes in blood culture or a sterile body cavity. 12 The study was approved by the ethics committee of the First Affiliated Hospital of Xi'an Jiaotong University (2021-G-86). The information obtained for each patient included the maternal history, patient demographics, clinical presentation, microbiological and laboratory results, imaging results, treatment, and outcomes. Because this was a retrospective observational study, patient informed consent was not required.
After the neonates were admitted to the neonatal intensive care unit (NICU), blood gas, routine blood, blood culture, C-reactive protein, and biochemical examinations were carried out, and any changes were closely monitored. Lumbar puncture was performed in nine patients for cerebrospinal fluid (CSF) examination. Bacterial culture and drug sensitivity tests were performed according to the standard procedures described by the National Clinical Laboratory Operations Guideline. 13 No formal statistical analysis was applied.
Results
Fourteen neonates, including nine (64%) males and five (36%) females, were identified. Eleven (79%) were preterm and three (21%) were full term, with a mean gestational age of 34 ± 2.6 weeks (range 29 + 2–40 + 2 weeks). All infants had a birth weight appropriate for gestational age (range 1370–3580 g). The mothers' ages ranged between 22 and 40 years. Two mothers had a clear history of consumption of uncooked meat, and one mother had a long-term history of exposure to cattle during pregnancy. Thirteen (93%) mothers presented with maternal pyrexia prior to delivery, and three (21%) had flu-like symptoms. Eight (57%) infants were born via caesarean section, and six (43%) were born via vaginal delivery. In 12 cases (86%), meconium-stained amniotic fluid was observed, and 11 (79%) patients had intrauterine fetal distress. The age of onset was within 3 days in all 14 (100%) infants. All infants developed fever of varying degrees; seven infants (50%) developed a maculopapular rash, and eight infants (57%) presented with intermittent convulsions. Ten (71%) patients presented with asphyxia or respiratory distress requiring endotracheal intubation in the delivery room. An overview of prenatal data and neonatal characteristics is shown in Table 1.
Maternal and neonatal characteristics of 14 cases of neonatal listeriosis.

DOB, date of birth; GA, gestational age; BW, birth weight; MSL, meconium-stained liquor; PROM, premature rupture of membrane; MOD, mode of delivery; POD, place of delivery; CS, caesarean section; VD, vaginal delivery.
Initial laboratory examinations revealed leukocytosis (16.5–48.1 × 109/L) in 11 (79%) and elevated C-reactive protein levels (10.6–183 mg/L) in 13 (93%) infants. An elevated mononuclear cell count (8.2%–44.7%) and thrombocytopenia (26–92 × 109/L) were observed in six infants each (64%). Aspartate transaminase and creatine kinase-muscle/brain levels were significantly elevated in 10 (71%) infants, with peak values of 970 U/L and 2279 U/L, respectively. These values gradually normalized after appropriate treatment. CSF examination confirmed purulent meningitis in eight (57%) infants with pleocytosis and hypoglycorrhachia. Furthermore, placental pathology examinations revealed acute chorioamnionitis in three (21%) patients. All infants underwent chest X-ray examination on the day of admission, and the results were consistent with neonatal pneumonia. Cranial magnetic resonance imaging revealed ventriculomegaly of the lateral ventricles, intracranial hemorrhage, or cystic periventricular leukomalacia (Table 2).
Laboratory test results and cranial MRI findings in the 14 cases of neonatal listeriosis.

AST, aspartate aminotransferase; CKMB, creatine kinase-muscle/brain; CRP, C-reactive protein; CSF, cerebrospinal fluid; MO, monocyte; MRI, Magnetic resonance imaging; NP, not performed; WBC, white blood cell count.
On admission to the NICU, 10 (71%) patients required ventilator support, and five (35%) patients were treated with pulmonary surfactant because of respiratory distress. Eight (57%) patients were treated with phenobarbital (loading dose 20 mg/kg, maintenance dose 5 mg/kg) because of intermittent convulsions. However, in Case 4 and 8, convulsion control was not satisfactory, and these patients were successfully treated with midazolam given as an intravenous bolus dose (0.15 mg/kg/hour) followed by continuous intravenous infusion for 26 hours and 37 hours, respectively. Empiric antibiotic treatment consisted of a third-generation cephalosporin plus penicillin/vancomycin in all cases. After obtaining a positive blood culture for gram-positive bacilli, subsequently identified as L. monocytogenes, meropenem was substituted for the third-generation cephalosporin. L. monocytogenes was isolated from this case series and was susceptible in vitro to penicillin, meropenem, vancomycin, and linezolid. The average duration of antibiotic therapy for the nine (64%) patients treated in our hospital was 27.2 ± 4.7 days (Table 3).
Treatment and outcome of the 14 cases of neonatal listeriosis.
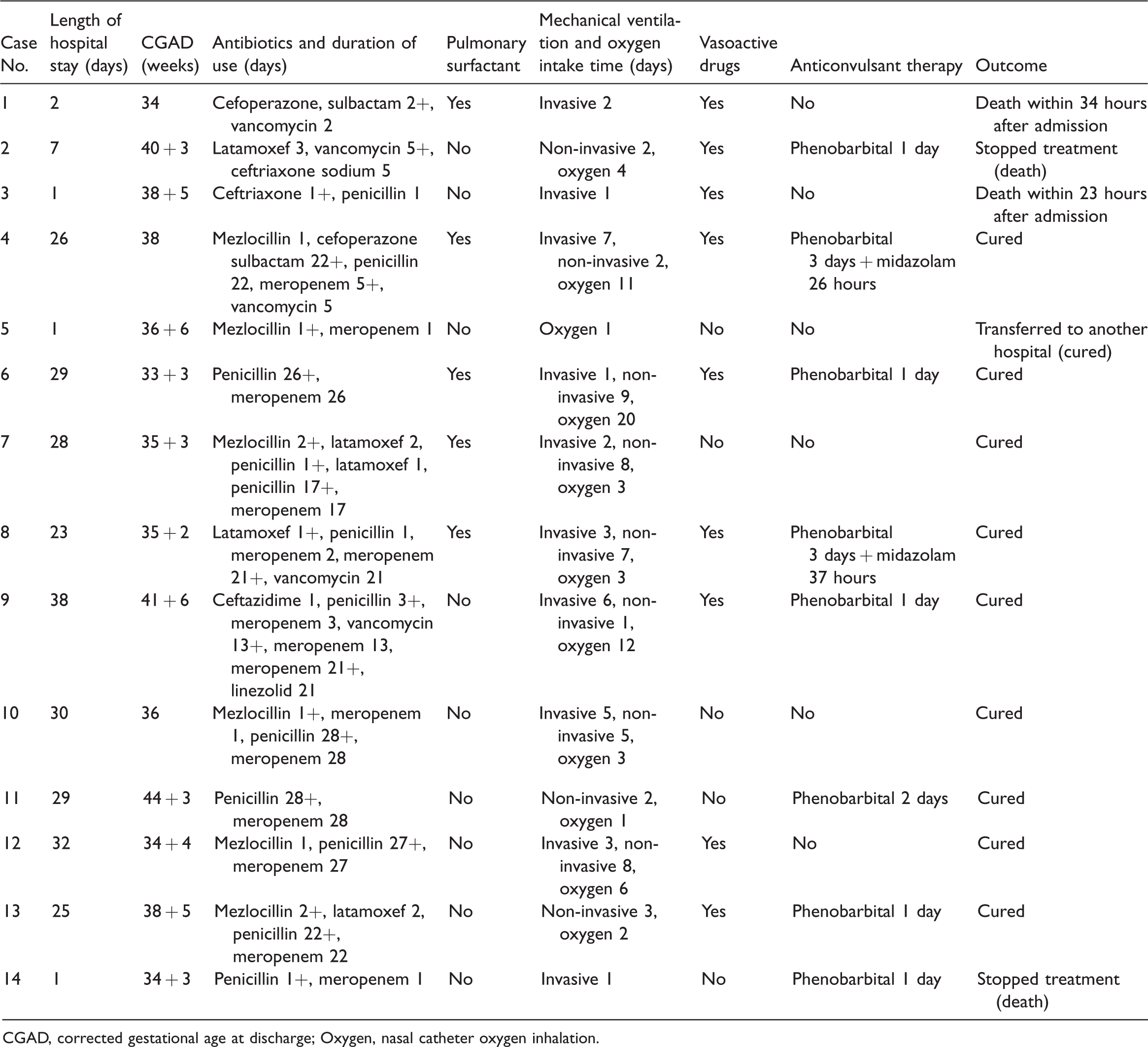
CGAD, corrected gestational age at discharge; Oxygen, nasal catheter oxygen inhalation.
Ten (71%) infants were cured; of whom, nine were treated and discharged from our hospital, and one was transferred to another hospital where they had a full recovery. At follow-up, the surviving infants had good psychomotor development. Among the four patients who died, two patients died in the hospital, and two died after stopping treatment. Case 1 was admitted to the NICU 1 hour after birth with an intrauterine abscess and stench at birth and purulent effusion from the airway, which was managed with tracheal intubation in the delivery room. The patient was treated with cefoperazone sulbactam combined with vancomycin and died of septic shock 35 hours after birth. Cases 2 and 3 were admitted to our hospital at 4 days and 36 hours after birth, respectively. They presented with respiratory and circulatory failure and frequent convulsions on admission and had no response to emergency treatments. Case 14 was admitted to our hospital at 2 hours after birth. She presented a poor response because of severe asphyxia at the time of birth. Although treatment was prompt, frequent convulsions still occurred, and the patient died of coagulation disorder.
Discussion
L. monocytogenes is a gram-positive, rod-shaped bacterium that causes listeriosis. It is usually acquired through the consumption of contaminated food and generally affects those at age extremes, including newborn infants and the elderly, immunocompromised hosts, and pregnant women.1,6,14–18 Listeriosis is 20 times more common in pregnant women than in the non-pregnant population and may result in severe outcomes including miscarriage, preterm delivery, sepsis, and fetal and neonatal infection.8,15–20 The correlation between the incidence of pregnancy-associated listeriosis and dietary habits has been documented. Furthermore, a high prevalence of L. monocytogenes has been reported on farms, and ruminant farms are considered a potential reservoir for this foodborne pathogen.5,21
Infection is commonly observed in the third trimester of pregnancy, and the incidence was reported to be two times higher after 28 weeks of gestation.1,17,18 The incidence during the first month of pregnancy could be underestimated because of undiagnosed spontaneous or premature abortions.15,20 Fetal infection can occur through transplacental dissemination. 5 Less frequently, contamination may occur from the lower genital tract of the mother, and infection may occur in the birth canal during labour.2,20,22 Cross contamination in the same nursery or outbreaks because of contact with contaminated clinical equipment are rare but have been reported. 5
Maternal infection may be asymptomatic or may present as a non-specific, flu-like syndrome.1,5,17,22 Maternal infection precedes delivery by 2 to 14 days and in approximately 70% of cases. Newborns delivered at less than 35 weeks of gestation exhibit a high prevalence of early-onset neonatal listeriosis,5,20,22 which is consistent with our findings. The most common antepartum presentations were fever (93%), meconium staining of the amniotic fluid (86%), and intrauterine fetal distress (79%). Three mothers presented with flu-like symptoms during their pregnancy, and the three women who gave birth in our hospital showed acute chorioamnionitis in placental pathology examinations. This finding emphasizes the importance of placental pathology evaluation in suspected cases.19,23 Clinicians should pay full attention to women with high risk factors such as fever, influenza-like symptoms, a history of intrauterine distress, and amniotic fluid contamination during delivery. Placental tissue and vaginal secretions should be collected in a timely manner during delivery for clinical diagnosis and treatment.
Neonatal listeriosis is described to have two distinct infection forms, early-onset and late-onset infection. 7 The signs of early sepsis are apparent from birth, with a mean symptom onset at 1.5 days of life.4,5,19,24 The onset time was within 3 days after birth for all patients in our study. The most common symptoms included septicemia and respiratory symptoms.6,15,20 The high frequency of respiratory tract involvement may result from inhalation of contaminated amniotic fluid. 4 In our study, most patients developed asphyxia or respiratory distress shortly after birth, requiring endotracheal intubation in the delivery room. These patients also had septic shock, and blood gas analysis suggested various levels of respiratory/metabolic acidosis. The severity of acidosis was correlated with the severity of infection, respiratory distress, and insufficiency of tissue perfusion.
Blood culture confirmed the diagnosis in all cases. Incorrect determination of culture results because of the resemblance of the organism to diphtheroids, cocci, or diplococci and the ability to decolorize during the gram staining procedure contributes to the paucity of confirmed diagnoses of neonatal listeriosis.2,,3,19,25 Therefore, isolation of diphtheroids from the blood or CSF should alert clinicians to the possibility of L. monocytogenes infection. 26 Even in the absence of positive culture results, this infection should be highly suspected in patients presenting signs of early sepsis, respiratory distress, pneumonia, and meconium-stained amniotic fluid at delivery. 10 Serological studies are not helpful in the diagnosis of listeriosis. However, they are important to assess the severity of infection. The hemogram results in our study showed that leukocytosis and thrombocytopenia were common in patients. Neonatal listeriosis mainly occurs in premature infants, who are more susceptible to brain injury because of immature cerebrovascular development, coagulation disturbances, hypoxia, and inflammatory reactions. Therefore, in the diagnosis and treatment of listeriosis, it is important to check for signs and symptoms of central nervous system involvement, such as assessments of the state of consciousness, muscle tension, primitive reflexes, head circumference, and size of the anterior fontanelle. Neuroimaging evaluation, including bedside cranial ultrasound and cranial magnetic resonance imaging, is recommended to monitor the occurrence and evolution of brain damage.
The first-line drugs used for the treatment of listeriosis are penicillin, ampicillin, or amoxicillin, which are often used in combination with an aminoglycoside, classically gentamicin, because of their synergistic bactericidal effects in vitro.1,5,7,9,14,15,20 Although this combination therapy has failed to show any significant advantage in animal models, some studies have reported a decreased risk of death with this combination. In the case of penicillin allergy or unresponsiveness, vancomycin or trimethoprim/sulfamethoxazole can be used as an alternative therapy.18,25 Vancomycin is ineffective for neurolisteriosis because of its inability to cross the blood–brain barrier. 14 In contrast, trimethoprim/sulfamethoxazole has extracellular and intracellular bactericidal activity and penetrates well into the central nervous system. 26 However, it is contraindicated in neonates because of the potential risk of bilirubin displacement and kernicterus. Linezolid is also considered adequate for the treatment of neurolisteriosis because of its elevated CSF and intracellular concentrations. Even though the data are currently limited to support routine administration of this drug for neurolisteriosis, several case reports with favorable outcomes following linezolid therapy have been documented.14,27 Meropenem has a lower minimum inhibitory concentration against L. monocytogenes than that of ampicillin. However, one study reported a higher mortality rate in patients receiving meropenem than in those receiving amino penicillin and benzyl penicillin, but the limited number of neonates and children enrolled in the study does not qualify its conclusion for this age group.9,14 In our study, despite in vitro susceptibility results, Case 9 failed to respond to penicillin/vancomycin combined with meropenem and was successfully treated with linezolid combined with meropenem. The recommended duration of treatment is 2 weeks for bacteremia patients with normal CSF, and for severe cases of infection or meningitis, the treatment period should be no less than 3 weeks because relapses have been documented with shorter durations of therapy.2,19,22,25 The treatment should be extended to at least 6 weeks for patients with brain abscess. 3
In conclusion, neonatal listeriosis is a serious infection associated with a high mortality rate. Early diagnosis and prompt treatment with appropriate antibiotics are essential for a good neonatal outcome. Careful interpretation of culture results and a high index of suspicion are essential for an early and accurate diagnosis. Treatment with a combination of antibiotics improves the bactericidal effect and helps reduce mortality. Finally, educating pregnant women on dietary habits and establishing other preventive strategies are crucial to reduce the frequency of neonatal listeriosis.