
Abstract
Objective
This quasi-randomized controlled trial was performed to evaluate the effects of the PRECEDE-PROCEED model (PPM) in enabling mothers of preterm infants to develop care knowledge, skill, and a sense of competence.
Methods
Among 116 mothers of preterm infants, 60 received traditional discharge education (control group) and 56 received PPM discharge education (PPM group). Improvement in knowledge and skills was transformed into the mothers’ routine daily care of infants. The primary outcome was knowledge of preterm infant care. The secondary outcomes were preterm infant care skills and a sense of competence, routine intervention compliance among mothers, and the readmission rate of infants 6 months after discharge.
Results
Six months after discharge, the mean knowledge score and mean skills score were significantly higher in the PPM group than in the control group. The mothers’ sense of competence with respect to both self-efficacy and satisfaction was also significantly better in the PPM group than in the control group. Moreover, intervention behavior compliance and the readmission rate were significantly better in the PPM group than in the control group.
Conclusion
Care knowledge, skills, and sense of competence in mothers of preterm infants improved after implementation of the PPM.
Introduction
The advanced technology in the neonatal intensive care unit (NICU) has facilitated clinicians’ ability to prolong the life of preterm infants (<37 completed weeks of gestation) and has provided a greater likelihood of surviving to discharge to be cared for by parents, raising questions regarding the adequacy of post-hospital care and readmission. 1,2 Because of the unpredictable physiological changes in premature infants, it is essential for parents to have necessary care knowledge before discharge. 3 Up to 30% of preterm infants are rehospitalized within 6 months after hospital discharge for common problems such as infection, feeding difficulties, weight loss, and gastrointestinal and respiratory conditions because their parents lack required care knowledge, skills, and self-efficacy at home. 4
Studies have shown that caregivers of premature infants who hope to learn infant care skills rely on health care professionals before discharge. 5 Parents’ participation in the care of their infant in a NICU would decrease readmission rates of infants and alleviate the patients’ psychological symptoms, thus contributing to increased care knowledge and satisfaction based on the family integrated care model. 6 However, involving the parents and collaboratively working with health care professionals in the closed and limited space of the NICU is a great challenge in most areas of China. 7 Therefore, it is necessary to establish an effective training model with appropriate interventions and provide tailored education training for mothers of preterm infants, aiming to improve their preterm infant care knowledge and thus meet the care needs of preterm infants.
The PRECEDE-PROCEED model (PPM) was developed by Green and Kreuter, 8 and it guides users to perform assessments in social, epidemiological, behavioral, and environmental areas to plan and evaluate a process using a systematic approach. 9 More recent adaptations of the model in relation to maternal and child health have included studies and projects on chronic diseases. 10 With application of the PPM to primiparas, participants were motivated to implement a more effective breastfeeding practice. 11 In the present study, we used the PPM to construct and implement health education training among mothers of preterm infants in the NICU of Baoji Maternal and Child Health Hospital. Our aim was to enable mothers to increase their infant care knowledge, skills, and sense of competence in their abilities after hospital discharge.
Methods
Setting and participants
This study was conducted in a 60-bed NICU of a tertiary maternal and child health hospital located in the northwest region of China from June 2019 to July 2020. Approximately 1000 preterm infants are admitted to the NICU each year. The infants receive intensive treatment and care in the NICU by professions until they are discharged from the hospital. No visiting policies are in place; parents are not allowed to visit their infants at the bedside but only in the parents’ reception room of the NICU, where they can also communicate with physicians and nurses.
The reporting of this study conforms to the CONSORT statements. 12 The inclusion criteria were preterm infants with a gestational age of 28 to 36+6 weeks, weight of >1500 g, 5-minute Apgar score of ≥8 points after birth, and birth in the hospital in which the study took place. Additionally, the mothers were required to be the primary caregiver after the infants’ discharge and express willingness to participate in the study. For the infants, the exclusion were the performance of surgery and ventilator treatment in the neonatal period as well as the presence of any congenital malformations and genetic diseases; for the mothers, the exclusion criteria were psychiatric problems, infectious diseases, disabilities, and education not extending beyond high school. All infants’ mothers were verbally informed about the purpose of the study and provided their written consent. The study was approved by the Ethics Committee of Baoji Maternal and Child Health Hospital (IRB No. BFYL-2017-6). In total, 120 infants and their mothers were initially enrolled in the study. The sample size was calculated using a mean difference of α = 0.05, β = 0.1, and σ = 1.43, and in accordance with a similar clinical study, 6 we determined that 60 patients per group were required to yield statistically significant results. The mothers were assigned to either the PPM group or control group (60 in each group) 13 according to the last digit of the infants’ sequential hospitalization number (single or double entry number).
Design
This quasi-randomized controlled trial was based on the PPM. Phases 1 to 5 were related to the PRECEDE stage, and phases 6 to 9 were related to the PROCEED stage (Figure 1). In the first three phases, we reviewed the literature and assessed the coping ability of mothers of premature infants upon discharge, identified the type of education models used to improve preterm infants’ care practice, identified the factors influencing the education process, and assessed the gaps in the mothers’ care ability. In phase 4, we categorized the identified factors into predisposing factors, enabling factors, and reinforcing factors. Predisposing factors provide mothers with motivation in their current skill, knowledge, and sense of competence in infant care. Enabling factors include setting up a health education room, improving the education care process, providing training resources, and providing simulation teaching equipment (e.g., incubators, disinfection and emergency rescue equipment, a crib, an adult bed, a bathing area, breastfeeding and other simulation teaching aids, and physical and nerve measurement tools to enable educators to provide demonstrations). Reinforcing factors promote intervention behavior compliance, prompting preterm infants’ mothers to realize that a change is needed in their care skills or providing professional activities that encourage and motivate them to make an improvement. In phase 5, we carefully examined the information from previous phases, identified the mothers’ background competence in infant care, and analyzed the competence gaps in the care content and process of caring.

Flow diagram of study participants.
Traditional post-discharge care and PPM intervention
After the PROCEED stage, our health education started with video training that was repeated from Monday to Friday in the parents’ reception setting of the NICU. The video content was related to knowledge regarding the catch-up growth of preterm infants and routine care skills. Mothers in the control group received traditional post-discharge care. In the PPM group, the mothers were provided theory and practice support by health professionals at monthly hospital visits and were informed of the next follow-up time. The infant care information included verbal instruction, demonstration, and brochures regarding infant care before discharge; the mothers were also advised to autonomously learn as much care-related information as possible from the WeChat platform of the hospital. The infants’ growth information records were collected. However, mothers in the control group did not receive theory and practice support or continuous care nursing.
The mothers’ care knowledge in the PPM group consisted of three training sessions lasting an average of about 1.5 to 2.0 hours and continuous care nursing after infant discharge. The first session occurred on the second day of the infants’ admission to the NICU. The session focused on predisposing factors by the teaching of theory, and the mothers were given educational materials (booklets and videos) that included the training content. The second session involved practice training on the day of the mothers’ discharge. Professional caring skills and daily care methods were delivered by trained nurses. The third session was implemented 1 day before the infants’ discharge. The content aimed to strengthen mother–infant attachment and to help mothers reflect on their parenting role and respond their preterm infant’s behaviors. In-depth communication was also conducted to understand the mothers’ needs and their perceived barriers to establishing a trust relationship with the medical staff (Table 1). For continuous care nursing after infants’ discharge, a supervision system was set up through WeChat or telephone for continuous intervention monitoring. Text messages and video teachings were regularly sent to the WeChat platform during the 6-month intervention period to further enhance the mothers’ confidence and skills in adopting and maintaining healthy care behaviors at home after discharge. Peer (mother-to-mother) WeChat communication was established to provide adequate emotional and information support, allowing mothers to share their caring experiences with one another.
PRECEDE-PROCEED model intervention plan for predisposing factors among mothers of preterm infants.

CPR, cardiopulmonary resuscitation; NICU, neonatal intensive care unit.
Assessment measures
This study primarily assessed the effect of the PPM intervention on mothers’ care knowledge of preterm infants. The assessment tool was developed from literature titled Essential guide for parenting premature infants
14
and Family readiness for preterm infant discharge.
15
Validity was tested by three experienced health care professionals who assessed the questionnaire content. The instrument contained the following four subscales.
Demographic information of the infants (sex, gestational age, birth weight, delivery route, Apgar score, and length of stay in the hospital) and their mothers (age, education level, and place of residence) was collected. Care knowledge and skills were assessed before the intervention and at 1 and 6 months after discharge using a self-made questionnaire titled “Care ability of mothers for preterm infants.”
16,
17 Knowledge of preterm infant care (e.g., knowledge of the infant’s digestion and appropriate volume of milk) was assessed using 14 items, the responses to which were scored on a 5-point Likert scale ranging from poor (1 point) to very good (5 points). The highest possible score was 70 points, and higher scores indicated better infant care knowledge. Skills of preterm infant care (e.g., oxygen use) were assessed using 11 items, the responses to which were scored on a 3-point Likert scale ranging from poor (1 point) to very good (3 points). The highest possible score was 33 points. Cronbach’s alpha was 0.916, and the content validity of the questionnaire was 0.946. The mothers’ sense of competence was measured before the intervention and at 1 and 6 months after discharge using the Chinese version of the parenting sense of competence scale.
18
This scale consists of 16 items in 2 subscales (efficacy dimension and satisfaction dimension). Responses were scored on a 6-point Likert scale ranging from strongly disagree (1 point) to strongly agree (6 points). The total score ranged from 8 to 48 points for the efficacy dimension with 8 items forward-coded and from 9 to 54 points for the satisfaction dimension with 9 items reverse-coded. Higher scores indicated a greater sense of competence. Cronbach’s alpha was 0.823, and the content validity of the questionnaire was 0.881. Early intervention behavior and the readmission rate were measured at 6 months after discharge. Early intervention behavior into routine daily life was assessed using the items breastfeeding, skin-to-skin contact, weekly recording of growth, and listening to music for ≥30 minutes. The mothers’ responses were scored on a 5-point Likert scale ranging from never (1 point) to always (5 points), and higher scores indicated greater intervention behavior compliance.
Data collection
Trained investigators explained the purpose and significance of the study to each participant, and the questionnaires were administered and completed on site after obtaining consent from the participants. First, for evaluation of the demographic characteristics and baseline data, 120 questionnaires on demographics and baseline evaluation content regarding care competence among mothers of preterm infants were distributed and then collected on the second day of the infants’ admission. Second, for the survey of the intervention effect after 1 month, questionnaires were completed on site at the 30- to 40-day return to the hospital after discharge; the response rate was 96.67% (116/120). Finally, for the survey of the intervention effect at the end of 6 months, 120 questionnaires were administered at the 180- to 190-day return to the hospital after discharge; the response rate was 96.67% (116/120).
Data analysis
The distributions of the baseline demographic characteristics of the PPM group and control group are summarized using descriptive statistics. Data from eligible questionnaires in the PPM group and control group were entered into EpiData 3.0. Statistical analyses were conducted using SPSS Statistics for Windows, Version 17.0 (Chinese Version) (SPSS Inc., Chicago, IL, USA). Data regarding knowledge, skills of preterm infant care, and mothers’ sense of competence are presented using mean ± standard deviation. Differences in scores between the PPM group and control group were examined using the independent-sample (two-sample) t-test, and differences between the pre-intervention period and 1 and 6 months after discharge were compared by one-way analysis of variance. Data regarding early intervention behaviors (breastfeeding, skin-to-skin contact, weekly recording of growth, and listening to music for ≥30 minutes) are presented as mean (P25, P75), the differences in the scores between the PPM and control groups were evaluated by the independent-samples nonparametric Mann–Whitney test, and the 6-month readmission rate is presented as a percentage. Probability values of <0.05 were considered statistically significant.
Results
Demographic characteristics at baseline
A total of 120 mothers met the inclusion criteria and consented to participate. During the follow-up period, four mothers in the PPM group dropped out because of an inability to complete all the infant development cards and intervention items. Thus, the PPM group comprised 56 participants and the control group comprised 60 participants (Figure 2). There were no significant differences in the demographic characteristics of the participants between the two groups (Table 2).

Application of PRECEDE-PROCEED model among mothers of preterm infants.
Baseline data: demographic characteristics of preterm infants and mothers.

Data are presented as n (%) or mean ± standard deviation.
PPM, PRECEDE-PROCEED model.
Baseline evaluation of knowledge, sense of competence, and skills of preterm infant care
The mean scores for knowledge, a sense of competence, and skills of preterm infant care before the intervention were similar between the two groups (Table 3). Table 4 shows the three lowest numbers of positive responses regarding preterm infant care knowledge, a sense of competence, and skills. The baseline results showed that 22.50% of mothers had adequate knowledge of infant behavior and abnormalities, such as spitting up, a choking cough, and cardiopulmonary resuscitation, and that 34.16% of mothers had adequate knowledge regarding growth and development, including requiring a long time to settle into a routine and fluctuating attention. Only 10.83% of mothers showed that they could cope with an emergency condition in the event of a fever or the requirement for oxygen. Only 25.00% thought that being a mother is manageable and that any problems can be easily resolved, whereas 74.17% felt tense and anxious and were worried that their preterm infants would not grow up in a healthy way like other term infants.
Comparison of mothers’ knowledge, sense of competence, and skills scores between pre- and post-intervention periods in the two groups.

Data are presented as mean ± standard deviation. The units of measurement are points (i.e., scores).
PPM, PRECEDE-PROCEED model.
*P < 0.05, PPM group vs. control group; △P < 0.001, 1 month after discharge vs. before intervention; #P < 0.001, 6 months after discharge vs. 1 month after discharge.
Baseline survey: items with lowest number of positive responses among mothers of preterm infants (n = 120).

Data are presented as n (%).
CPR, cardiopulmonary resuscitation.
Post-intervention knowledge, sense of competence, and skill scores for preterm infant care
The primary outcome of care knowledge was significantly higher in the PPM group than in the control group at both 1 and 6 months (37.07 vs. 33.25 and 56.70 vs. 43.28, respectively; P < 0.05). The mean scores for care skills, satisfaction, and efficacy were significantly higher in the PPM group than in the control group (P < 0.05) (Table 3).
Intervention behavior compliance among mothers of preterm infants and readmission rate within 6 months after discharge
Early intervention behavior compliance including skin-to-skin contact, breastfeeding, weekly recording of growth and development, and regular clinic follow-up was higher in the PPM group than in the control group (P < 0.05); however, no significant difference was observed in listening to music for ≥30 minutes. The readmission rate within 6 months after discharge was significantly lower in the PPM group than in the control group (P = 0.03) (Table 5).
Intervention behavior compliance among mothers of preterm infants and readmission rate within 6 months after discharge.
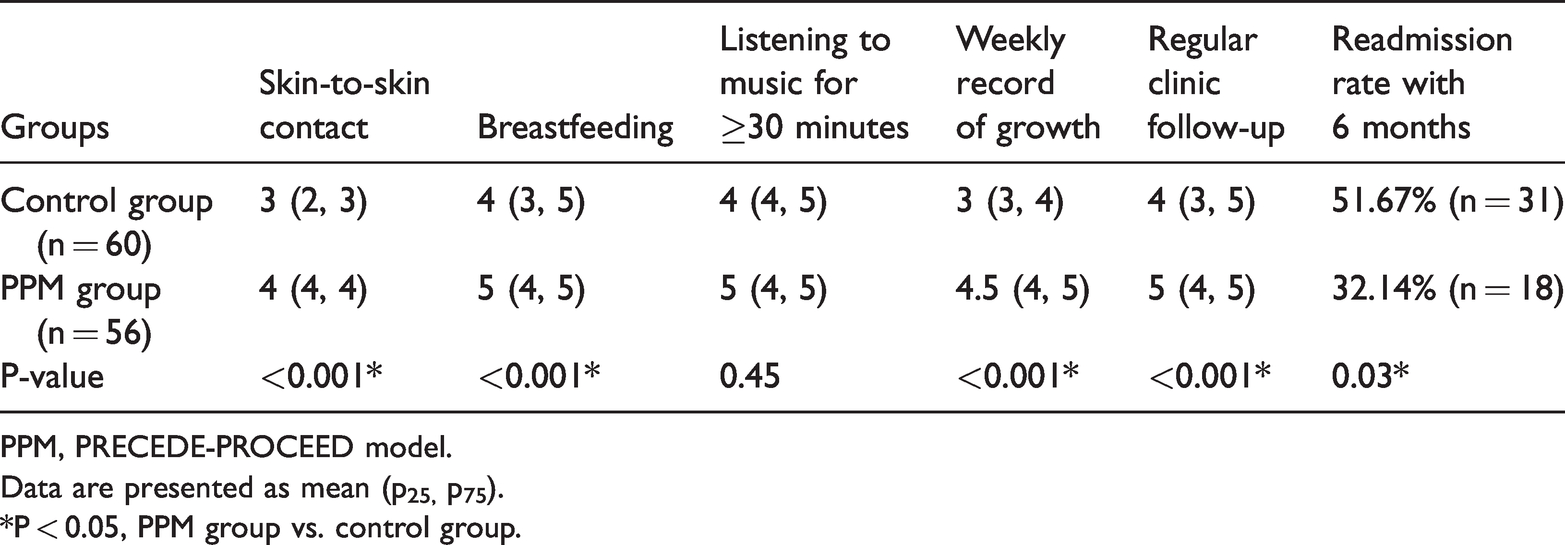
PPM, PRECEDE-PROCEED model.
Data are presented as mean (p25, p75).
*P < 0.05, PPM group vs. control group.
Discussion
The main result of this study is that implementation of the PPM was effective in improving mothers’ care knowledge of preterm infants. The 6-month PPM intervention resulted in a significantly greater improvement in knowledge among mothers in the PPM group than among those in the control group. In the PRECEDE phases, we found that the items regarding knowledge of preterm infant care (e.g., knowledge of early intervention and correct gestational age, recognition of infants’ behaviors and abnormalities) had the lowest frequency of correct responses in both groups. A similar study by Lijun and Shuju 19 showed that caregivers of preterm mothers had a low level of knowledge. It is necessary for nurses to be experts in guiding and supporting parents to effectively participate in their infants’ daily care. 20 In another study, health education was tailored to mothers based on the PPM by clarifying existing misconceptions about occupational blood-borne infectious exposure and preventive regimens and by increasing relevant knowledge using lectures, booklets, and reminder text messages. 21 In this respect, mothers in the intervention group received a tailor-made education course, and extended nursing increased the mothers’ knowledge in caring for their preterm infants 6 months after discharge from the hospital.
The participants’ mean skills score improved to a greater degree in the PPM group than in the control group at 1 and 6 months after discharge. The mothers in both groups were encouraged to practice their care skills as much as they needed before discharge. A policy exists in the NICU to prevent mothers from being involved in infant care. 17 A previous study based on the PPM indicated that individual factors and environmental constraints play a major role in practicing the techniques of care. 22 In the PRECEDE phases of this study, the participants in the intervention group attended practice training involving the use of simulation teaching equipment, and trained nurses provided purposeful actual practice interaction with the participants in the education room of the NICU. However, mastering skills requires frequent practice. 23 Therefore, reinforcing factors guided researchers in conducting follow-up monitoring by regular reminder messages and videos to help mothers apply routine practice, early intervention behavior (i.e., skin-to-skin care and massage), and care skills such as breastfeeding and bottle-feeding, bathing, excretion, body temperature, hand-washing, room disinfection, measurement of growth and development, and correct handling of fever, chest care, cardiopulmonary resuscitation, and vaccination.
A sense of competence is defined as having the knowledge and skill abilities to manage demands with high self-efficacy and having satisfaction in the parental role. 24 A low level of parenting competence may increase parental depression and other negative emotions. 25 Our study revealed that mothers’ sense of competence improved to a significantly greater degree in terms of self-efficacy and satisfaction in the PPM group than in the control group at 6 month after discharge. This might be attributable to health professionals providing continuous care guidance, supporting mothers in developing their self-efficacy, and giving mothers a feeling of security; mothers’ interactions with their peers was also a valuable source of emotional support for one another after infant discharge. 26 A high level of care skills has a positive effect on mothers’ sense of competence in parenting, which in turn inspires learning skills. 26
Preterm infants should be closely monitored and regularly receive health services after discharge to detect deviations in their growth development and to guide caregivers in feeding and preventive measures. 27 One study indicated that providing a strong basis for interventions has the potential to support parents in their parenting role and guide them in engaging in developmentally appropriate interactions with their preterm infants. 28 The present study revealed that mothers who received the PPM intervention had significantly higher routine early intervention behavior compliance and a significantly lower readmission rate than those in the control group. This was because application of the PRECEDE assessment phase and the PROCEED planning and implementation phases translated knowledge, competence, and skills more effectively and thus facilitated mothers’ participation in infant care and earlier intervention compliance.
Limitations
This study had several limitations. First, we did not measure the effect of the preterm infants’ clinical outcomes (such as weight and motor growth) as a result of improvements in knowledge, skills, and sense of competence. Second, very-low-weight preterm infants and mothers with less than a high school education were excluded from this study; therefore, the results cannot be generalized to broader populations. Third, the intervention and continuous supervision were conducted for only 6 months, but catch-up growth of preterm infants requires at least 1 year of intervention compliance; therefore, the findings cannot be directly applied to longer intervals.
Application to practice
This health education based on the PPM provides evidence that knowledge, skill, and a sense of competence in changing strategies can be used to improve quality of life and expand family care.
Conclusions
This study showed how the PPM is beneficial for increasing knowledge, enhancing care skills, and improving the sense of competence among mother of preterm infants. The PPM intervention enhanced mothers’ participation in intervention behavior compliance and reduced the readmission rate.
Supplemental Material
sj-pdf-1-imr-10.1177_03000605221110699 - Supplemental material for Effectiveness of the PRECEDE-PROCEED model for improving the care knowledge, skill, and sense of competence in mothers of preterm infants
Supplemental material, sj-pdf-1-imr-10.1177_03000605221110699 for Effectiveness of the PRECEDE-PROCEED model for improving the care knowledge, skill, and sense of competence in mothers of preterm infants by Shaoli Li, Shufang Liu, Xinchun Zhang, Yali Chen and Xiaohong Ren in Journal of International Medical Research
Footnotes
Acknowledgements
The authors would like to thank all the health professionals in the NICU as well as one nutritionist and pharmacist in our hospital. The authors would also like to thank all the mothers of preterm infants who participated in this study for their invaluable cooperation.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.