
Abstract
Objective
To identify factors associated with high-flow nasal cannula (HFNC) therapy failure in patients with severe COVID-19.
Methods
We retrospectively examined clinical and laboratory data upon admission, treatments, and outcomes of patients with severe COVID-19. Sequential Organ Failure Assessment (SOFA) scores were also calculated.
Results
Of 54 patients with severe COVID-19, HFNC therapy was successful in 28 (51.9%) and unsuccessful in 26 (48.1%). HFNC therapy failure was more common in patients aged ≥60 years and in men. Compared with patients with successful HFNC therapy, patients with HFNC therapy failure had higher percentages of fatigue, anorexia, and cardiovascular disease; a longer time from symptom onset to diagnosis; higher SOFA scores; a higher body temperature, respiratory rate, and heart rate; more complications, including acute respiratory distress syndrome, septic shock, myocardial damage, and acute kidney injury; a higher C-reactive protein concentration, neutrophil count, and prothrombin time; and a lower arterial partial pressure of oxygen/fraction of inspired oxygen (PaO2/FiO2). However, male sex, a low PaO2/FiO2, and a high SOFA score were the only independent factors significantly associated with HFNC therapy failure.
Conclusions
Male sex, a low PaO2/FiO2, and a high SOFA score were independently associated with HFNC therapy failure in patients with severe COVID-19.
Keywords
Introduction
Coronavirus disease 2019 (COVID-19) is an acute respiratory infectious disease caused by a novel coronavirus, severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2, previously known as 2019-nCoV).1 –3 Patients with severe COVID-19 can develop dyspnea and hypoxemia within 1 week after symptom onset, and their condition can quickly progress to acute respiratory distress syndrome (ARDS) and end-organ failure. 4 In three pooled studies involving 278 patients with COVID-19, 56 (20.1%) patients developed ARDS.4 –6 Considering that acute hypoxemic respiratory failure is prevalent in patients with severe COVID-19, large-scale, safe delivery of respiratory support is needed to resolve this key healthcare challenge of the COVID-19 pandemic. 7
High-flow nasal cannula (HFNC) oxygen therapy is a noninvasive therapy in which heated, humidified oxygen is delivered via a large-bore nasal cannula at flow rates up to 60 L/min. 8 HFNC therapy may be considered a first-line therapy in patients with acute respiratory failure, including patients with ARDS. 9 The major goal of HFNC therapy in treating ARDS is to achieve sufficient oxygenation to avoid endotracheal intubation. Compared with standard oxygen therapy, HFNC therapy can improve oxygenation, decrease the respiratory rate, increase the lung volume, and improve patient comfort 8 ; HFNC therapy may also be better tolerated than noninvasive ventilation. Therefore, HFNC therapy may be an appropriate therapy for many patients with COVID-19 for whom tracheal intubation has not yet become a necessity but for whom low-flow nasal oxygen or facemask oxygen is not providing adequate respiratory support. 7 HFNC therapy is currently one of the most common ventilation strategies for patients with COVID-19 who have developed respiratory failure.10 –18 To avoid HFNC therapy failure and intubation delay, it is essential to select appropriate patients with COVID-19 for this therapy. However, little attention has been given to evaluating the factors associated with HFNC therapy failure. This retrospective observational case series study was performed to identify the factors associated with HFNC therapy failure in patients with severe COVID-19 who have developed hypoxic respiratory failure.
Materials and methods
Participants
This retrospective, single-center, observational case series included patients with COVID-19 who were admitted to the Infectious Disease Department of the Renmin Hospital of Wuhan University (Wuhan, China) from 1 February 2020 to 26 March 2020. The selected patients met the following inclusion criteria: age of ≥18 years, diagnosis of severe COVID-19, and treatment with HFNC therapy for hypoxic respiratory failure. Severe COVID-19 was defined according to the Chinese management guidelines for COVID-19 (version 6.0). 19 SARS-CoV-2 infection was confirmed by real-time reverse-transcription polymerase chain reaction assay. 20 The present study was conducted in accordance with the Declaration of Helsinki (2013 edition) adopted by the World Medical Association. 21 The reporting of this study conforms to the STROBE guidelines. 22 The retrospective analysis of data was approved by the ethics committee of the First Affiliated Hospital of Dalian Medical University (PJ-KS-KY-2020-88). Because this was a retrospective study, the need for informed consent from the study participants was waived.
HFNC
HFNC therapy (Fisher & Paykel Healthcare Ltd., Auckland, New Zealand) was used to treat patients with severe COVID-19 with the aim of reaching and maintaining a target pulse oximetry blood oxygen saturation (SpO2) of >90% only when dyspnea (respiratory rate of ≥30 breaths/minute) and/or hypoxemia (SpO2 of <90%) were not improved after treatment with standard oxygen therapy (oxygen inhalation by nasal tube or facemask). 19 The temperature was set at 31°C to 37°C, the flow rate was set at 30 to 60 L/minute, and the fraction of inspired oxygen concentration (FiO2) was set to maintain an SpO2 of >93%. HFNC therapy was used continuously for all enrolled patients in the initial phase of treatment. When respiratory failure was reversed, HFNC therapy was used intermittently. The duration of standard oxygen therapy was gradually increased, and the duration of HFNC therapy was gradually decreased until the patient was weaned from HFNC therapy. However, if dyspnea (respiratory rate of ≥30 breaths/minute) and/or hypoxemia (SpO2 of <90%) were not improved within 1 to 2 hours after HFNC therapy, the attending physicians determined whether to use either noninvasive ventilation or invasive mechanical ventilation as rescue therapy. Early endotracheal intubation and invasive mechanical ventilation were immediately considered in patients who failed to maintain an arterial partial pressure of oxygen (PaO2)/FiO2 of >150 within 1 to 2 hours after HFNC therapy. 19 Patients who were changed from HFNC therapy to conventional oxygen therapy were defined as having undergone successful HFNC therapy (Success group), and patients who required noninvasive ventilation or intubation as rescue therapy or who died were defined as having undergone failed HFNC therapy (Failure group).
Data collection
Epidemiological data, demographics, medical history, contact history, signs and symptoms, comorbidities, and laboratory results were collected from the patients’ clinical records. Disease severity was assessed with the Sequential Organ Failure Assessment (SOFA) score. We also recorded outcomes within 28 days of HFNC therapy.
Statistical analyses
Data were analyzed with IBM SPSS Statistics for Windows, Version 22.0 (IBM Corp., Armonk, NY, USA). Continuous variables are presented as median (range), and categorical variables are presented as frequency (%). Categorical data were compared using the chi square test or Fisher’s exact test, and continuous variables were compared by the Mann–Whitney U test. We performed a binary logistical regression analysis with stepwise backward elimination to determine the factors associated with HFNC therapy failure, and the odds ratios (ORs) and 95% confidence intervals (CIs) were calculated. Considering the small sample size of our study (n = 54) and to avoid overfitting in the model, we chose five independent variables with a P value of <0.10 in the univariable analyses for inclusion in the binary logistic regression analysis according to previous findings. We used HFNC therapy failure (yes/no) as the dependent variable and age, sex, time from symptom onset to diagnosis, PaO2/FiO2, and SOFA score as independent variables. All tests were two-sided, and a P value of <0.05 was considered statistically significant.
Results
We enrolled 54 patients with severe COVID-19 who underwent HFNC therapy (Figure 1). Of these 54 patients, 28 (51.9%) were successfully treated by HFNC therapy (Success group) and 26 (48.1%) experienced HFNC therapy failure (Failure group). Among the 26 patients in the Failure group, 9 received noninvasive ventilation as rescue therapy and 15 cases received endotracheal intubation and invasive mechanical ventilation as rescue therapy. In addition, among the nine patients who received noninvasive ventilation, six received endotracheal intubation and invasive mechanical ventilation as rescue therapy. Among 10 patients who died in the Failure group, 2 with a long history of coronary heart disease died during HFNC therapy because of sudden cardiac arrest induced by the initial rhythm of the ventricular fibrillation, 6 died during invasive mechanical ventilation therapy because of severe ARDS, and 2 died during noninvasive ventilation therapy because a relative did not consent to early intubation and invasive mechanical ventilation.

Flowchart of participant enrollment.
The clinical characteristics of all patients with severe COVID-19 who underwent HFNC therapy in the Success and Failure groups are summarized in Table 1. Patients in the Failure group were older than those in the Success group, but the difference was not statistically significant. However, the percentage of patients older than 60 years was higher in the Failure group than in the Success group (69.2% vs. 30.8%, respectively; P = 0.001). The proportion of male patients was higher in the Failure group than in the Success group (61.5% vs. 38.5%, respectively; P < 0.001). Notably, patients in the Failure group had a significantly higher percentage of fatigue, anorexia, and comorbid cardiovascular disease than patients in the Success group. In addition, the time from symptom onset to diagnosis was longer in the Failure group than in the Success group, indicating delayed hospitalization and treatment in the Failure group. The body temperature, respiratory rate, and heart rate were also significantly higher in the Failure group than in the Success group. Furthermore, patients in the Failure group had significantly higher SOFA scores, with a significantly higher percentage of ARDS, septic shock, and acute myocardial and kidney injury than patients in the Success group, indicating greater disease severity in patients in the Failure group. Patients in the Failure group had a significantly higher neutrophil count, prothrombin time, creatinine level, and C-reactive protein level and a significantly lower PaO2/FiO2 than those in the Success group (all P < 0.05).
Characteristics of patients with severe COVID-19 treated with HFNC therapy.

Data are presented as median (range) or n (%). P* indicates the P-values for comparisons of the Success group and Failure group.
χ2/F, chi-square/Fisher’s exact test; HFNC, high-flow nasal cannula; COPD, chronic obstructive pulmonary disease; COVID-19, coronavirus disease 2019; SOFA, Sequential Organ Failure Assessment; MAP, mean arterial pressure; ARDS, acute respiratory distress syndrome; AKI, acute kidney injury; PCT, procalcitonin; PaO2/FiO2, arterial partial pressure of oxygen/fraction of inspired oxygen; PaCO2, arterial partial pressure of carbon dioxide; BUN, blood urea nitrogen; APTT, activated partial thromboplastin time; ALT, alanine aminotransferase; AST, aspartate aminotransferase.
The binary logistic regression analysis showed that male sex, a low PaO2/FiO2, and a high SOFA score were the only independent factors significantly associated with HFNC therapy failure in patients with severe COVID-19 (Table 2).
Risk factors associated with HFNC therapy failure in patients with severe COVID-19.
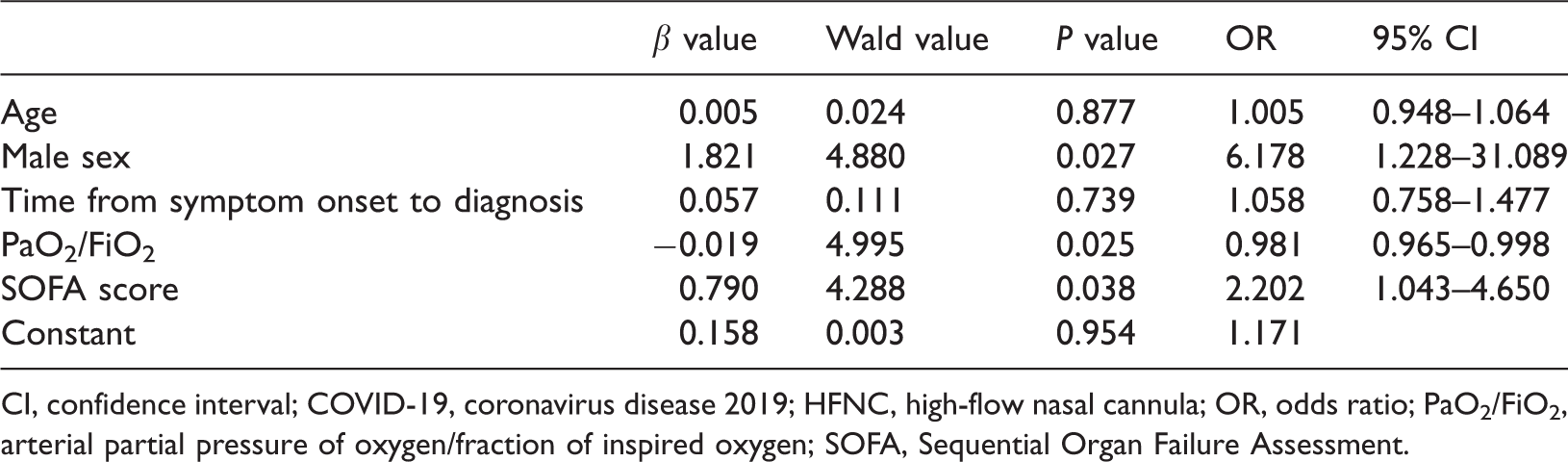
CI, confidence interval; COVID-19, coronavirus disease 2019; HFNC, high-flow nasal cannula; OR, odds ratio; PaO2/FiO2, arterial partial pressure of oxygen/fraction of inspired oxygen; SOFA, Sequential Organ Failure Assessment.
Discussion
In the present study, we retrospectively investigated the clinical characteristics of patients with severe COVID-19 who underwent failed HFNC therapy and the factors associated with HFNC therapy failure. We observed a high failure rate of HFNC therapy among the patients in this study, similar to the results reported by Wang et al. 10 We found that HFNC therapy failure was associated with male sex, a low PaO2/FiO2, and a high SOFA score in patients with severe COVID-19.
Increasing amounts of data are showing hat COVID-19 severity is related to sex.23 –25 A retrospective cohort study in China showed that male sex is a major risk factor for higher disease severity and mortality. 26 A web-based COVID-19 survey in Italy that included 6873 participants (mean age, 47.9 ± 14.1 years; 65.8% women) showed that women had lower odds than men of a positive nasopharyngeal swab test (adjusted OR, 0.75; 95% CI, 0.66–0.85) and of having a severe infection (adjusted OR, 0.46; 95% CI, 0.37–0.57). 27 This sex-related discrepancy of disease severity and high mortality in patients with COVID-19 may be due to hormonal differences, socioeconomic factors, genetic susceptibility, sex-related comorbidities, and habits such as smoking and alcohol consumption.28,29 In addition, recent structural and functional analyses of female sex hormones and their relation to SARS-CoV-2 cell entry revealed a putative mechanism whereby female sex hormones may protect against the development of a severe infection in patients with COVID-19. 30 In the present study, we found that male patients with COVID-19 had a higher OR for HFNC therapy failure, which was consistent with the tendency toward more severe disease and higher mortality in male patients with COVID-19.5,6,31 –33 This higher possibility of HFNC therapy failure may be because male patients tend to have greater disease severity and poorer tolerance to HFNC therapy, especially older male patients. Thus, early monitoring with high-quality supportive care is needed for these patients, and HFNC therapy should be implemented as early as possible to avoid treatment delay for older male patients with COVID-19 who are at high risk.
We also found that a low PaO2/FiO2 and a high SOFA score were independent factors significantly associated with HFNC therapy failure. Our observations showed that a low PaO2/FiO2, as one of six variables, constituted a large proportion of patients when assessing the SOFA scores because other variables (namely the platelet count, bilirubin level, mean arterial blood pressure, Glasgow coma score, and creatinine level) were not as strongly affected in patients with severe COVID-19. Increasing evidence also shows that patients with severe COVID-19 are characterized by classic ARDS, as indicated by the signs of dyspnea and a decreased PaO2/FiO2.5,6,31 –35 Indeed, from a therapeutic perspective, positive end-expiratory pressure ventilation is optimally used to increase functional residual capacity and open collapsed alveoli, thereby improving ventilation–perfusion match, reducing intrapulmonary shunting, and improving lung compliance; overall, these changes reduce the respiratory load. In addition, positive end-expiratory pressure assists respiratory muscles during inspiration, reducing respiratory effort and dyspnea. From a theoretical and physiological point of view, HFNC therapy may also be beneficial in patients with ARDS. However, HFNC therapy is only a “partial support” therapy. This is mainly because HFNC therapy generates only a small positive-pressure spike at end-expiration that depends on the nasal airflow and the extent of mouth opening. HFNC therapy appears to improve oxygenation primarily by flushing the nasal airspaces, which reduces anatomical dead space. As such, HFNC therapy does not sufficiently address the underlying pathology of ARDS, such as the ventilation–perfusion mismatch caused by atelectasis or consolidation in the dependent areas. 36 Therefore, HFNC therapy is more likely to be unsuccessful when used in patients with COVID-19 who have a low PaO2/FiO2. A recent study showed that HFNC therapy alone could be offered to patients with mild disease (PaO2/FiO2 of 200–300 mmHg). 35 Therefore, patients with COVID-19 who develop severe ARDS are not appropriate candidates for HFNC therapy,17,37,38 and invasive mechanical ventilation is the optimal choice. This is because invasive mechanical ventilation may result in better physiological effects on ventilation–perfusion mismatch and greater homogeneity in ARDS mechanics during positive-pressure support.31,39
The present study had two limitations. First, this was a retrospective study, which may limit the strength and reliability of our results. Second, this was a single-center study with a relatively small sample size. The small sample size may have led to bias, yielding spurious findings in the statistical analysis and thus limiting the reliability of the results. Increasing the sample size by enrolling more patients in future studies would help to avoid this limitation.
Conclusions
In patients with severe COVID-19, male sex, a low PaO2/FiO2, and a high SOFA score were independent factors associated with HFNC therapy failure. However, studies with larger sample sizes or multicenter studies are warranted.
Supplemental Material
sj-pdf-1-imr-10.1177_03000605221103525 - Supplemental material for Factors associated with failure of high-flow nasal cannula oxygen therapy in patients with severe COVID-19: a retrospective case series
Supplemental material, sj-pdf-1-imr-10.1177_03000605221103525 for Factors associated with failure of high-flow nasal cannula oxygen therapy in patients with severe COVID-19: a retrospective case series by Xiao-Huan Ma, Meng-Meng An, Fang Yin, Jie Zhang, Meng-Yun Peng, Hong Guan and Ping Gong in Journal of International Medical Research
Footnotes
Acknowledgements
We thank the staff of the Infectious Disease Department of Renmin Hospital of Wuhan University for their efforts in collecting the information that was used in this study and in caring for the patients. We thank Jane Charbonneau, DVM, from Liwen Bianji, Edanz Group China (![]() ), for editing the English text of a draft of this manuscript.
), for editing the English text of a draft of this manuscript.
Author contributions
PG and HG conceived and designed the study. XHM, MMA, FY, and JZ participated in the patient management and data collection. XHM, MMA, and MYP analyzed the data. XHM and MMA wrote the manuscript. PG and HG took overall responsibility for the manuscript. All authors approved the final version of the manuscript.
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the National Natural Science Foundation of China (81571869).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.