
Abstract
Objective
To compare the results and 5- and 8-year overall survival (OS) and disease-free survival (DFS) of hand-assisted laparoscopic surgery (HALS) and laparoscopic-assisted surgery (LAS) in radical gastrectomy for advanced distal gastric cancer.
Methods
A total of 124 patients admitted to our institution from May 2009 to April 2013 were randomly divided into a HALS group (n = 62) and a LAS group (n = 62). Postoperatively, 110 patients were followed for 5 and 8 years, and 14 patients were lost to follow-up. The 5- and 8-year OS and DFS rates of the groups were compared and analyzed.
Results
The 5- and 8-year OS rates, respectively, were 38.8% and 19.4% in the HALS group and 38.3% and 15.3% in the LAS group (log-rank test, χ2 = 0.250). The 5- and 8-year DFS rates, respectively, were 23.1% and 10.6% in the HALS group and 19.3% and 11.6% in the LAS group (log-rank test, χ2 = 0.109). No significant differences were found.
Conclusion
Compared with LAS, HALS radical gastrectomy for advanced distal gastric cancer had a lower conversion rate to open surgery, shorter surgical duration, and more thorough dissection of lymph nodes; 5- and 8-year OS and DFS rates were similar to those with LAS.
Keywords
Background
Hand-assisted laparoscopic surgery (HALS) is an important type of laparoscopic surgery in which the surgeon extends one hand into the abdominal cavity through a specific hand-assisted device, and completes the operation with laparoscopic instruments. HALS combines the traditional advantages of open surgery, restores the tactile function of the hand, reduces the surgical difficulty of laparoscopic surgery, and retains the minimally invasive advantages of laparoscopic surgery. 1 Both HALS and LAS have minimally invasive advantages in the treatment of advanced distal gastric cancer; however, which laparoscopic technology is best is unclear. To evaluate the superiority of HALS over LAS in radical gastrectomy for gastric cancer, patients with advanced distal gastric cancer were prospectively compared in our hospital from May 2009 to April 2013. The surgical results and initial outcomes were published in February 2017. 2 After publishing the initial results, we continued to follow the patients, and we report the final outcomes in the current article.
Materials and methods
General information
This study enrolled 124 patients, namely 62 patients in the HALS group and 62 patients in the LAS group. The reporting of this study conforms to the CONSORT statement. 3
Ethics statement
This study was approved by the ethics committee of the General Hospital of Western Theater Command.
Informed consent
All patients or their families provided written informed consent.
Randomization
The patients in this study were randomized using the envelope method. The envelopes were chosen and opened by a nurse who was blinded to the randomization. The two randomized groups comprised patients who underwent radical gastrectomy with HALS (HALS group) and patients who underwent radical gastrectomy with LAS (LAS group).
Inclusion criteria
The inclusion criteria were as follows: (1) willing to participate in the study and had regular follow-up; (2) generally in good condition and could tolerate endoscopic surgery; (3) aged 25 to 80 years with stomach cancer; and (4) tumor-node-metastasis (TNM) stage T2-4N0-3M0 (corresponding to stage Ib–III disease) and the tumor could be treated with D2 radical resection.
Exclusion criteria
The exclusion criteria were peritoneal dissemination or positive peritoneal lavage cytology found during intraoperative exploration, conversion to open surgery, and intraoperative resection of other organs.
Treatment
All patients underwent radical gastrectomy for gastric cancer under general anesthesia. The key operative points in D2 radical gastrectomy for gastric cancer with HALS are as follows: (1) Placing the hand port: The surgeon stands on the patient’s right side and makes an incision of approximately 7 cm long at the center of the upper abdomen approximately 2 cm below the xiphoid process. Dissection into the abdominal cavity then proceeds in layers, and the surgeon places the hand port into the incision. (2) Next, the surgeon retracts the transverse colon out of the abdominal cavity through the hand port, separates only part of the greater omentum and the transverse colon under direct vision, and peels off the anterior lobe of the transverse mesocolon to expose tissues and organs, such as the pancreas and the posterior wall of the stomach. (3) Pneumoperitoneum is established, and the lymph nodes of regions 4, 7, 8, 9, 11, 1, 3, 5, 6, and 12 are dissected in that order. The gastric body is then severed approximately 5 cm from the proximal edge of the tumor. (4) Pneumoperitoneum is released, the duodenal bulb is severed under direct vision, and digestive tract reconstruction is completed through the hand port. 4,5
Re-examination
Re-examination was performed every 3 to 6 months and comprised routine blood examination; liver function testing; renal function testing; measurement of electrolytes, carcinoembryonic antigen, and carbohydrate antigen 19-9; contrast-enhanced chest and abdominal computed tomography; and gastroscopy.
Follow-up
The patients in both groups were followed-up, and the follow-up duration, survival rates, and the results of each re-examination were recorded.
Statistical analysis
All statistical analyses were performed using SPSS for Windows, version 18.0 (SPSS Inc., Chicago, IL, USA). Survival curves were plotted using the Kaplan–Meier product-limit estimator method, and differences between survival curves were analyzed using the log-rank test. Statistical significance was set at P < 0.05.
Results
Patient characteristics and the number of dissected lymph nodes
There were no statistically significant differences in sex, age, tumor size, TNM stage, or underlying diseases between the two groups. Sixty-two patients underwent radical gastrectomy with HALS, and 62 patients underwent radical gastrectomy with LAS. In both groups, 55 patients received postoperative chemotherapy. The follow-up duration ranged from 6 to 96 months (median, 39.5 months). The number of dissected lymph nodes in the HALS group was higher than that in the LAS group (28.37 ± 11.12 vs 22.44 ± 5.64, respectively; t = 2.680, P = 0.007).
Comparison of overall survival between the HALS and LAS groups
The mean and median overall survival times of the patients in the HALS group were 52.00 ± 3.86 and 48.00 ± 6.26 months, whereas those in the LAS group were 48.98 ± 3.71 and 48.00 ± 5.64 months, respectively. The 5- and 8-year overall survival rates were 38.8% and 19.4% in the HALS group and 38.3% and 15.3% in the LAS group, respectively. The log-rank test showed no significant difference in overall survival between the two groups (χ2 = 0.250) (Figure 1).
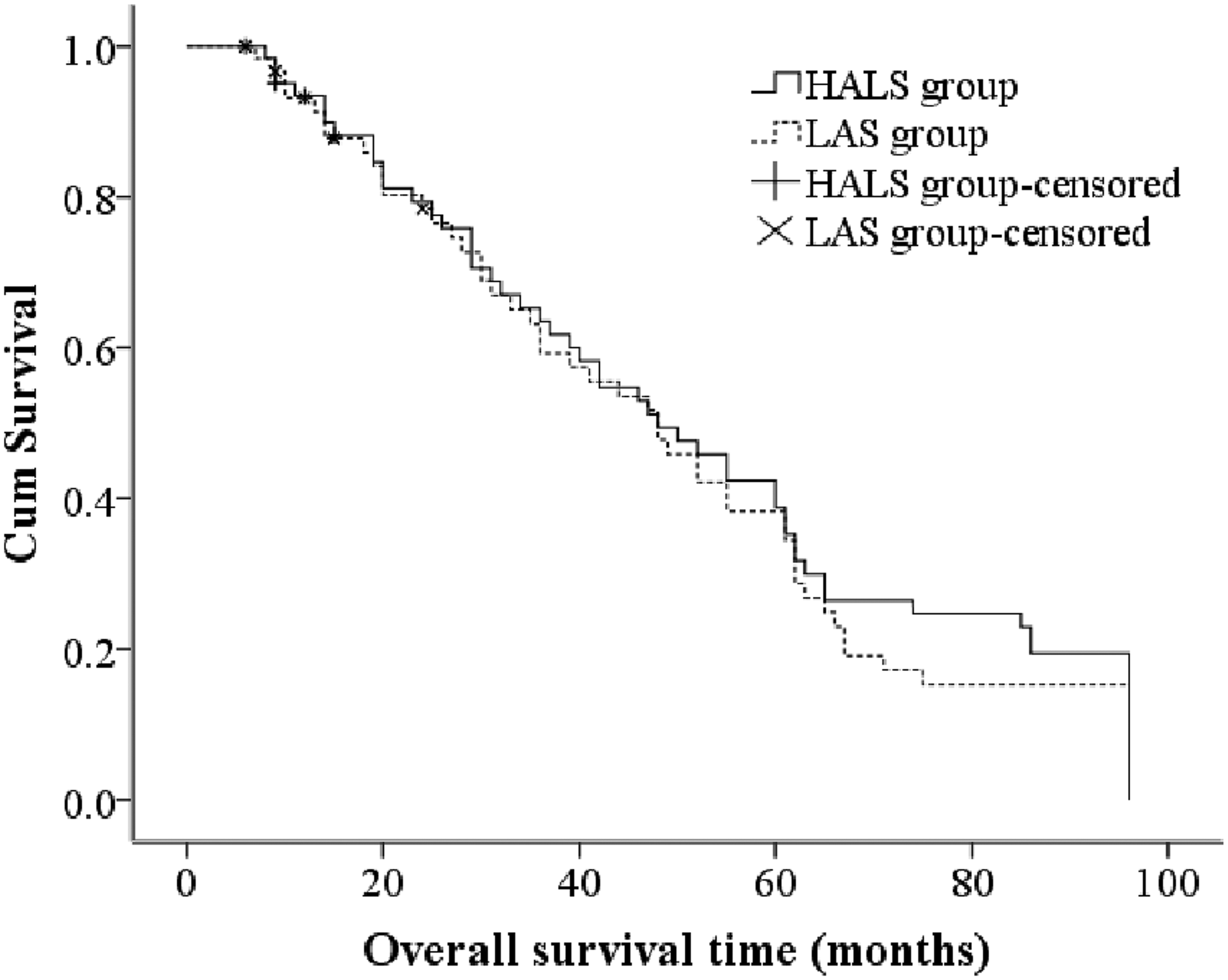
Kaplan–Meier postoperative survival curves for overall survival.
Comparison of disease-free survival between HALS and LAS groups
The mean and median disease-free survival times of the patients in the HALS group were 42.17 ± 3.68 and 39.00 ± 4.80 months, whereas those in the LAS group were 39.65 ± 3.75 and 39.00 ± 4.13 months, respectively. The 5- and 8-year disease-free survival rates were 23.1% and 10.6% in the HALS group and 19.3% and 11.6% in the LAS group, respectively. The log-rank test showed no significant difference in disease-free survival between the two groups (χ2 = 0.109) (Figure 2).
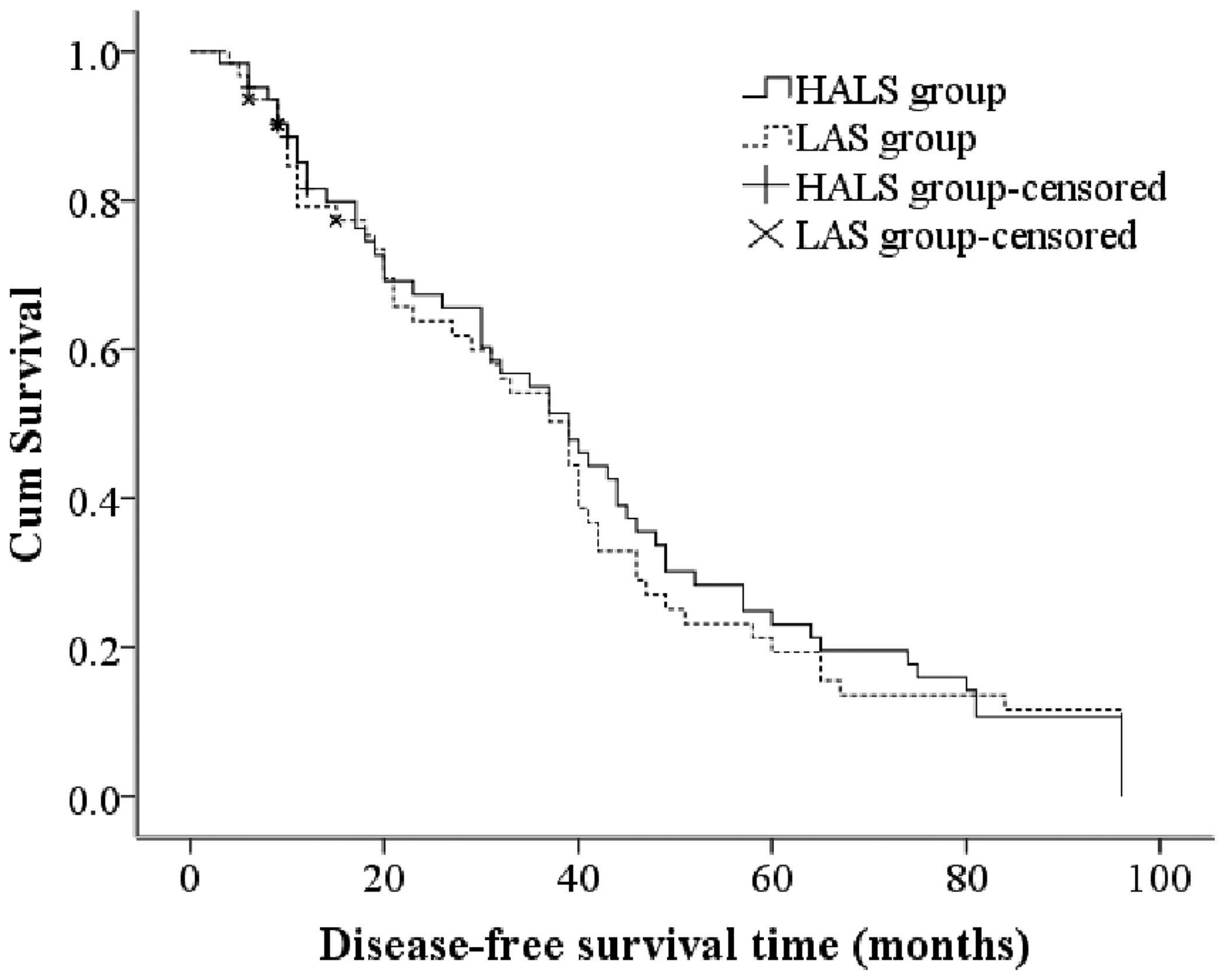
Kaplan–Meier postoperative survival curves for disease-free survival.
Discussion
China has a high incidence of gastric cancer, and currently, surgery is the main treatment. 6 Recently, with developments in laparoscopic instruments and the improvement of surgical skills, open radical gastrectomy is performed less often than previously, and laparoscopic radical gastrectomy for gastric cancer has become the mainstream surgical method in large and medium-sized hospitals in China. 5 Laparoscopic radical gastrectomy comprises three types: laparoscopic-assisted radical gastrectomy, total laparoscopic radical gastrectomy, and hand-assisted laparoscopic radical gastrectomy. The first two surgical methods are widely used clinically, and the associated radical tumor excision results and surgical safety are well-accepted. However, these two types of surgery also have disadvantages, such as the long learning curve, frequent need for a fixed surgical team, higher requirements for surgical cooperation, and totally laparoscopic surgery, generally, is difficult. 7 This raises the question of whether there is a simple and easy radical operation for gastric cancer. In 1999, Ohki et al 8 first reported a successful case of HALS in the treatment of gastric cancer, which initiated HALS as a treatment for gastric cancer. Previously, we reported 7 that HALS radical gastrectomy for gastric cancer was associated with satisfactory short-term results and could achieve a minimally invasive effect. Owing to the combination of the advantages of laparoscopic surgery and open surgery, HALS has gradually developed in clinical practice. Currently, HALS is performed for gastric cancer as well as colon cancer, 9 gynecological diseases, 10 urinary system diseases, 11 and liver and spleen diseases. 12,13
In HALS radical gastrectomy for gastric cancer, the complexity of the operation is greatly reduced compared with other methods because the auxiliary hand can provide tactile feedback and resist traction tissues. 14 Based on our clinical experience and previous studies, HALS has a short learning curve and is suitable for senior doctors with no basic knowledge of laparoscopic surgery and for primary hospitals. 15 HALS radical gastrectomy for gastric cancer can be completed by only a surgeon and an assistant. The assistant can be a standardized trained physician or a resident, and only approximately 20 minutes of pre-procedure training is required. Because only two doctors are directly involved in the operation, the difficulty associated with cooperation is greatly reduced, and the training time is shorter compared with laparoscopic-assisted radical gastrectomy, which often requires the direct participation of three doctors. Therefore, laparoscopic-assisted radical gastrectomy can be performed smoothly only with coordination and tacit understanding. Accordingly, laparoscopic-assisted radical gastrectomy usually takes longer than HALS to perform and requires continuous training in a large number of cases. Therefore, the difficulty of laparoscopic radical gastrectomy is significantly greater than that of HALS radical gastrectomy. 2
During HALS, the chief surgeon stands on the right side of the patient and is in the ideal hand position. In the dissection of the 4sa, 4sb, splenic hilar, and left cardia lymph nodes, the auxiliary hand of the chief surgeon plays an important role in the exposure of blood vessels and dissection of the perivascular lymph nodes. However, the exposure of these sites is difficult during LAS, especially in obese patients with gastric cancer. Additionally, during HALS, owing to hand-eye coordination and tactile feedback, the chief surgeon can use a hand to perform vascular compression and other procedures, which can address massive intraoperative bleeding quickly and reduces the possibility of surgical conversion to laparotomy. 16
As the operative difficulty of HALS decreases, the operation speed increases, and the operation time shortens. Regarding radical tumor treatment, the number of dissected lymph nodes in the HALS group was higher than that in the LAS group, showing a very good radical treatment effect.
This study showed that the 5- and 8-year overall survival rates were 38.8% and 19.4% in the HALS group and 38.3% and 15.3% in the LAS group, respectively. The 5- and 8-year disease-free survival rates were 23.1% and 10.6% in the HALS group and 19.3% and 11.6% in the LAS group, respectively. No significant differences were found between the groups regarding survival. These findings further confirmed the long-term efficacy of HALS for gastric cancer.
This study has some limitations. First, because this was a single-center study, potential bias could not be avoided, and multicenter studies are needed to verify our results. Second, the sample size was limited, and more cases are needed to draw a solid conclusion.
In conclusion, compared with laparoscopic-assisted D2 radical gastrectomy for advanced gastric cancer, HALS has the advantages of a lower rate of conversion to open surgery, shorter surgical duration, and more thorough lymph node dissection. Additionally, the long-term efficacy with HALS was similar to that with LAS.
Footnotes
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Department of Science and Technology, Sichuan Province, China (No. 2020YFS0491).