
Abstract
Objective
To compare the baseline clinical characteristics between patients with ROS1-positive and ALK-positive advanced non-small cell lung cancer (NSCLC), and the correlations of these subtypes with the distribution of metastases.
Methods
We compared the clinical characteristics and imaging features of patients with ROS1-positive and ALK-positive NSCLC using statistical methods.
Results
Data for 232 patients were analyzed. Compared with ALK-positive NSCLC, ROS1-positive NSCLC was more likely to occur in women (71% vs 53%), and primary lesions ≤3 cm were more common in patients with ROS1-positive compared with ALK-positive NSCLC (58% vs 37%). There was no significant difference in the distribution of metastases between the two groups. Subgroup analysis within the ROS1-positive group showed that, compared with primary lesions >3 cm, primary lesions ≤3 cm were more likely to present as peripheral tumors (72% vs 43%) and more likely to exhibit non-solid density (44% vs 4%).
Conclusions
Although ROS1-positive and ALK-positive NSCLCs show similar clinical features, the differences may help clinicians to identify patients requiring further genotyping at initial diagnosis.
Keywords
Introduction
Primary lung cancer is one of the most common malignant tumors in China. Treatment of non-small cell lung cancer (NSCLC) has progressed over the past decade from chemotherapy to personalized targeted precision therapy, in line with advancements in molecular medicine and the continuous emergence of targeted drugs. Gene mutations in c-ros proto-oncogene 1 (ROS1) and anaplastic lymphoma kinase (ALK) are popular therapeutic targets for NSCLC. The amino acid sequences of ROS1 and ALK show nearly 49% similarity, and the homology of ATP-binding sites in the kinase catalytic domain is as high as 77%.1–3 A recent multicenter study in China showed incidence rates of ALK and ROS1 rearrangements of 12.2% and 4.4%, respectively. 4 NSCLCs haboring either of these mutations show similar clinical features, and many ALK-tyrosine kinase inhibitors, such as crizotinib, ceritinib, lorlatinib, and brigatinib, have therapeutic effects in patients with either ROS1- or ALK-positive NSCLC.
Common sites of lung cancer metastasis include the brain, bone, liver, adrenal gland, and lungs. 5 Although ROS1 and ALK share a high degree of homology, the metastatic characteristics of tumors with these different mutations remain unknown, and evidence on this topic is currently lacking. In this study, we therefore compared the clinical characteristics and imaging features of ROS1-positive and ALK-positive NSCLCs and investigated the correlations of these mutations with their metastatic distribution. This study aimed to provide a basis for the clinical screening and treatment of patients with ROS1-positive and ALK-positive NSCLC.
Patients and Methods
Study population
Patients admitted to Shanghai Pulmonary Hospital with NSCLC between March 2018 and March 2020 were included in this retrospective study. All patients met the following inclusion criteria: 1) histologically or cytologically confirmed locally advanced or metastatic NSCLC (including patients with stage IIIB to IV at initial diagnosis); (2) ROS1 or ALK rearrangement detected by amplification-refractory mutation system (ARMS) or positivity for ROS1 or ALK fusion protein detected by immunohistochemistry; and (3) complete imaging data at the initial diagnosis. This study was approved by the Ethics Committee of Shanghai Pulmonary Hospital. All patients provided written informed consent for inclusion in this study.
Imaging analysis
The clinical characteristics and baseline imaging features of patients with ROS1-positive and ALK-positive NSCLC were collected. Imaging examination items included chest computed tomography (CT), whole-body positron-emission tomography/CT, abdominal ultrasound, color Doppler ultrasonography for supraclavicular or cervical lymph nodes, whole-body bone imaging, and contrast-enhanced cranial magnetic resonance imaging. All the above imaging examinations were performed in all the patients. The size (maximal diameter ≤3 cm or >3 cm), axial location (central or peripheral), density (solid or non-solid), cavitation, and air bronchograms of the primary tumor were analyzed. Tumor-node-metastasis (TNM) staging was annotated according to The Eighth Edition Lung Cancer Stage Classification (AJCC/UICC, 2017). 6 The presence of metastases was recorded by site. Images were also assessed for pleural effusion and lymphangitic carcinomatosis.
Statistical analysis
All statistical analyses were carried out using SPSS Statistics for Windows, Version 25.0 (SPSS Inc., Armonk, NY: IBM Corp). Continuous and categorical data were compared using independent samples t-tests and χ2 tests, respectively. All tests were two-sided. P values <0.05 were considered significant. A multivariable logistic regression model was built with candidate predictors chosen according to a value of P < 0.20 in univariate analysis.
Results
A total of 232 NSCLC patients were included in this study, including 55 ROS1-positive and 177 ALK-positive patients (Table 1). Among these, 209 patients were detected by ARMS (51 with ROS1 rearrangement and 158 with ALK rearrangement) and 23 patients were detected by immunohistochemistry (4 ROS1 fusion protein-positive and 19 ALK fusion protein-positive). Regarding pathological type, all but three cases were adenocarcinoma, with no significant difference between the two groups in terms of TNM staging (Table 1). Two patients in the ROS1-positive group had other gene mutations, including one patient with a KRAS (Kirsten rat sarcoma viral oncogene homolog) mutation and one patient with an L858R point mutation in the epidermal growth factor receptor gene. ROS1-positive NSCLC was significantly more likely to occur in women than ALK-positive NSCLC (71% vs 53%, P = 0.020) (Table 1).
Characteristics of all patients (n = 232).
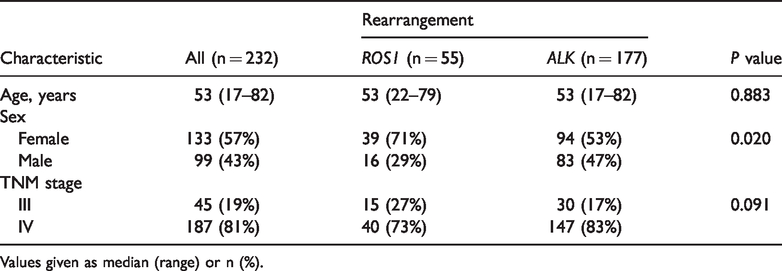
Values given as median (range) or n (%).
According to univariate analysis, significantly more patients in the ROS1-positive group had primary lesions ≤3 cm compared with the ALK-positive group (58% vs 37%, P = 0.006) (Table 2). There was no significant difference in the distribution of metastases between the two groups (Table 3). We analyzed the variables able to distinguish between ROS1-positive and ALK-positive NSCLC using a multivariable logistic regression model with sex, TNM stage, primary tumor size, and bone metastasis. Holding other covariates fixed, the odds of having ROS1-positive NSCLC were significantly higher in women than in men (P = 0.033; odds ratio [OR]=2.080, 95% confidence interval [CI]: 1.059–4.082) and in patients with primary lesions ≤3 cm compared with those with primary lesions >3 cm (P = 0.005; OR=2.476, 95%CI: 1.315–4.663). Typical imaging features of ROS1-positive and ALK-positive patients are shown in Figure 1.
Primary tumor imaging features in all patients (n = 232).

Values given as n (%).
Distribution of lymphadenopathy and metastases (n = 232).
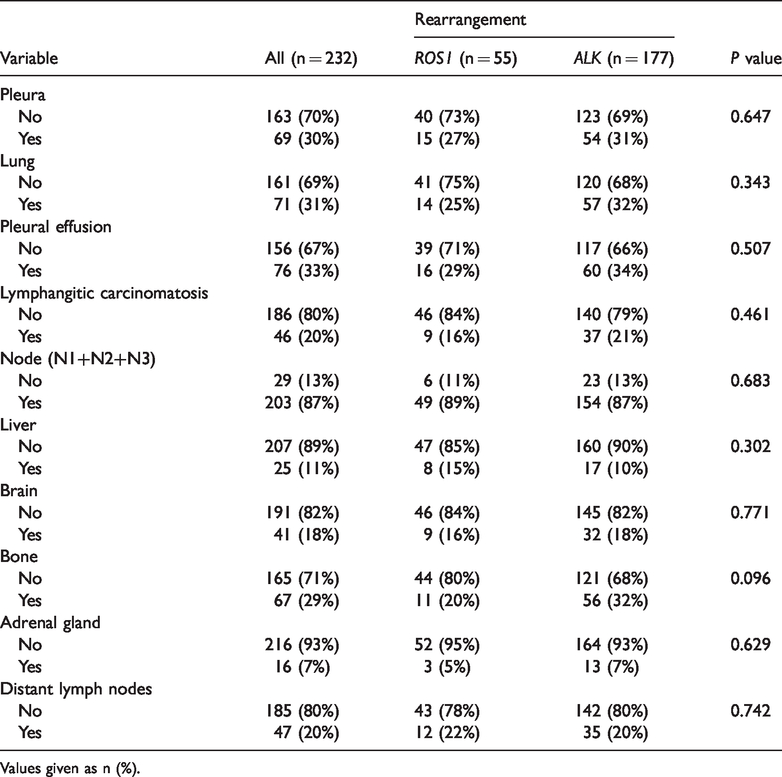
Values given as n (%).
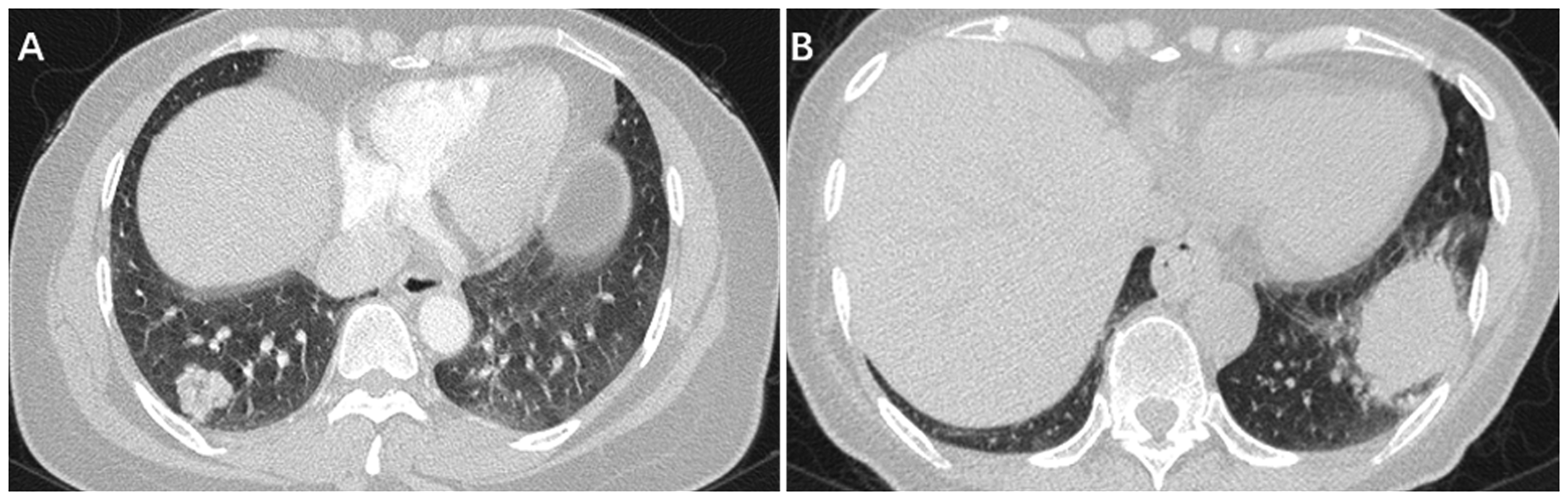
Typical imaging features of ROS1-positive and ALK-positive patients with non-small cell lung cancer. (a) A 49-year-old woman with adenocarcinoma. Computed tomography (CT) image showing a 2.2-cm non-solid nodule in the right lower lobe. ROS1 rearrangement was detected by amplification-refractory mutation system (ARMS). (b) A 63-year-old woman with adenocarcinoma. CT image showing a 4.7-cm solid nodule in the left lower lobe. ALK rearrangement was detected by ARMS.
We further subdivided ROS1-positive patients into patients with primary tumors ≤3 cm and >3 cm, respectively. Primary lesions ≤3 cm were more likely to present as peripheral tumors (72% vs 43%, P = 0.034), and more likely to exhibit non-solid density (44% vs 4%, P = 0.001) compared with larger primary lesions >3 cm (Table 4).
Characteristics and imaging features of ROS1-positive patients (n = 55).

Values given as median (range) or n (%).
Discussion
Rikova et al. 7 and Soda et al. 8 first reported the presence of the echinoderm microtubule-associated protein-like 4 (EML4) and ALK (EML4–ALK) fusion gene in lung cancer in 2007, and this fusion gene was confirmed as a driver gene for lung carcinogenesis. ALK-positive lung cancer was subsequently identified as a specific molecular subtype of NSCLC in 2009. 9 Rikova et al. 7 also found that ROS1 was activated by gene rearrangements, resulting in the novel chimeric fusion proteins SLC34A2–ROS1 and CD74–ROS1. Subsequent work has identified such rearrangements in 1% to 2% of NSCLCs, representing a distinct molecular subgroup.2,10,11
Distant metastasis is a complex process involving the regulation of multiple gene and signaling pathways. 12 Previous studies have shown that changes in corresponding genes in different signaling pathways may be related to metastatic spread to different organs, and biological alterations in the tumor may affect its metastatic behavior and pattern. 13 Hoshino et al. 14 found molecules present on tumor-derived exosomes that ‘addressed’ them to specific organs, suggesting that the metastatic process is programmed. However, information on the correlation between gene mutations and organ metastasis, and the mechanism connecting them, is still lacking.
In the current study, the median age at diagnosis in both ROS1-positive and ALK-positive patients was 53 years. In contrast, Digumarthy et al. 15 found that patients with ROS1 rearrangements were older than patients with ALK rearrangements (median 55 vs 50 years, P = 0.01). Park et al. 16 reported that the median age of 103 patients with ROS1 rearrangements, including patients with stage I and stage II, was 56 years. Wu et al. 17 found no significant difference in age between ROS1-postitive and ROS1-negative patients, although the median age of ROS1-postitive patients tended to be younger (53 vs 62 years). Li et al. 18 found a median age of 50.8 years (range 32–78 years) among 36 patients with ROS1 rearrangement. In summary, the median age of ROS1-positive NSCLC patients is approximately 50 years, and both ROS1-positivity and ALK-positivity are more likely to occur in younger patients.
The current study found a difference in sex distribution between ROS1-positive and ALK-positive patients, with a significantly higher percentage of women in the ROS1-positive group (71% vs 53%, P = 0.020). Multivariate analysis confirmed that the odds of ROS1-positivity were significantly higher in women than in men (P = 0.033; OR=2.080, 95%CI: 1.059–4.082). Digumarthy et al. 15 also found a higher proportion of women in the ROS1-rearrangement (72%) compared with the ALK-rearrangement group (45%), and Park et al. 16 found a higher proportion of women (68.9%) than men among patients with ROS1 rearrangement. The higher frequency of ROS1 rearrangement among women than men in the current study was thus consistent with previous studies.19–21 However, Song et al. 4 found similar proportions of female patients in the ALK- and ROS1-rearrangement groups (52.8% and 53%, respectively). The discrepancy between these results may have been due to the low disease incidences and small sample sizes of the studies.
Analysis of the imaging features revealed significantly more primary lesions ≤3 cm in the ROS1-positive compared with the ALK-positive group (58% vs 37%, P = 0.006), but no significant differences in any other imaging features between the two groups. No previous studies have reported differences in the sizes of the primary tumors between patients with these two gene rearrangements. Further subgroup analysis of the ROS1-positive group also showed that primary lesions ≤3 cm were more likely to present as peripheral tumors (72% vs 43%, P = 0.034) and more likely to exhibit non-solid density (44% vs 4%, P = 0.001) compared with primary lesions >3 cm. Song et al. 4 found non-solid lesions in 71% and 76% of patients with ROS1 and ALK rearrangements, respectively. However, Digumarthy et al. 15 found that virtually all (98%) ROS1-rearrangement tumors showed solid density.
The comparative metastatic features of ROS1-positive and ALK-positive tumors remain unclear. Gao et al. 13 reviewed multiple studies and found that patients with ALK rearrangements were more prone to lymph node, pleural, and brain metastases. Digumarthy et al. 15 compared the CT features of ROS1- and ALK-rearrangement patients and found significantly lower incidences of brain and extrathoracic metastases in patients with ROS1 compared with ALK rearrangement (9% vs 25%, P = 0.03; 49% vs 75%, P < 0.01). A previous retrospective study found that ALK rearrangement in lung adenocarcinoma was correlated with lymph node and pleural metastases, with distant lymph node metastasis mostly occurring in the abdominal cavity, few axillary lymph node metastases, and pleural metastasis manifested as pleural nodules or malignant pleural effusion. 22 The current study found no significant differences in the distributions of major metastases, such as pleural (27% vs 31%), liver (15% vs 10%), bone (20% vs 32%), and brain metastases (16% vs 18%), between the ROS1- and ALK-positive groups. This result may still be due to the small sample sizes.
According to the “seed” theory, the most common metastatic location of lung cancer is the brain, accounting for up to 50% of all metastases, followed by bone, liver, and adrenal glands. 23 In a phase II clinical study, Wu et al. 24 found an incidence of brain metastases in ROS1-rearrangement patients of 18.1%, which was similar to our current results. Patil et al. 25 found no difference in the incidence of brain metastases between ROS1- and ALK-rearrangement patients.
Gainor et al. 26 found that the incidences of extrathoracic and brain metastases were significantly lower in the ROS1-rearrangement compared with the ALK-rearrangement group (59.0% vs 83.2%, P = 0.002; 19.4% vs 39.1%, P = 0.033). In addition, progression-free survival (PFS) after crizotinib treatment was significantly longer in the ROS1 than in the ALK group (11 vs 7.9 months, P = 0.007), with no difference in overall survival (OS) between the two groups (2.5 vs 3 years). Liu et al. 27 found that ALK-rearrangement patients with adrenal metastasis at baseline had poorer PFS, and Ock et al. 28 showed that patients with at least three metastatic organs had significantly shorter PFS and OS among patients with ALK-positive NSCLC. Pacheco et al. 29 also showed that more baseline metastases was associated with shorter OS.
This study had several limitations associated with the investigation of rare mutations. The sample size was small and samples were collected over a long period of time, leading to imbalance between the experimental groups. In addition, we did not analyze the correlation between metastatic distribution and treatment efficacy, which is worthy of further investigation.
In conclusion, this study identified differences in clinical and imaging features between patients with NSCLC with ROS1 and ALK rearrangements, including differences in the proportions of women and of primary lesions ≤3 cm. These results need to be validated in future studies with larger sample sizes. However, the presence of these features may help clinicians to determine which NSCLC patients require further genotyping at the initial diagnosis.