
Abstract
With the advent of targeted therapy for non-small-cell lung cancer, there are many new available treatment options for patients whose cancer harbors an actionable mutation or alteration. These new medications come with numerous side effects, for some of which, the management is not well defined. Alectinib is a second-generation tyrosine kinase inhibitor approved for stage-IV lung adenocarcinoma with anaplastic lymphoma kinase gene rearrangement. Severe (⩾Grade 3) skin rash is a rare side effect of alectinib. Reintroducing alectinib in patients with severe skin rash is not well defined in the medical literature. While other case reports have outlined their approach and desensitization protocol, the maximum dose that patients were titrated up to in a desensitization protocol was 300 mg twice daily. Here, we report a case of Grade 3 skin rash secondary to alectinib, and our experience in managing the rash and reintroducing alectinib with a unique desensitization protocol to a max of 600 mg twice daily (full dose). This case could provide further guidance to oncologists managing patients with this adverse event and may aid in reducing concerns to both patients and physicians about recurrence of skin rash at the maximum dose.
Introduction
The anaplastic lymphoma kinase (ALK) gene rearrangement is found in 2%–7% of advanced non-small-cell lung cancer (NSCLC) patients. 1 Tyrosine kinase inhibitors (TKIs) that target this rearrangement are more effective in the management of such patients, with improved response rate and progression-free survival compared with chemotherapy. Alectinib is one of the first-line treatments for ALK-positive stage-IV lung adenocarcinoma.1,2 Severe (⩾Grade 3) skin rash due to the medication is rare. In the ALEX trial, 1% of patients developed Grade 3 rash, while in the J-ALEX trial, 2.9% developed Grade 3 rash.2,3 Pooled data from NP28673 and NP28761 trials reported Grade 3 rash in 1% of patients. 4 In the ALUR and AF-001JP studies, there were no reports of ⩾Grade 3 rash.5,6 The approach for managing patients with Grade 3 adverse events in these trials, involved dose interruptions and dose reductions but no desensitization protocol was reported. To our knowledge, only three case reports outlined desensitization protocols.7–9 Here, we report a case of Grade 3 skin rash due to alectinib and our desensitization protocol.
Case
A 57-year-old woman, with history of stage IIIB non-small-cell lung adenocarcinoma, was initially treated with concurrent chemo-radiation with cisplatin 75 mg/m2 and pemetrexed 500 mg/m2 every 3 weeks for three cycles followed by adjuvant durvalumab 10 mg/kg every 2 weeks, which started 5 weeks after completing chemo-radiation. She had progression of disease in the mediastinal lymph nodes after 19 cycles of durvalumab. Repeat biopsy of a mediastinal lymph node revealed adenocarcinoma with programmed death ligand 1 (PD-L1) 10%. The patient then started a combination of carboplatin AUC 6, paclitaxel 200 mg/m2, atezolizumab 1200 mg, and bevacizumab 15 mg/kg, and received two cycles with partial response. Genomic testing revealed ALK-EML4 rearrangement.
Alectinib 600 mg twice daily was started 4 weeks after her last dose of chemo-immunotherapy. Twelve days after, the patient presented with an itchy, red skin rash on her neck, face and back. There was no history of allergies, or new medications to explain her rash. On examination, she was afebrile, with vital signs within normal limits; maculopapular rash seen on neck (Figure 1), back (Figure 2) and face with BSA ⩾ 30%, (Grade 3) with a Naranjo score of 9 (previous conclusive report on this reaction +1, adverse event appear after drug administered +2, adverse event improved when drug discontinued +1, causal association known and re-challenge at the same dose cannot be done +2, alternative causes +2, confirmed by objective clinical evidence +1). There was no mucosal involvement, and examination of other organ systems was unremarkable.

Maculopapular rash of neck.

Maculopapular rash of back.
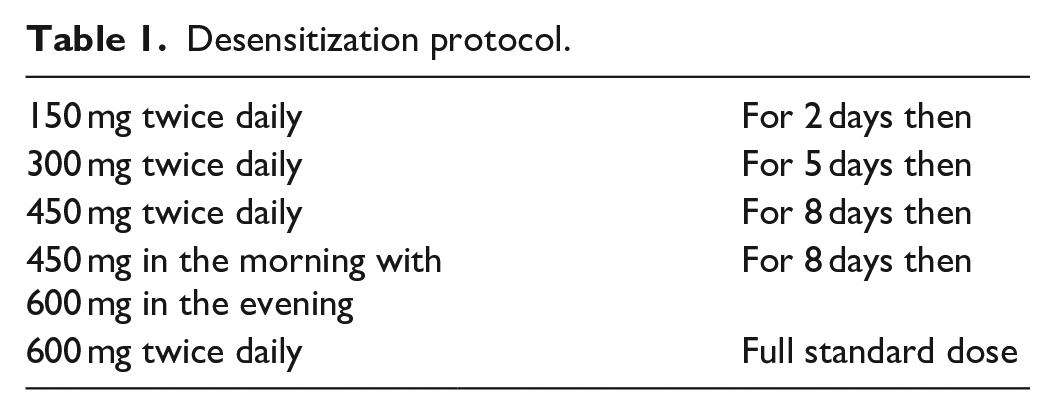
Alectinib was stopped, and a tapered dose of methylprednisolone given over 5 days. The rash resolved by Day 19. Alectinib was restarted Day 21 and titrated up to the full dose of 600 mg twice daily. The following desensitization protocol (Table 1 and Figure 3) was employed:
150 mg twice daily for 2 days; then
300 mg twice daily for 5 days; then
450 mg twice daily for 8 days; then
450 mg in morning with 600 mg in evening for 8 days; then
600 mg twice daily.
Patient tolerated this protocol without any recurrence of the rash. One year later, she continued to be on the full-dose alectinib without any adverse effects and had stable disease on imaging.
Desensitization protocol.

Case timeline and desensitization protocol.
Discussion
Severe skin rash (⩾Grade 3) is an uncommon but previously reported side effect of alectinib. Our patient had a Naranjo score of 9 indicating a definite probability of adverse drug reaction. 10 Reintroducing alectinib with a desensitization protocol is not well-established.7,11 A literature review identified four cases (Table 2), of which three outlined their desensitization protocol.7–9 In all four, the skin rash occurred 10–14 days of starting alectinib and did not reoccur after the desensitization protocol.
Literature review of patients with alectinib skin rash including our case.

There is no universal desensitization protocol. In designing one, the initial dose is usually much smaller than the target level, and gradually titrated up.13,14 The time interval between doses and dose increments are based on the pharmacokinetics, hypersensitivity history and comorbidities. 14 In patients with exanthems, a gradually increasing dose, lasting days to several weeks is reasonable. 14 Most protocols increase doses by incremental steps of two-times to ten-times the previous dose. 15 While there are protocols for alectinib in the literature (Table 2), these protocols are variations on the theme of gradual dose-up titration from a low starting dose. Where there are no validated protocols, physicians may have to tailor a regimen for their patients. 15
Our protocol differed from the other three cases.7,8 The restarting doses of alectinib in the other three cases were very low (20 mg, 37.5 mg and 40 mg), whereas we started at a higher dose of 150 mg twice daily.7–9 Since alectinib comes in 150 mg capsules, we believe our starting dose was more convenient and feasible. Furthermore, considering that our patient had no prior allergies and experienced no additional complications except for a rash which completely resolved after stopping the medication, we felt it was reasonable to start at 150 mg twice daily with very close monitoring. Based on the pharmacokinetics of alectinib which peaks in 4 h and has a half-life of 33 h, there was still room to decrease the starting dose to 150 mg once daily or use a reduced dose via compounded formulation as in prior care reports; however, we felt this was unnecessary based on the hypersensitivity history or our patient.
There is no data on the efficacy of alectinib when reintroduced via the desensitization process. While previous studies showed that chemotherapy given by desensitization was not therapeutically inferior to the regular infusion. 13 These data may not be applicable to alectinib; therefore, long-term follow-up of patients desensitized with alectinib would be needed to determine if there was any loss of efficacy in these patients. Of note, to the time of submitting this manuscript, the patient continues to be on the same dose of alectinib and is maintaining a durable response.
In the other three cases alectinib was titrated to 300 mg twice daily and 200 mg twice daily,7–9 whereas we titrated to 600 mg twice daily. Although providers in the other two cases completed the desensitization protocol in a shorter period of time (8, 9 and 14 days compared to 23 days in our case),7–9 we were able to reach a higher dose than their final dose by Day 3.
We understand that some providers may be reluctant to titrate to the full dose of alectinib after Grade 3 skin rash in fear of seeing another episode; however, this may lead to patients not receiving the full benefit of alectinib. Physicians should consider when feasible, titrating to the standard dose as long as the patient experiences no recurrence of the skin rash during the desensitization process. We realize that our approach may not work for every patient, and some patients may not tolerate the full dose, therefore staying on a lower dose may be indicated.
We recognize the limitations in our case report where prior immunotherapy exposure may have been an unproven confounding variable in development of the skin rash; however, we thought this less likely as immunotherapy-related adverse effects after introducing TKIs are reported with osimertinib and not with other TKIs. 16 Finally, every patient is unique, and therefore, no single desensitization protocol may fit all.
Conclusion
Severe skin rash is a rare adverse event in patients treated with alectinib. Use of an appropriate desensitization protocol may allow safe reintroduction of this medication to the full dose of 600 mg twice daily.
Supplemental Material
author-declaration-template-case-reports-and-case-series-0 – Supplemental material for Patients with high-grade alectinib-induced skin rash: How do we desensitize these patients? A case report and review of literature
Supplemental material, author-declaration-template-case-reports-and-case-series-0 for Patients with high-grade alectinib-induced skin rash: How do we desensitize these patients? A case report and review of literature by Karan Seegobin, Umair Majeed, Yanyan Lou, Yujie Zhao and Rami Manochakian in SAGE Open Medical Case Reports
Footnotes
Acknowledgements
Special thanks to the patient who provided us with the pictures and approved publishing the report.
Author contributions
All authors reviewed, edited and approved the final contents.
Declaration of conflicting of interests
R.M. discloses advisory board in AstraZeneca and advisory board for Guardant Health, Novocure and Takeda and consultancy in AstraZeneca. Y.L. discloses advisory board in AstraZeneca and Novocure; consultancy in AstraZeneca; honoraria in Clarion Health Care; research funding support from Merck, MacroGenics, Tolero Pharmaceuticals, AstraZeneca, Vaccinex, Blueprint Medicines and Sun Pharma; and advanced research from Bristol-Myers Squibb, Kyowa Pharmaceuticals and Tesaro.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Informed consent
Written informed consent was obtained from the patient for their anonymized information to be published in this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.