
Abstract
Objective
Anaplastic lymphoma kinase (ALK) rearrangement is an important oncogenic driver in some non-small cell lung cancers (NSCLC). Treatment with ALK tyrosine kinase inhibitors improves survival. The availability of diagnostic immunohistochemistry (IHC) has led to a paradigm shift in ALK testing. This study examined the prevalence of ALK rearrangement in Jordanian patients with NSCLC and compared the results of IHC and fluorescence in situ hybridization (FISH) for detecting ALK rearrangement.
Methods
This retrospective study on 449 patients with NSCLC treated at the King Hussein Cancer Center in Jordan tested biopsy samples for ALK rearrangement using FISH and/or IHC (D5F3) between 2018 and 2020.
Results
Eighteen patients (4%) had ALK-positive NSCLC. The calculated sensitivity and specificity of ALK immunostaining compared with FISH were 87.5% and 96%, respectively. ALK-positive patients were significantly younger than their ALK-negative counterparts, and women were three times more likely to carry ALK rearrangement than men. ALK rearrangement was significantly associated with smoking history, with most ALK-positive patients being non-smokers, former smokers, or light smokers.
Conclusions
IHC is a reasonable alternative to FISH for ALK testing with advantages in terms of robustness, turnaround times, and cost-effectiveness.
Keywords
Introduction
Lung cancer was the second most common cancer and the main cause of cancer mortality in 2020. There were an estimated 2.2 million new cancer cases and 1.8 million deaths in 2020, accounting for approximately one-tenth (11.4%) of new cancer diagnoses and one-fifth (18.0%) of cancer-related deaths. 1 Smoking is responsible for the relatively high incidence of lung cancer in Jordan, where lung cancer is the most common cancer in men and the leading cause of cancer-related death in both sexes. 2
Non-small cell lung cancer (NSCLC) accounts for roughly 80% of lung cancers, and it is a leading cause of cancer-related deaths worldwide.1,3 It is frequently diagnosed in advanced stages and is associated with a short survival time. Although the prognosis of this disease is dismal, significant advances in the genetics and treatment of NSCLC have recently been made. Over half of lung adenocarcinomas carry one of several identifiable genetic alterations. Some of these alterations can be targeted by specific therapeutic inhibitors that are either approved by the US Food and Drug Administration or undergoing clinical trials. 4 Chromosomal rearrangement involving the ALK gene is present in approximately 5% of lung adenocarcinomas, most commonly in the form of an intrachromosomal inversion leading to the EML4–ALK fusion product, which is associated with ALK protein overexpression.5–7 Patients with ALK-rearranged NSCLC are usually non-smokers or light smokers with a younger age at diagnosis (mean, approximately 54 years). 8 The majority of ALK-positive patients have progressive disease at the time of diagnosis, indicating the aggressiveness of these tumors and their tendency to metastasize. 9
Patients with this tumor type are responsive to ALK tyrosine kinase inhibitors (TKIs) such as crizotinib;10,11 however, resistance develops after a few months of treatment. More potent second- and third-generation ALK inhibitors have exhibited efficacy following relapse, and they have been approved for patients with resistance or intolerance to crizotinib.12,13
The currently approved methods for ALK testing in metastatic NSCLC include immunohistochemistry (IHC) and fluorescence in situ hybridization (FISH). FISH, using break-apart probes, has been considered the “gold standard” for detecting ALK rearrangements. 14 Recent findings illustrated that IHC using the 5A4 or D5F3 clone is highly sensitive and specific for ALK gene rearrangement in lung adenocarcinoma, and IHC can be used as an accurate and equivalent alternative to FISH for ALK testing. 15 The US Food and Drug Administration has approved the Ventana ALK (D5F3) CDx Assay as a companion diagnostic for crizotinib, ceritinib, and alectinib.16–18 Furthermore, IHC is a routine testing method in the majority of pathology laboratories and a cost-effective alternative to more expensive and labor-intensive molecular testing techniques.
A review of the available literature revealed some variation of ALK rearrangements in NSCLC based on studies in White, Asian, and African populations.5,19–27 Nevertheless, less is known about the Middle East population. This study examined the frequency of ALK rearrangement in a group of Jordanian patients with NSCLC and compared IHC and FISH for detecting ALK gene rearrangement.
Materials and methods
This retrospective study encompassed patients with NSCLC treated at King Hussein Cancer Center (Amman, Jordan) between 2018 and 2020 whose biopsy samples were tested for ALK rearrangement using FISH and/or IHC. Tissues from small biopsies or lung resection specimens were used. This study was approved by the Institutional Review Board at King Hussein Cancer Center, and the reporting of this study conforms to STROBE guidelines. 28 The requirement for informed consent was waived by the Institutional Review Board as this study is a retrospective data collection study with no patient identifiers used.
Patient records were reviewed to collect information regarding age, sex, and smoking history. The tumor type, grade, and stage were determined. Each patient’s response to TKI therapy, if any, was assessed.
IHC was performed strictly in accordance with the manufacturers’ protocols for immunohistochemical staining. For this purpose, paraffin-embedded tissue fixed in 10% neutral buffer formalin for 6 to 72 hours was used. Then, unstained histologic sections (2–4 µm thick) on charged slides were used in all cases. On a Ventana-Roche BenchMark XT Automated Slide Stainer (Roche-Ventana, Tucson, AZ, USA), immunostaining was performed using Ventana anti-ALK (D5F3 clone Ready-To-Use Rabbit Monoclonal Primary Antibody, Roche-Ventana), an OptiView DAB IHC Detection Kit (Roche-Ventana), and an OptiView Amplification Kit (Roche-Ventana). Strong granular cytoplasmic staining in tumor cells denoted positivity for ALK (any percentage of positive tumor cells; Figure 1). A positive control and a negative reagent control were used for every case.

ALK immunohistochemistry performed on a cell block from a pleural fluid-containing metastatic adenocarcinoma. (a) Hematoxylin and eosin staining and (b) ALK immunostaining (D5F3).
FISH was performed on formalin-fixed, paraffin-embedded tumor samples using a probe specific to the ALK locus (Vysis LSI ALK dual color, break-apart rearrangement probe; Abbott, Abbott Park, IL, USA) in accordance with the manufacturer’s instructions. The FISH results were analyzed under a fluorescence microscope (Zeiss Axio Imager M1, Carl Zeiss AG, Oberkochen, Germany) with the appropriate filters. At least 50 neoplastic cells were counted. The result was considered positive if >25 cells (>25/50 or >50%) displayed split orange and green signals or an isolated orange signal.29,30
Microsoft Excel version 2013 (Microsoft, Redmond, WA, USA) was used for data analysis. Descriptive statistics using frequencies and percentages were applied. Sensitivity and specificity for IHC results were calculated using the equations presented in Table 1.
Sensitivity and specificity rate calculation.
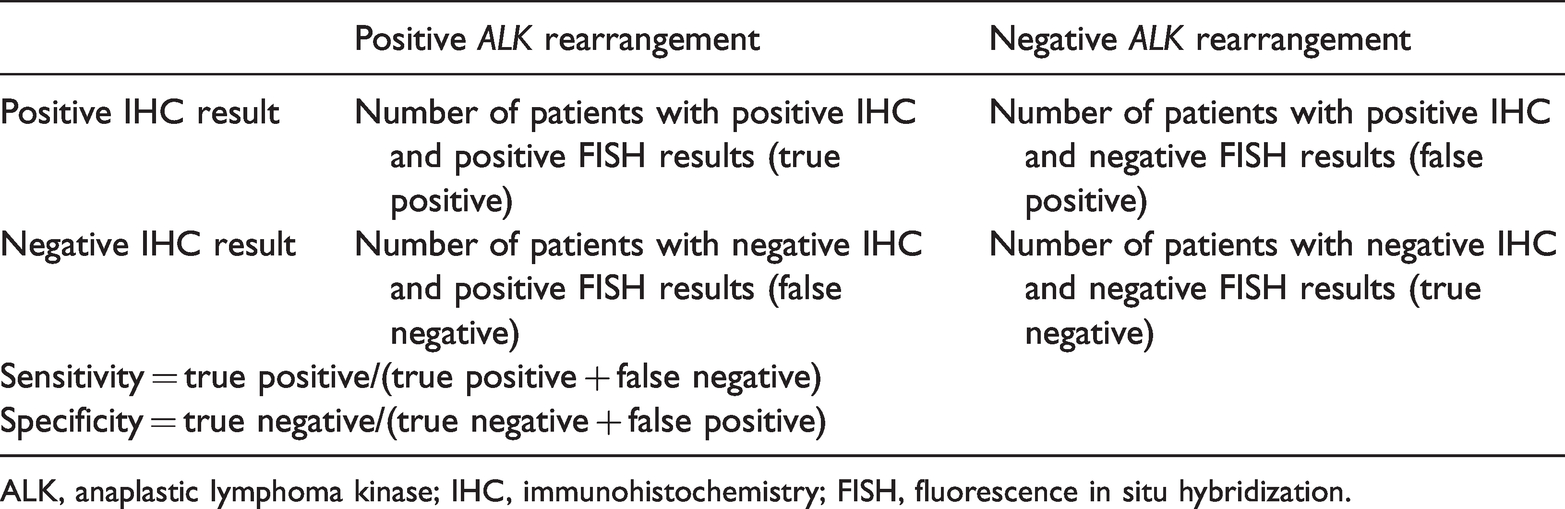
ALK, anaplastic lymphoma kinase; IHC, immunohistochemistry; FISH, fluorescence in situ hybridization.
Univariate analysis was performed using Student’s t-test for continuous variables, and the differences in proportions were tested using the chi-square test or Fisher’s exact test.
Results
During the study period, 449 patients with confirmed NSCLC were included in the study. The population consisted of 336 men (74.8%) and 113 women (25.2%) with a median age of 62 years (range, 21–92 years). The most common tumor type was pure adenocarcinoma (370 [82.4%]), followed by squamous cell carcinoma (10.5%) and adenosquamous carcinoma (3.8%). Data on smoking status were available for 371 patients. Most tumors were moderately or poorly differentiated (Table 2).
Clinicopathological features of patients with non-small cell lung cancer.

NOS, not otherwise specified.
IHC for ALK was performed in all patients, whereas FISH for ALK gene rearrangement was performed in 34 patients. Of the 449 patients with NSCLC, 18 carried ALK-positive tumors (4%). Seven patients were positive for ALK by both IHC and FISH, and nine patients were positive for ALK by IHC but were not tested by FISH. In addition, one patient who was ALK-positive by IHC and ALK-negative by FISH had a significant response to ALK TKI therapy. One patient was ALK-negative by IHC but ALK-positive by FISH, and this patient did not receive ALK TKIs. The calculated sensitivity and specificity of ALK D5F3 immunostaining compared with FISH results in the current study were 87.5% and 96%, respectively.
The 18 patients who were positive for ALK rearrangement included 9 men and 9 women with a mean age of 54.67 (range, 21–72) years. Of the 16 patients with available smoking data, 4 were heavy smokers. Four patients had a family history of cancer, including two patients with first-degree relatives. The majority of the tumors were adenocarcinomas (nine were poorly differentiated, seven were moderately differentiated, and one was mucinous), and one tumor was an adenosquamous carcinoma. At the time of diagnosis, all ALK-positive patients had advanced to progressive disease with metastasis (Table 3).
Characteristics of individual patients with ALK-positive non-small cell lung cancer.

ALK, anaplastic lymphoma kinase; IHC, immunohistochemistry; FISH, fluorescence in situ hybridization.
ALK-positive patients were significantly younger than those with negative results (54.67 years vs. 61.45 years, P = 0.05; Table 4). Women were three times more likely than men to have ALK rearrangement (P = 0.013). There was a significant association between ALK rearrangement and smoking history, with most positive patients being non-smokers, former smokers, or light smokers (P = 0.013).
Relationship between ALK positivity and clinicopathological features.

Data are mean ± standard deviation or n (%).
Discussion
Lung cancer is one of the most frequent cancers globally, and is the deadliest, accounting for 1.8 million deaths each year. 1 Nonetheless, significant discoveries have improved the management and treatment of NSCLC, most notably the identification of particular oncogenic drivers that direct treatment selection toward the most effective targeted therapy. Among these therapies, ALK inhibitors have displayed efficacy in patients with NSCLC harboring ALK rearrangement. These therapies have produced impressive response rates and progression-free survival rates and cause less treatment-related death compared with chemotherapy. 31 Therefore, ALK testing should be performed in all patients with advanced NSCLC. In the present study, which is—to our knowledge—the first to document the frequency of ALK rearrangement in the Jordanian population, we observed a frequency of 4%. This rate is comparable to that of other Middle Eastern populations, such as those in Lebanon and Saudi Arabia (3.9% and 3%, respectively),32,33 as well as South Asian populations, in which rates of 2.7% and 4% were reported in two Indian studies.23,24 However, the rate is lower than those of 7.1% and 7.8% recorded in Spain and the USA, respectively,19,20 as well as rates of 5% and 9% in two earlier Tunisian studies.25,26
In line with most previous reports5,21–24,34 we found that ALK-positive patients were significantly younger than those with ALK-negative tumors.
Although literature on the link between sex and ALK status shows varying results, female patients had higher rates of ALK positivity than male patients in most reports.5,21,34 In the present study, despite the limited number of positive cases, the difference between the sexes proved statistically significant. Several previous large-scale studies of ALK positivity in NSCLC did not detect a difference between sexes,19,35 whereas others found a higher rate in male patients.33,35 Thus, the connection between sex and ALK status in NSCLC is inconsistent, and the relationship might vary by race. Additional data from the Middle Eastern population are required in this regard.
Our present study also reported a substantial effect of smoking status on the frequency of ALK positivity, with the rate being higher in non-smokers or light smokers, a finding that is consistent with the majority of reports in the literature.21,34,36
Most of the patients included in our study had adenocarcinoma based on selection per the ASCO/CAP guidelines, except in some instances in which clinical features indicated a higher probability of an oncogenic driver (e.g., age <50 and light or absent tobacco exposure). Of the non-adenocarcinomas, none had ALK rearrangement.
The current study revealed a good concordance between FISH and IHC results for the identification of ALK-positive NSCLC, with a sensitivity of 87.5% and a specificity of 96%, in line with the findings of earlier studies.24,37–39 According to Wynes et al., IHC for ALK has a sensitivity of 90% and a specificity of 95% compared with FISH for ALK. 40 Furthermore, we had a single patient with positive IHC findings for ALK (D5F3) and a negative FISH result who had a significant response to ALK TKIs, which supports the conclusions of Cabillic et al. and Van der Wekken et al. that IHC for ALK is a better predictor of the response to targeted therapy than FISH when laboratories follow proper procedures.17,41
The other discordant case was an ALK IHC-negative patient with an ALK FISH-positive result. This form of discordance has been described in a few studies, and it might be attributable to a lower proportion of tumor cells carrying the rearrangement or to technical errors. Nonetheless, the clinical outcomes of patients with contradictory FISH and IHC results have not been consistent regarding the superiority of either technique.15,41
In conclusion, ALK rearrangement was detected in 4% of patients with NSCLC in a cohort in Jordan. IHC is an acceptable alternative to FISH for ALK testing with reasonable sensitivity and specificity, and it has advantages in terms of robustness, turnaround times, and cost-effectiveness. Even in situations in which ALK is negative with FISH, ALK positivity with IHC is correlated with the tumor response to ALK inhibitors.