
Abstract
Objective
Anastomotic leakage (AL) is the most serious postoperative complication following anterior resection for rectal cancer. We aimed to investigate the efficacy of active drainage for the management of AL.
Methods
This was a retrospective study using information from a database of patients who underwent colorectal resection without a defunctioning ileostomy at our center between September 2013 and January 2021. We identified 122 cases with definitive AL who did not require revision emergent laparotomy. Among these patients, we evaluated those who received active drainage to replace the original passive drainage.
Results
There were 62 cases in the active drainage group and 60 cases in the passive drainage group. The active drainage group had a shorter mean AL spontaneous resolution time (26.9 ± 3.3 vs. 32.2 ± 4.8 days) and lower average hospitalization costs (82,680.6 vs. 92,299.3 renminbi (RMB)) compared with the passive drainage group, respectively. Moreover, seven patients in the passive drainage group subsequently underwent diverting stoma to resolve the Al, while all ALs resolved spontaneously after replacing the passive drainage with active drainage.
Conclusions
Our study suggests that active drainage may accelerate the spontaneous resolution of AL.
Introduction
Anastomotic leakage (AL) after surgical resection for rectal cancer is a common and serious complication, with an incidence ranging from 2.2% to approximately 19%.1,2 AL significantly increases postoperative morbidity, requires a prolonged hospital stay, 3 and results in death in some patients who require further surgical intervention. 4 These issues decrease patients’ quality of life and the oncologic therapeutic outcomes. 5 To enhance patients’ quality of life, in addition to the need to prevent the high-risk factors for AL, the fundamental challenge is resolving the leakage quickly and avoiding the need for a diverting stoma.
Currently, the management of AL following anterior resection for rectal cancer comprises two main options: conservative treatment and surgical intervention. Conservative management is suitable for Grade A/B AL 6 and comprises maintaining drain patency, antisepsis, nutritional supplementation, and other comprehensive measures.7,8 Grade C leakage is managed with emergent or elective surgery.6,9 Emergent surgery is essential to save the lives of critical patients. Elective surgery mainly refers to creating a defunctioning stoma, which can shorten hospital duration but requires more operations, impairs patients’ health and quality of life, and increases medical costs.10,11 Recently, novel treatments for AL have been developed, such as vacuum-assisted closure in coloproctology and secondary sutures.12,13 These methods accelerate AL closure, although the success rate is unsatisfactory because of several factors.
Most postoperative AL after anterior resection can resolve spontaneously with effective drainage. The exception is cases of massive dehiscence causing diffuse peritonitis, which requires emergency laparotomy.12,14 In this study, we retrospectively analyzed the treatment outcomes of 122 cases of AL to determine whether active drainage effectively enhances spontaneous resolution of AL.
Materials and methods
The reporting of this study conforms to the STROBE guidelines. 15
Patient characteristics
Eligible cases comprised the following: (1) pathological diagnosis of rectal cancer after surgery; (2) radical proctectomy without a protective stoma; and (3) diagnosis of postoperative AL in accordance with the clinical manifestations and confirmation with a water-soluble contrast X ray study and computed tomography (CT). The exclusion criteria were as follows: (1) non-malignant tumor confirmed by postoperative pathology; (2) colorectal palliative surgery and by-pass procedure; and (3) AL with diffuse peritonitis requiring emergent reoperation (Figure 1).

CONSORT flow diagram.
General information
After institutional review board (IRB) approval, we performed a retrospective chart review of patients with postoperative AL following anterior resection for rectal cancer in the Department of Gastrointestinal Surgery at the Affiliated Hospital of Qingdao University between September 2013 and January 2021. All patients underwent preoperative routine laboratory blood examination to evaluate liver and renal function, cardiopulmonary function testing, abdominal and chest CT, pelvic magnetic resonance imaging (MRI), and colonic and rectal endoscopy. Some patients underwent preoperative chemoradiotherapy following a multidisciplinary consultation, and all patients underwent standard radical surgery for colorectal cancer. Postoperative AL was determined according to the following: suspicious or definitive fecal outflow from the drain followed by confirmation using a water-soluble contrast X ray study via the drain, and additional CT to identify a localized collection of fecal material or abscess around the anastomosis.
AL management
The retrospective data analysis showed that conservative management was the first-choice therapy, except for patients who underwent emergency reoperation to treat obvious manifestations of severe abdominal pain, abdominal distension, high fever, and diffuse peritonitis. Conservative management comprised the following: (1) maintaining unimpeded drainage by intermittently flushing the drain with saline or replacing the original passive drain with a dual-lumen active drainage cannula (Figure 2) at least 1 week postoperatively; (2) fluids to maintain homeostatic balance; and (3) parenteral nutrition combined with enteral nutritional supplementation and a residue-free diet. For effective drainage, the replacement cannula needed to be properly located around the anastomosis site, connected to continuous suction (0.02–0.04 Mpa), and irrigated with water. The active drain was constructed as follows: an efferent suction tube was placed inside an outer silicone tube with side holes, with the end of the outer tube connected to a slim afferent tube supplying continuously circulating water. The efferent tube was connected to negative pressure suction, and the afferent tube was connected to a continuous water irrigation system.

Active drainage cannula (dual-lumen drain, diameter: 8 mm) (a) efferent tube (inner tube with a diameter of 6 mm) connected to continuous suction; (b) afferent tube (diameter: 3 mm) connected to water irrigation.
The original passive drain was replaced with an active drain, as follows: A percutaneous passive drain was routinely placed near the anastomosis after rectal surgery. Once AL was definitively diagnosed, usually 8 to 9 days postoperatively when the sinus tract around the original passive drain had formed tightly, an active drain (Figure 2) with a similar outer diameter to the original passive drain was quickly inserted along the sinus tract as the original drain was removed. The active drain was then fixed securely to the skin. The depth of the active drain within the pelvic cavity was the same as that for the original passive drain. CT was used to verify whether the drain was at the appropriate location near the anastomosis.
Curative criteria
AL was considered resolved when patients had no pelvic and abdominal symptoms, no feces outflow from the drain, and a water-soluble contrast X ray study confirmed AL resolution, which was confirmed by pelvic CT to ensure there was no fecal collection around the anastomosis.
Statistical analysis
The SPSS version 17.0 statistical software package (Chicago, IL, USA) was used for statistical analysis. Discrete variables between the two groups were compared by the Chi-square test (or Fisher’s exact test, where necessary) while continuous data were presented as mean ± standard deviation (SD) and were assessed using Student’s t-test. Two-sided P < 0.05 was considered statistically significant.
Results
Our institution treated approximately 600 cases of anterior resection for rectal cancer per year during the study period, and the AL incidence was 4.2%. From September 2013 to January 2021, we identified 177 patients diagnosed with AL. After excluding 55 cases for various reasons, 122 patients with AL were retrospectively analyzed. Among the 122 patients, 60 patients received passive drainage accompanied by intermittent saline flushing to maintain unimpeded drainage, while 62 patients had the original passive drain replaced with a dual-lumen drain with continuous saline irrigation to maintain drain patency. Sex distribution, the height of the anastomosis from the anal verge, preoperative chemoradiotherapy, major laboratory examination results, and operative approaches were comparable between the two groups (Table 1).
Patient characteristics and preoperative factors.

Continuous data are presented as mean ± SD; other values indicate the number and percentage of patients.
ALT: alanine transaminase; AST: aspartate transaminase; AL: anastomotic leakage; SD: standard deviation.
The average time to spontaneous AL resolution in the active drainage group was 5 days shorter than that in the passive drainage group (26.9 ± 3.3 vs. 32.2 ± 4.8 days, respectively; P < 0.001), and the duration of supplemental parenteral nutrition was significantly shorter in the active drainage group compared with the passive drainage group (20.4 ± 4.0 vs. 25.6 ± 5.0 days, respectively; P < 0.001). Importantly, AL in all patients in the active drainage group resolved spontaneously, and seven patients in the passive drainage group subsequently received a diverting ileostomy to resolve the AL (P = 0.006). The retrospective data analysis showed that ileostomy was performed approximately 1 month after the occurrence of AL, and that two patients did not undergo stoma reversal because of stenosis of the anastomosis during follow-up. Moreover, the mean hospitalization cost for AL was approximately 10,000 RMB less in the active drainage group than that in the passive drainage group (Table 2).
Outcomes of active vs. passive drainage in managing anastomotic leakage.
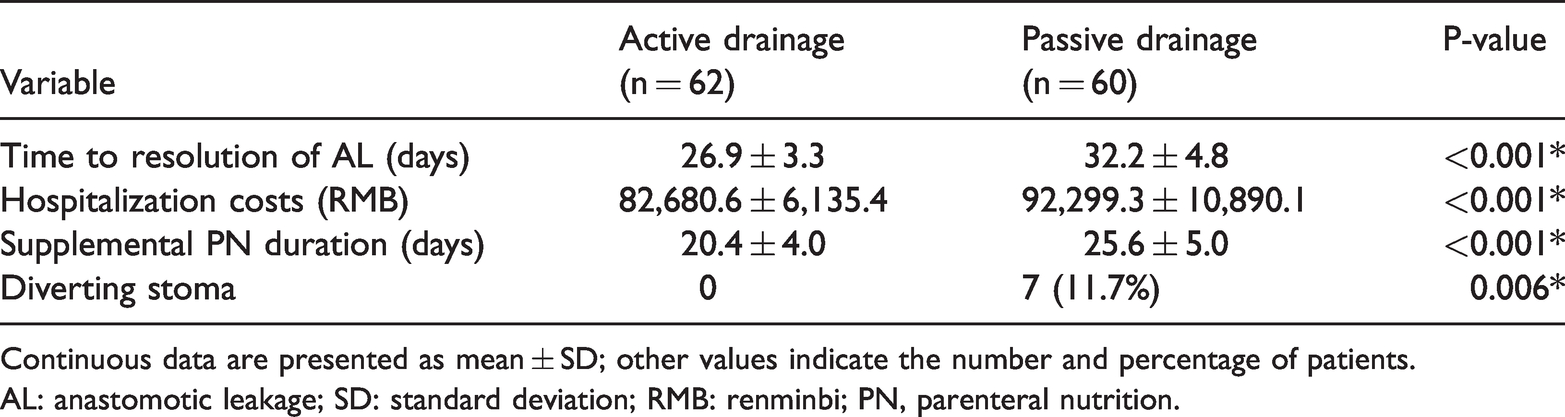
Continuous data are presented as mean ± SD; other values indicate the number and percentage of patients.
AL: anastomotic leakage; SD: standard deviation; RMB: renminbi; PN, parenteral nutrition.
Discussion
AL is a major postoperative complication after colorectal surgery and is associated with high postoperative morbidity and mortality, functional defects, and poor oncologic outcomes.4,5,16,17 AL is defined as a defect in the bowel wall integrity at the zone of attachment between the colon and the rectum that leads to communication between the intestinal lumen and the pelvic cavity. There is no universal grading for AL; however, a three-grade scale proposed by the International Study Group of Rectal Cancer in 2010 is often used for rectal cancer. 6 Grade A requires no therapeutic intervention, and grade B comprises active intervention without laparotomy; if laparotomy is required, the leakage is classified as grade C. 6 However, AL treatment should be guided by the severity and dynamic variation in the patients’ clinical manifestations. In our clinical practice, we found that the AL grade can change depending on the management modality. For example, if the AL is managed properly and timely, even patients presenting with symptoms and signs of fever, abdominal pain, and peritonitis (initially diagnosed as grade C) can avoid reoperation and experience AL resolution with conservative treatment.
Patients with symptomatic AL usually present with fecal discharge from the pelvic drain, and all of the subsequent consequences are caused by the fecal discharge. 18 If the fecal discharge is effectively eliminated, the local tissue edema and inflammatory response will be limited, which results in a strong possibility of spontaneous AL resolution when combined with improved nutritional status. In comparison, it is difficult to explore and suture the AL site because of the severe tissue edema and adhesions around the anastomosis in the narrow pelvic cavity. Additionally, surgical intervention often results in a high frequency of abdominal and pelvic cavity flushing and the need for a proximal intestinal segment stoma to divert the intestinal contents while waiting AL closure.19–21 Therefore, salvage of the anastomosis is very important in early grade A or grade B AL, when proper conservative strategies comprising effective fecal drainage and other comprehensive measures can prevent progression to a stage requiring reoperation. 22
Maintaining drain patency is the cornerstone of AL treatment. The fundamental principle of conservative AL management is to maintain effective and unimpeded evacuation of feces, reduce fecal contamination and bacterial infection, and maintain a clean environment around the anastomosis site to facilitate spontaneous AL healing. In our previous study, we found that active drainage significantly decreased the severity of pancreatic fistula and the associated complications following pancreaticoduodenectomy. 23 The novel active drain used in our previous and current studies comprises an efferent suction tube inside an outer silicone tube with side holes, and the end of the outer tube is connected to a slim afferent tube that supplies continuously circulating water to maintain drain patency. When the efferent tube is connected to negative pressure suction and the afferent tube is connected to continuous water irrigation, the drain acts as a continuous suction pump to efficiently evacuate fecal collection within the pelvic cavity. Compared with conventional passive drainage, active drainage can effectively eliminate collected fecal material and exudate to reduce retention of pollutants around the AL and promote spontaneous resolution of the leakage.
The current study demonstrated that replacing passive drains with active drains led to a 5-day shorter average AL resolution time compared with the resolution time in the passive drainage group. The hospital stay in the passive drainage group was comparable to the average hospital stay associated with AL (36.2 days) reported by Shinji et al. 24 We speculate that active drainage can effectively eliminate intestinal excretions, thereby reducing the incidence of serious complications, such as infection and erosion of the anastomosis, and promote spontaneous AL resolution. This speculation is consistent with a previous report by Kinugasa et al. 25 indicating that open drainage was associated with a much lower incidence of postoperative leakage compared with closed drainage.
Surprisingly, all patients with AL in the active drainage group experienced spontaneous AL resolution, whereas seven patients receiving passive drainage subsequently received a diverting stoma to resolve the AL. Two of the patients who received a diverting stoma did not undergo stoma reversal because of anastomosis stenosis. Active drainage is the most important factor for accelerating AL resolution. The potential underlying mechanism for this acceleration may be effective elimination of exudate around the colorectal anastomosis, thereby providing a clean environment for tissue regeneration. The advantages of active drainage promote wound healing, resulting in short hospitalization duration and lower hospital costs compared with passive drainage. However, the exact mechanism underlying AL resolution with active drainage must be validated in prospective randomized controlled trials and related animal experiments.
Our study has limitations. First, the single-institution, retrospective design made it difficult to avoid bias in patient selection and data collection. Second, all eligible participants developed AL after colorectal cancer resection; no other diseases were involved. Additionally, the sample size is relatively small. Third, the operations were performed by different surgical teams, and AL management strategies varied greatly, with some patients receiving active drainage early after original passive drainage and others receiving passive drainage for longer periods. There was also variability in the therapeutic quality, which made the data unsuitable for propensity score matching and which may have created bias in the data analysis. Randomized controlled trials are needed to resolve these issues.
Conclusions
Via a retrospective, single-institutional study, we found that active drainage has the potential to reduce the spontaneous resolution time of AL, and is a proposed alternative for patients with a high risk of developing AL following anterior resection for colorectal cancer.
Supplemental Material
sj-pdf-1-imr-10.1177_03000605211065942 - Supplemental material for Retrospective study of active drainage in the management of anastomotic leakage after anterior resection for rectal cancer
Supplemental material, sj-pdf-1-imr-10.1177_03000605211065942 for Retrospective study of active drainage in the management of anastomotic leakage after anterior resection for rectal cancer by Xiaojie Tan, Mei Zhang, Lai Li, He Wang, Xiaodong Liu and Haitao Jiang in Journal of International Medical Research
Supplemental Material
sj-pdf-2-imr-10.1177_03000605211065942 - Supplemental material for Retrospective study of active drainage in the management of anastomotic leakage after anterior resection for rectal cancer
Supplemental material, sj-pdf-2-imr-10.1177_03000605211065942 for Retrospective study of active drainage in the management of anastomotic leakage after anterior resection for rectal cancer by Xiaojie Tan, Mei Zhang, Lai Li, He Wang, Xiaodong Liu and Haitao Jiang in Journal of International Medical Research
Footnotes
Availability of data and materials
All data and materials are available upon request.
Authors’ contributions
Conceptualization and design of the study: HT Jiang and XJ Tan. Data acquisition: Tan, Zhang, Wang, and Liu. Analysis and interpretation of the data: Tan, Li, and Zhang. Drafting the manuscript: Tan and Zhang. Critical revision of the manuscript: HT Jiang and Liu. Supervision of the study: Jiang.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Ethics approval
This study was approved by the medical ethics committee of the Affiliated Hospital of Qingdao University (approval number: QYFYWZLL 26279). Written informed consent was obtained from all individual participants in this study, both for participation and for publication of their data.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and publication of this article: The study was supported by the Wu Jieping Medical Foundation (No. 320.6750.19089-47) to Haitao Jiang.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.