
Abstract
Objective
Anastomotic leakage (AL) is a frequent complication after laparoscopic rectal cancer resection (LRCR). The main objective of the present study was to identify accurate indicators of AL after LRCR.
Methods
A retrospective case-control study was performed of 185 patients who underwent laparoscopic surgery for rectal cancer between March 2012 and February 2017 at Beijing Friendship Hospital. Potential indicators of AL were examined via univariate and multivariate analyses. The performance of multivariate analysis was evaluated using receiver operating characteristic (ROC) curves.
Results
The overall AL rate was 17.84%. Multivariate analysis identified drainage smell (odds ratio [OR = 35.318, 95% confidence interval [CI] = 7.114 to 175.338) and peritonitis [OR = 17.475, 95% CI = 1.540 to 198.318) as independent indicators of AL. The area under the ROC curve was 0.720 (95% CI = 0.606 to 0.835).
Conclusion
Drainage smell and peritonitis could be reliable and accurate indicators of AL after LRCR.
Keywords
Introduction
Laparoscopic surgery for rectal cancer is safe and feasible,1,2 and it has become the preferred technique over open surgery. 3 An excellent surgical field is provided in a narrow pelvis by laparoscopic surgery during rectal resection. 4 Common complications are shared by laparoscopic and open surgery.
Anastomotic leakage (AL) following laparoscopic rectal cancer resection (LRCR) is a common complication with high morbidity and mortality rates.5–9 The AL rate after LRCR has been reported to range from 6% to 28%. 1 , 9 , 10 The leakage rate increases when the anastomosis is located closer to the distal or infra-peritoneal region. 11 There are several risk factors that helps to predict leakage before and after surgery, but indicators are signs and symptoms which help to suspect the AL after surgery.
Recently, elevated C-reactive protein levels after rectal resection for rectal cancer were found to be predictive of infectious postoperative complications including AL, and they might be indicative of AL. 6 The other signs of AL after surgery, including postoperative fever, leukocytosis, abdominal pain, and abdominal pain, have been briefly explained in the literature. 12 These signs play vital roles as indicators of AL, but they are also associated with other surgical complications. Pelvic drainage serves as an indicator of anastomosis that reflects its integrity. 13 According to the experiences of different surgeons, clinical AL was indicated by the presence of clinical signs such as abnormal discharge from the pelvic drain tube (gas, pus, or feces), 3 , 4 , 14 peritonitis, 2 , 3 , 13 postoperative fever, 3 , 4 postoperative leukocytosis, 4 postoperative abdominal pain, 3 rectovaginal fistula, 4 or pelvic abscess. 4 If leakage is suspected, then abdominopelvic computed tomography (CT), 3 , 4 , 14 sigmoidoscopy, 4 , 14 rectal examination 4 , 14 or water-soluble contrast enema 4 should be conducted to confirm the diagnosis of AL. However, few studies have analyzed the indicators for AL after open rectal resection. In addition, no study has detailed the accuracy of indicators for AL after laparoscopic resection of the rectum to date.
The main objective of the present study was to identify specific and reliable indicators for AL after LRCR. To our knowledge, this is the first study to investigate the accuracy of indicators for AL.
Materials and methods
Study population
A retrospective case-control study was performed for patients who underwent laparoscopic surgery for rectal cancer at Beijing Friendship Hospital (Beijing, China) between March 2012 and February 2017. Patients with colorectal cancer, anorectal cancer, or inflammatory diseases and those who required conversion to laparotomy were excluded. The inclusion and exclusion criteria are presented in Figure 1. Based on the clinical signs and symptoms, patients were diagnosed with rectal cancer via biopsy, colonoscopy, and/or CT. Patients were distinguished and categorized into two groups: AL group and non-AL group. Postoperative clinical signs and symptoms (abdominal pain, abdominal distension, fever, leukocytosis, drainage smell, and peritonitis) were recorded retrospectively when they were manifested by patients before a diagnosis of AL. Body temperature, drainage fluid, peritonitis, abdominal pain, and abdominal distension were evaluated for 10 days after surgery. The white blood cell (WBC) count was measured using venous blood on postoperative days 1, 3, and 5 if no abnormalities were detected.

Flowchart of the inclusion and exclusion criteria.
The study was conducted in accordance with the Declaration of Helsinki and was approved by the Research Ethics Committee of Beijing Friendship Hospital (approved on 9 October 2017; IRB: 2017-P2-122-01). Informed written consent was obtained from all patients.
Definitions of clinical terms
AL after rectal resection was defined as communication between the intra- and extra-luminal compartments occurring because of a defect in the integrity of the intestinal wall at the site of anastomosis between the colon and rectum or between the colon and anus. A pelvic abscess or abscess close to the anastomosis site, recto-urethral fistula, or rectovaginal fistula was also considered to indicate AL.
Peritonitis was defined as the presence of at least three clinical signs and symptoms such as abdominal tenderness with abdominal guarding, rigidity, abdominal pain that worsened with movement, abdominal distension, fever, and leukocytosis.
Drainage smell was defined as a light to foul smell encountered from the pelvic drain tube in the presence of gas, feces, turbid fluid, purulent discharge, or infection. It was evaluated and documented for 10 days after surgery to track the anastomosis site.
Statistical analysis
Categorical variables were expressed as numbers and analyzed using the chi-squared or Fisher’s exact test. Continuous variables were expressed as the mean ± SD and analyzed using an independent-samples t-test. The variables and their association with AL were investigated in univariate and multivariate analyses using binary logistic regression, and the data were reported as odds ratios (ORs) and 95% confidence intervals (CIs). Two-tailed P < 0.05 denoted statistical significance. The multivariate analyses were conducted using the following covariates: drainage smell (Yes or No), peritonitis (Yes or No), and postoperative abdominal distension (Yes or No). Receiver operating characteristic (ROC) curve analysis was used to check the performance of the multivariate analysis for the indicators of AL. An area under the curve (AUC) of >0.5 was considered statistically significant for analyzing the accuracy of binary outcomes. SPSS software v22 (IBM, Armonk, NY, USA) was used for statistical analyses.
Results
Demographic characteristics
In total, 185 patients who underwent laparoscopic surgery for rectal cancer over the 5-year period were included in this study. The median age of surgically treated patients with rectal cancer was 62 years (range, 33–91). Thirty-three patients were diagnosed with AL after laparoscopic surgery (17.84%), including 24 men and 9 women. The mean age of patients with AL was 66.51 ± 9.87 years (range, 51–89), and the mean body mass index (BMI) was 24.08 ± 2.37 kg/m2 (range, 20.3–29.4). Among 33 patients with AL, one each had pelvic abscess and recto-urethral fistula. The median time to a diagnosis of AL was 3 postoperative days (range, 2–20).
The patient baseline information for the entire study group is summarized in Table 1. Drainage smell was found in 36.36% (n = 12) of patients with AL, compared with 1.32% (n = 2) patients in the non-AL group (P < 0.001). Among 185 patients, five exhibited peritonitis, including four patients (12.12%) in the AL group and one patient (0.66%) in the non-AL group (P = 0.004).
Baseline characteristics of the patients.
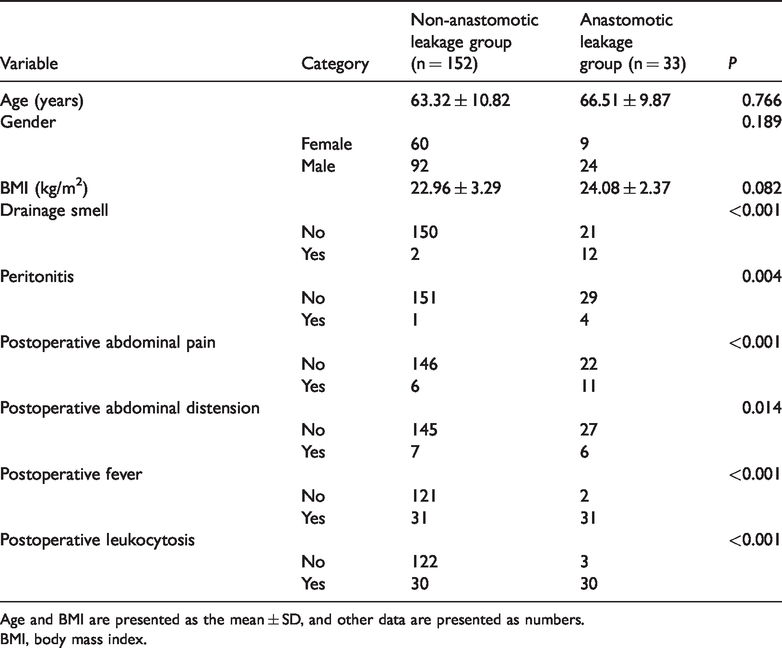
Age and BMI are presented as the mean ± SD, and other data are presented as numbers.
BMI, body mass index.
Univariate analysis
In univariate analysis, six clinical indicators of AL after laparoscopic surgery were evaluated. The results indicated that drainage smell (OR = 42.857, 95% CI = 8.960–204.982, P < 0.001), peritonitis (OR = 20.828, 95% CI = 2.246–193.122, P = 0.008), postoperative fever (OR =60.500, 95% CI = 13.726–266.664, P < 0.001), postoperative leukocytosis (OR = 40.667, 95% CI = 11.625–142.257, P = 0.001), postoperative abdominal pain (OR = 12.167, 95% CI = 4.086–36.225, P < 0.001), and postoperative abdominal distension (OR = 4.603, 95% CI = 1.435–14.761, P = 0.010) were significantly associated with AL, as presented in Table 2.
Univariate and multivariate analyses of the indicators of anastomotic leakage.
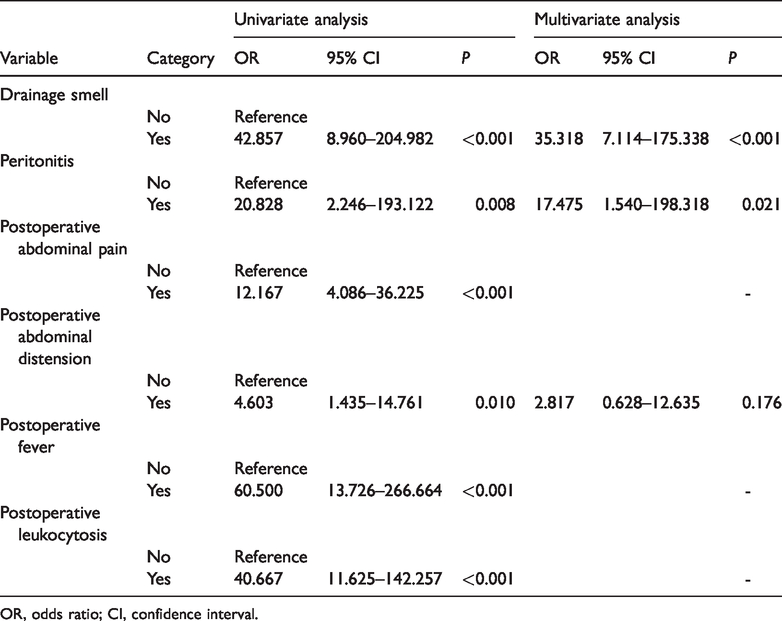
OR, odds ratio; CI, confidence interval.
Multivariate analysis
In multivariate analysis, drainage smell (OR = 35.318, 95% CI = 7.114–175.338, P < 0.001) and peritonitis (OR = 17.475, 95% CI = 1.540–198.318, P = 0.021) were identified as independent indicators of AL, as presented in Table 2.
Accuracy of multivariate analysis
The ROC curve was plotted according to binary outcomes, as presented in Figure 2. The AUC was 0.720 (95% CI = 0.601–0.835, P < 0.001).
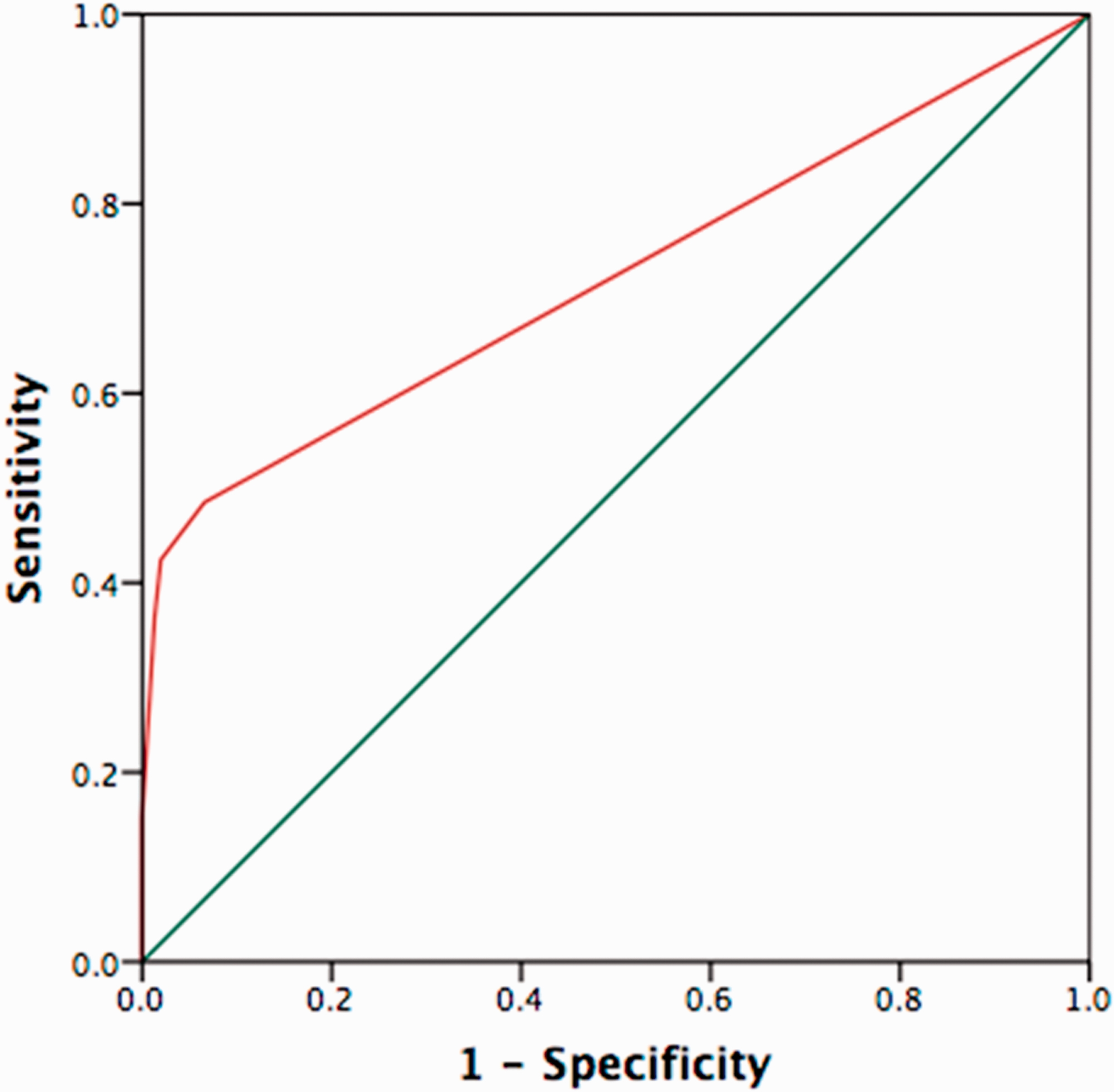
Receiver operating characteristic curve analysis of the performance and validity of the anastomotic leakage indicators.
Discussion
AL is the most bothersome complication after laparoscopic rectal resection associated with morbidity and mortality. The reported incidence rate of AL after laparoscopic surgery for rectal cancer varies from 6% to 28%. 3 , 9 , 10 In addition, Fukada et al. 3 and Hain et al. 9 recorded rates of 12.9 and 28%, respectively, after LRCR in their studies. The AL rate after LRCR was 17.84% in the present study, in line with previously reported results.
According to the present findings, drainage smell and peritonitis were significantly indicative of AL after LRCR. Postoperative fever, leukocytosis, abdominal pain, and abdominal distension were not predictive of AL after LRCR in this study.
Normal abdominal or pelvic fluid is odorless and clear to pale yellow in color. Cloudy or turbid abnormal fluid with a light to foul smell may be attributable to AL, perforated bowel, primary bacterial infection, or a strangulated or infracted bowel. In the case of AL, the cloudy and turbid appearance of pelvic drainage fluid and its foul smell are attributable to the presence of mixed colonic contents (gas, feces, or fluid). Tsujinaka et al. 13 mentioned that drainage can reflect the integrity of the anastomosis and facilitate the early diagnosis of anastomotic complications when bowel contents (gas, feces, pus, or excessive fluid) flow through the drain as an initial indicator of AL. Our result support this hypothesis, as drainage smell was identified as an accurate indicator of AL.
Peritonitis can be caused by spontaneous perforation or anastomotic disruption of the gastrointestinal tract after surgery. 15 , 16 In univariate and multivariate analyses, peritonitis was significantly associated with AL after laparoscopic surgery. Mulari et al. 16 indicated that peritonitis is related to anastomotic disruption, supporting our findings that peritonitis is a reliable indicator of AL.
Postoperative fever is an infectious symptom presenting 48 hours after surgery in the case of high body temperature or as a non-infectious symptom in the case of lower body temperature (<38.9°C). Fever can be caused by drugs, wound infection, respiratory tract infection, deep vein thrombosis, urinary tract infection, or intravenous injection. However, special attention is required if conditions such as anastomotic leakage, pulmonary embolism, alcohol withdrawal, adrenal insufficiency, myonecrosis, and malignant hyperthermia are present. 17 Postoperative leukocytosis is a nonspecific marker of a systemic inflammatory state, 18 which can be caused by surgery, infections, drugs, smoking, or anxiety. Abdominal distension explains the increase in abdominal girth with the sensation of increased abdominal pressure. It is frequently identified in patients with constipation and pelvic floor dysfunction. 19 After abdominal surgery, intestinal peristalsis slow or stops, leading to the accumulation of stagnant bowel contents and gas inside the intestine and giving rise to abdominal distension. Abdominal pain after surgery can be caused by anastomotic leakage, an insufficient analgesic drug dose in patients with incision wounds, urinary retention, constipation, or abdominal distension. Bellows et al. 11 observed postoperative fever, leukocytosis, abdominal pain, and/or abdominal distension in patients with AL, albeit as late signs. In the present study, these signs were identified in patients with and without AL, and thus, they were not accurate indicators of AL.
After analyzing the indicators for AL, the performance of the analysis was validated via ROC curve analysis, which confirmed the specificity and reliability of the results. Among postoperative indicators of AL after LRCR, drainage smell and peritonitis were confirmed as accurate indicators of AL after surgery. Conversely, other clinical indicators, including postoperative fever, leukocytosis, abdominal pain, and abdominal distension, were not specific for AL. These indicators can help surgeons identify AL promptly after surgery and prevent the deterioration of patient health.
The limitations of the present study included its retrospective design, single-institution nature, and insufficient sample size. Retrospective patient selection can lead to recall bias related to the details of medical history and data. Although peritonitis was an accurate indicator of AL in this present study, further studies with larger samples size are needed to evaluate the basic clinical indicators of AL because the number of patients with peritonitis in this study was small.
In conclusion, drainage smell and peritonitis could be reliable and accurate indicators of AL after LRCR. Hence, special attention should be paid to these symptoms if they appear after surgery.
Footnotes
Author contributions
Data collection: Enesh Shiwakoti, Jun Li, Jianning Song. Manuscript concept and design: Enesh Shiwakoti, Zhongtao Zhang. Manuscript preparation and drafting: Enesh Shiwakoti. Statistical analysis; Enesh Shiwakoti, Shanshan Wu. Critical review of subsequent drafts: all authors. Submission decision: all authors.
Declaration of Conflicting interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.