
Abstract
Takayasu’s arteritis is a rare, systemic, inflammatory vasculitis of large blood vessels with an unknown aetiology that more frequently affects women of childbearing age with progression to stenosis, fibrosis or thrombogenesis. Clinical manifestations are associated either with inflammation of the vascular wall (including fever, myalgia, arthralgia, weight loss) or the development of aneurysms and extensive vascular lesions, which creates challenges for a differential diagnosis. This current report presents the case of a female Caucasian patient, aged 23 years, that presented herself repetitively at the hospital reporting symptoms including fever, productive cough, myalgia associated with physical effort, arthralgia, inconstant headache, weight loss and altered general condition. The patient was diagnosed with Takayasu’s arteritis in the context of a prolonged febrile syndrome associated with reactive thrombocytosis. This association results in the need to exclude multiple differential diagnoses. Nonspecific management was initiated, which included antibiotic treatment, antifungal medication, anticoagulants, steroidal anti-inflammatory drugs and correction of anaemia. The patient slowly improved. Takayasu’s arteritis in the inflammatory phase associated with a prolonged febrile syndrome and reactive thrombocytosis is a rare diagnosis of exclusion of a multitude of inflammatory diseases of large blood vessels, infectious diseases and neurofibromatosis, which requires multiple investigations for an accurate diagnosis and management.
Keywords
Introduction
Takayasu’s arteritis, first described in Japan in 1908, is a rare type of vasculitis that was originally identified from changes in retinal blood vessels. 1 , 2 The highest incidence of the disease can be found in Asia (2.6 cases per million), followed by the USA (2.5 cases per million) and Europe (1.3 cases per million). 3
The aetiology of the disease remains unknown, but there are vascular changes that are dominated by a mononuclear and lymphocytes-rich inflammatory infiltrate that affect the vascular wall through the vasa vasorum. 4 Diagnosis of the disease, suggested by the clinical criteria, is confirmed by imaging techniques, but polymorphic symptomatology means that differential diagnosis is challenging and can even take up to 4 years from first symptoms. 4
This current case report presents the case of a 23-year-old female patient investigated for a 4-month long febrile syndrome and it describes the challenges associated with achieving a diagnosis.
Case report
In April 2018, a female Caucasian patient aged 23 years presented herself repeatedly at the Emergency Room of the Academic Emergency Hospital, Sibiu, Romania and at the Sibiu Pneumoftiziology Hospital, Sibiu, Romania for fever, productive cough, myalgia (predominantly in the upper limbs; especially the right limbs; and associated with physical effort), arthralgia in the interphalangeal joints of the upper limbs, inconstant headache, weight loss (8 kg in 4 months) and altered general condition. She was diagnosed with acute tracheobronchitis, for which she received symptomatic treatment. The biochemical evaluation performed on the first admission in the Sibiu Pneumoftiziology Hospital, Sibiu, Romania in May 2018, 2 months after the initial onset, revealed moderate anaemia, for which she was referred to the Department of Internal Medicine, Academic Emergency Hospital, Sibiu, Romania for admission. At the time of admission, on physical examination, the following changes were observed: pale underweight patient, with no skin rash with right submandibular and axillary adenopathy with multiple dental infections, heart rate of 100 beats per minute, blood pressure of 110/70 mmHg, no cardiovascular changes and with no signs of meningitis or neurological changes.
The laboratory examinations that were performed during hospitalization revealed a hypochromic microcytic anaemia, hyposideraemia, thrombocytosis, elevated transaminases, a marked inflammatory syndrome and the presence of fibrin monomers (Tables 1–3).
Main laboratory examinations during hospitalization in a 23-year-old female patient investigated for a 4-month long febrile syndrome.

Other laboratory examinations performed during hospitalization in a 23-year-old female patient investigated for a 4-month long febrile syndrome.

Laboratory examinations at a single time-point during hospitalization in a 23-year-old female patient investigated for a 4-month long febrile syndrome.
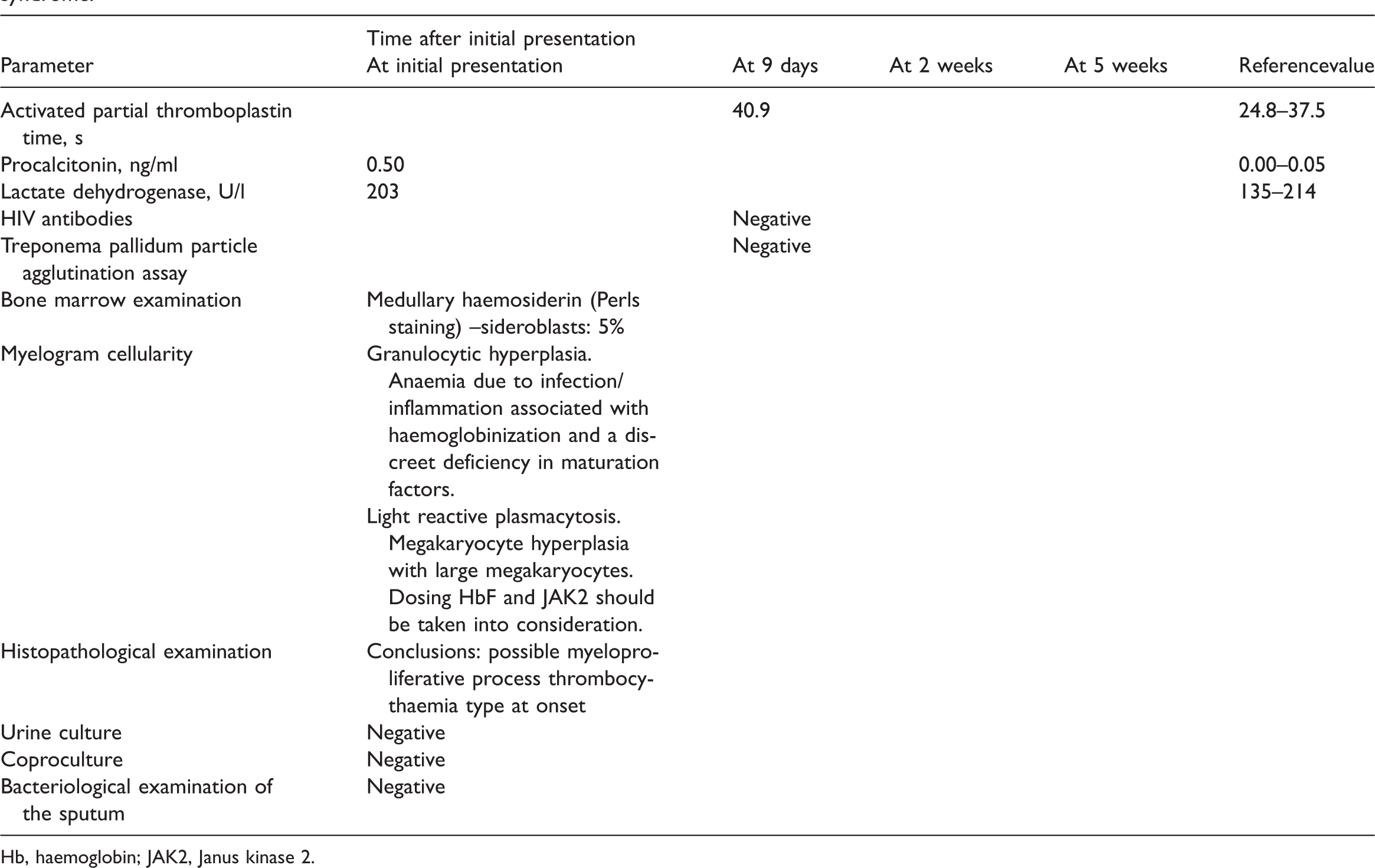
Hb, haemoglobin; JAK2, Janus kinase 2.
The patient was investigated for the exclusion of infectious endocarditis (transthoracic echocardiography), ear, nose, throat, genital and pulmonary infections. A native and contrast-enhanced thoraco-abdominal-pelvic multiple detector computed tomography (CT) scan with contiguous sections was performed and revealed no other changes besides a vesicular microlithiasis. Upper and lower gastrointestinal endoscopy were performed and revealed no changes. Dental treatments for apical periodontitis were performed under antibiotic protection, without influencing the febrile syndrome.
Further tests were conducted. The patient was investigated for the following: (i) tuberculosis (sputum and cultures for Mycobacterium tuberculosis were negative, and also the result of the QuantiFERON®-TB Gold test was negative); (ii) rheumatoid arthritis (rheumatoid factors and anti-cyclic citrullinated peptide antibodies were negative); (iii) systemic lupus erythematosus (antinuclear and anti-cardiolipin antibodies were negative, serum C3 and C4 levels were within the normal range); (iv) poly/dermatomyositis (repeated serum creatine kinase and lactate dehydrogenase within normal); (v) antineutrophil cytoplasmic antibodies-positive vasculitis (anti-neutrophil cytoplasmic antibodies were also negative); (vi) antiphospholipid antibodies were negative. The following pathologies were excluded: (i) Behçet’s disease (without oropharyngeal and genital lesions); (ii) Still’s disease (no characteristic rash or laboratory criteria); (iii) giant cell arteritis (age over 50 years and characteristic headache). The patient was referred to the Department of Haematology, Academic Emergency Hospital, Sibiu, Romania and the investigations were completed with a bone marrow examination that identified essential thrombocytosis, for which specific tests (i.e. Janus kinase 2 [JAK2]) were performed.
Her condition became slowly more favourable under antibiotic treatment (ceftriaxone that was used with levofloxacin and amikacin), antifungal medication, anticoagulants, steroidal anti-inflammatory drugs and correction of anaemia. She was discharged with no fever with the recommendation of ambulatory monitoring of body temperature and re-evaluation in case of fever.
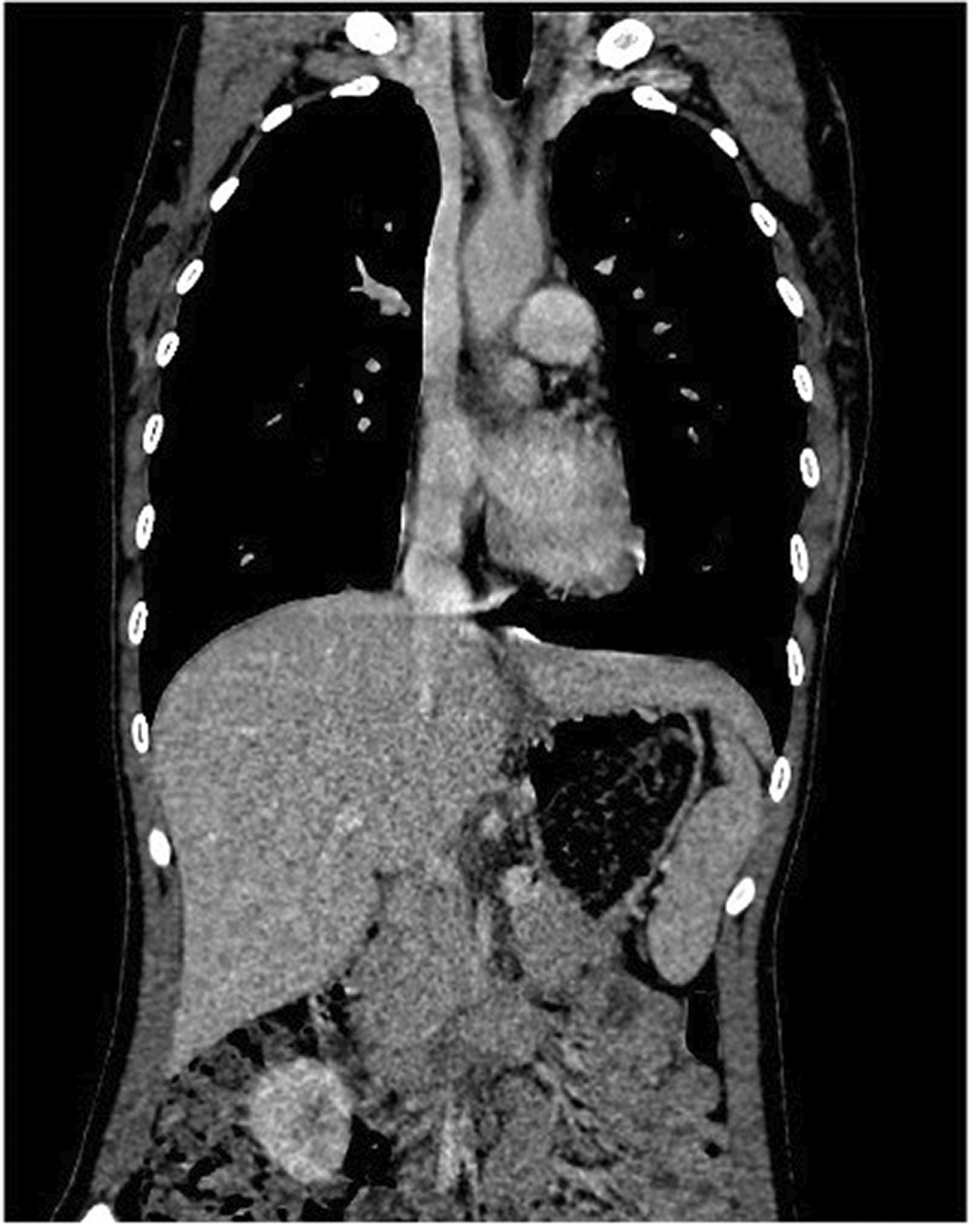
At 3 weeks after discharge, in June 2018, the patient returned to the Infectious Disease Department, Academic Emergency Hospital, Sibiu, Romania with 38 °C fever, headache, coughing, reversible visual disturbances, myalgias with the same characteristics as previously reported and lumbar pain. At the time of admission, on physical examination, the patient presented blood pressure differences, respectively blood pressure of 120/70 mmHg at the upper left limb and 90/60 mmHg at the upper right limb, murmur in the right subclavian artery, bilateral carotides and abdominal aorta, with palpable pulse including at the level of bilateral radial arteries. Investigations for the exclusion of autoimmune thyroiditis were performed, as well as a native and contrast-enhanced head multiple detector CT scan with contiguous sections was performed and revealed only a left temporal arachnidan cyst with a diameter of approximately 3.5 cm. A new contrast-enhanced thoraco-abdominal-pelvic multiple detector CT scan with contiguous sections and this time with reconstruction dedicated to vascular pathology was performed and revealed the following changes: discretely circumferentially thickened walls at the arch of the aorta (Figure 1), at the emergence of the brachiocephalic arterial trunk, at the emergence of the left common carotid (Figures 2, 3 and 4), with no flux or calibre changes at their level (Figure 5), as well as at the left subclavian artery (Figures 2 and 5). Focal stenosis at the emergence of the celiac trunk on a segment of approximately 6 mm (Figure 6). More pronounced stenosis of the upper mesenteric artery from the emergence on approximately 1.5 cm with stenosis aspect of about 50% (Figure 6). No pathological changes in the renal arteries were observed. Slight thickening of the arch walls, of the brachio-cephalic artery trunk and of the left common carotid artery. There was stenosis of the upper mesenteric artery in the proximal segment. There was discrete focal stenosis of the cephalic trunk emergence.

Computed tomography scan section of a 23-year-old female patient investigated for a 4-month long febrile syndrome that shows discretely circumferentially thickened walls at the arch of the aorta.

Computed tomography scan section of a 23-year-old female patient investigated for a 4-month long febrile syndrome that shows discretely circumferentially thickened walls at the left subclavian artery.
Computed tomography scan section of a 23-year-old female patient investigated for a 4-month long febrile syndrome that shows discretely circumferentially thickened walls at the emergence of the brachiocephalic arterial trunk and at the emergence of the left common carotid.

Computed tomography scan section of a 23-year-old female patient investigated for a 4-month long febrile syndrome that shows discretely circumferentially thickened walls at the emergence of the brachiocephalic arterial trunk and at the emergence of the left common carotid.

Computed tomography scan section with reconstruction dedicated to vascular pathology of a 23-year-old female patient investigated for a 4-month long febrile syndrome showing no flux or calibre changes at the arch of the aorta, the brachiocephalic arterial trunk, the emergence of the left common carotid or at the left subclavian artery.

Computed tomography scan section of a 23-year-old female patient investigated for a 4-month long febrile syndrome showing focal stenosis at the emergence of the celiac trunk.
The patient was referred to the Department of Rheumatology, Academic Emergency Hospital, Sibiu, Romania for a decision regarding immunosuppressive therapy with methotrexate, azathioprine or leflunomide as a standard treatment or biologics in case of no respond to standard treatment.
The reporting of this case report conforms to CARE guidelines. 5 Written informed consent was obtained from the patient for publication of this case report. The study was approved by the Ethics Committee of the Academic Emergency Hospital, Sibiu, Romania (no. 06/2018) and they encouraged publication of the article.
Discussion
Takayasu’s arteritis is a systemic vasculitis of large blood vessels, more commonly seen in women up to the fourth decade of life, especially in Asia, which is characterized by damage to the aortic arch and to its associated branches. 4 The symptomatology is secondary to ischaemia or the formation of aneurysms with various localizations, leading to diagnostic confusion and sometimes to years of investigation. 4 Some research suggests that the time taken to confirm a diagnosis is four-times longer in children compared with adults. 3 Exceptional cases have been reported in infants. 6 At least three out of six criteria must be present for a diagnosis of Takayasu’s arteritis: (i) under 40 years of age; (ii) a difference of at least 10 mmHg between the systolic blood pressure in the upper limbs; (iii) the presence of claudication in one of the extremities; (iv) presence of murmurs in the subclavian or aortic arteries; (v) deceleration of brachial artery pulse; (vi) identification of arterial occlusion (aorta, main branches). 7
Up to 50% of cases present with general manifestations including fever, myoarthralgia and weight loss, but it can be also associated with cardiac manifestations including hypertension,8–13 cardiogenic shock, 10 myocarditis, 14 dilated cardiomyopathy 15 and acute myocardial infarction or anaemia. 16 Among the first cases, associations of radial and carotid pulse deficit with dyspnoea and weight deficiency were described. 1 However, there are also cases of neurological manifestations that present as visual disorders or stroke, 17 convulsions that present as recurrent 18 or postural vertigo, 19 jaw pain after chewing 20 and chest pain or nodal erythema. 20 Rarely, cases with onset of fever of unknown aetiology unaccompanied by weight loss, cataracts or Horner’s syndrome have been reported. 21
Renal artery stenosis, present in 23–31% of cases, causes malignant hypertension, heart failure or death. 22 In the literature, a single case was reported as being diagnosed after 3 years from the detection of thrombocytosis associated with general manifestations, which suggests that Takayasu’s arteritis should be included in the differential diagnosis of these manifestations. 23 Although it seems premature, the findings from this current case suggest that this is more common, probably not routinely evaluated and that it is also possible to measure fibrin monomers during the inflammatory episodes of Takayasu’s arteritis.
The current case was characterized by a marked inflammatory syndrome, leading to multiple differential diagnoses, from infections (sepsis, infectious endocarditis, tuberculosis, infections with Mycoplasma, Chlamydia, syphilis or HIV), collagenosis, haematological disorders (anaemia, thalassaemia, essential thrombocytosis, lymphoma, myeloma) and neoplasia. The presence of a prolonged febrile syndrome in the current case, which is only seen in <20% of cases at onset, 21 with persistent thrombocytosis (maximum values of 880 × 103/µl) and fibrin monomers, hyperfibrinogenaemia (associated with aortic inflammatory phenomena) and a significant increase in the erythrocyte sedimentation rate are all indicative of the inflammatory phase of Takayasu’s arteritis. In addition, intense inflammatory activity was also responsible for the patient’s moderate anaemia. Complete paraclinical examinations, in the absence of a careful physical examination, are not sufficient for the diagnosis of vasculitis in all cases.
In conclusion, Takayasu’s arteritis in the inflammatory phase associated with a prolonged febrile syndrome, reactive thrombocytosis, the presence of fibrin monomers and anaemia, is a rare diagnosis of exclusion of a multitude of inflammatory diseases of large vessels, infectious diseases and neurofibromatosis, which requires multiple investigations for an accurate diagnosis and management.
Footnotes
Author contributions
All authors contributed equally to this manuscript in terms of acquisition, analysis and interpretation of data, conception and design, and drafting the manuscript. All authors read and approved the final manuscript.
Declaration of conflicting interest
The authors declare that there are no conflicts of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.