
Abstract
Type I Takayasu’s arteritis is a rare form of large vessel vasculitis with an unknown etiopathogenesis. It is characterized by progressive chronic inflammation and occlusive thromboaortopathy affecting the aorta and its main branches. Type I Takayasu’s arteritis predominantly affects women and is most commonly observed in their third decade of life. In this report, we present the case of a 32-year-old female patient who exhibited severe long-segment stenosis in the left common carotid artery and total occlusion of the left subclavian artery. The patient experienced significant ischemic symptoms of the left upper extremity and had previously been diagnosed with Takayasu’s arteritis, being followed up under maintenance corticosteroid therapy. To address these complications, we conducted a surgical bypass using a prosthetic graft. The graft was inserted intrathoracically, extending from the patient’s ascending aorta to both the left common carotid artery and the left distal subclavian artery. This approach was designed to closely mimic anatomical routes, promoting optimal graft patency. In the context of this case, we highlight the importance of surgical intervention in alleviating ischemia and explore potential surgical alternatives for treating patients with Takayasu’s arteritis involving the supraaortic region.
Introduction
Takayasu’s arteritis (TA) is a rare systemic inflammatory disease of an unknown etiology and pathogenesis, characterized by progressive chronic inflammation, occlusive thromboaortopathy, and aneurysmal degeneration of the aorta and its main branches. TA commonly presents in the second or third decade of life among women. 1 Infection with Mycobacterium tuberculosis and specific HLA alleles, namely HLA B52, DRB11502, DRB50102, DQA10103, DQB10601, and DPA102-DPB10901, have a clear association with TA. 1 Numerous findings have been identified that strengthen the argument for an autoimmune pathogenesis in TA. This is genetically linked to and involves an adaptive immune response, which leads to autoimmune damage against unknown autoantigens, playing a role in both its occurrence and recurrence.1,2
TA may involve not only the aorta itself but also its branches and pulmonary arteries. The disease is characterized by several distinct classifications. The commonly used Lupi-Herrera classification, based on the type of involvement, is anatomically categorized as follows: TA type I involves the aortic arch and its main branches, type II affects the descending aorta and/or abdominal aorta, type III encompasses the aortic arch and thoracoabdominal aorta, and type IV is associated with the pulmonary artery. 3 The manifestation of the disease also varies based on the geographic location. For example, in Japanese patients, involvement of the ascending aorta and its branches is more prevalent, while in India, there is a higher incidence of abdominal aorta and renal artery involvement. In North America, on the other hand, thoracic and abdominal aorta involvement tends to be more common. 4
The clinical spectrum can range from asymptomatic disease to severe ischemia. During the early phase of the disease, atypical symptoms and signs such as weakness, fatigue, loss of appetite, night sweats, weight loss, and arthralgia may emerge, typically accompanied by a high erythrocyte sedimentation rate (ESR) and anemia. The definitive diagnosis is often delayed, and this active period gradually evolves into the chronic phase within months. In the later stages of the disease, ischemic symptoms can arise due to stenosis and occlusions. These include intermittent claudication, rest pain, weakening and loss of pulses, as well as manifestations such as Raynaud’s phenomenon, murmurs, arterial aneurysms, and aortic valve insufficiency resulting from ascending aortic enlargement. Additionally, congestive heart failure, myocardial infarction, and hypertension due to renal artery stenosis can develop. Other complications include renal failure, mesenteric angina, vision loss, stroke, epileptic attacks, amaurosis fugax, and dizziness. During the natural progression of the disease, active and inactive periods alternate. This can lead to limitations in daily activities and loss of function.
In this case report, we describe a successful intrathoracic bypass operation. The operation involved connecting the ascending aorta to the left common carotid artery and the distal portion of left subclavian artery. The procedure was performed on a young female patient who had been previously diagnosed with TA. The patient was referred to our clinic due to symptomatic involvement of the aortic arch branches and critical ischemia in the left upper extremity. Despite previous medical treatment, her vascular disease had progressed.
Case report
A 32-year-old female patient was diagnosed with TA approximately 5 years ago, following a process that started with deep vein thrombosis in her left lower extremity in her home country. Since then, she has been receiving medical treatment for TA and undergoing routine follow-up with internists. About 2 months before her referral to our hospital, she started experiencing pain in her left arm and hand during daily activities. However, during this period, the severity of pain progressed rapidly to the point where it transitioned to rest pain that could not be managed with her usual pain medication. As a result, the patient was referred to our clinic for intervention due to possible arterial insufficiency resulting from TA.
Upon initial observation, it was evident that the patient’s daily activities have been severely limited, and her sleep pattern as well as overall quality of life have been severely compromised due to ischemic pain. In the physical examination, aside from the indications of arterial insufficiency such as coldness and pallor in her left hand and forearm, cyanosis, atrophy in the thenar and hypothenar muscles, and the absence of left axillary, brachial, and distal arterial pulses, no other significant issues were detected. The patient’s current medication regimen included 5 mg oral prednisolone maintenance therapy for TA, 25 µg of thyroid hormone for hypothyroidism, and newly introduced antiplatelet therapy comprising clopidogrel 75 and 100 mg of acetylsalicylic acid.
Patient’s laboratory values were as follows: ESR: 11 mm/h (N: 0–20), C-reactive protein (CRP): <0.2 mg/dL (N: 0–0.5), leukocyte count: 7.34 × 109/L (N: 4.5–11), hemoglobin: 10.9 g/dL (N: 10.8–14.9), and platelet count: 213 × 109/L (N: 140–400).
Conventional angiography and computed tomographic angiography revealed that a total occlusion of the left subclavian artery starting from its origin at the aorta (approximately 4.5 cm length), with weak collaterals filling the distal portion. Additionally, the left common carotid artery showed short segment (approximately 1.5 cm) of pre-occlusive narrowing up to the middle just after its origin (Figure 1).
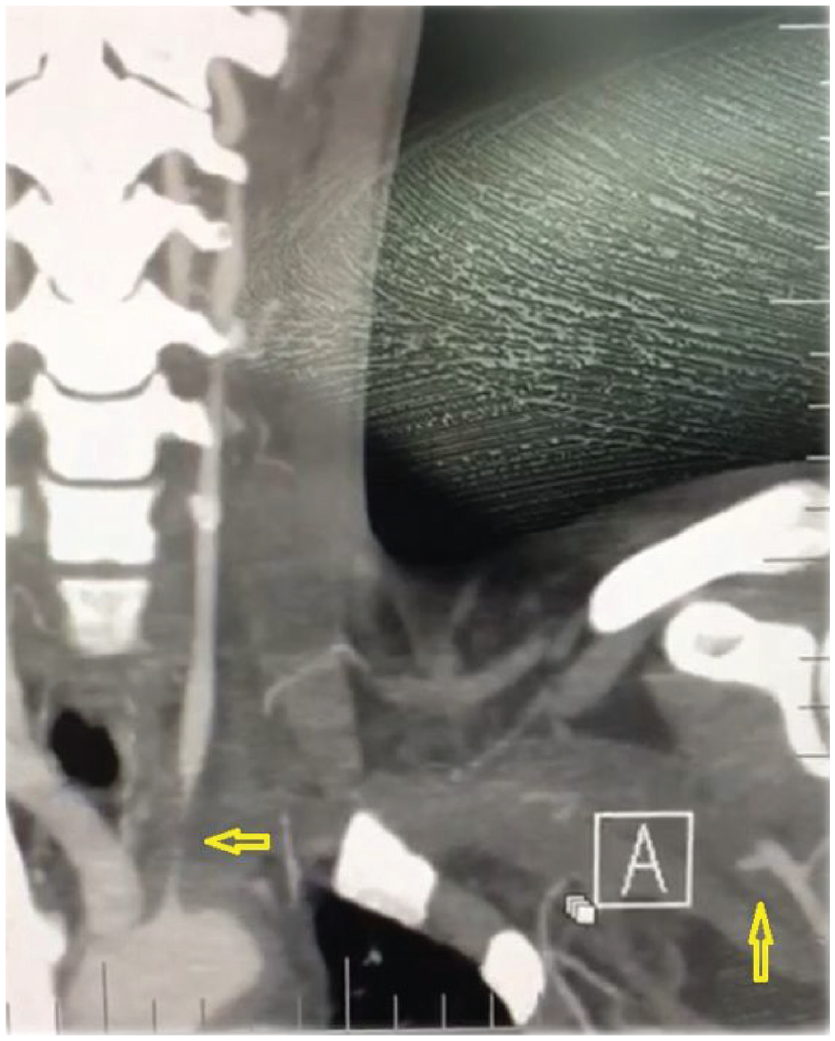
Computed tomographic angiography, coronary section. Occlusion of the left subclavian artery starting from its origin at the aorta, with weak collaterals filling the distal portion and left subclavian artery occluded from its division from the aorta, filled by weak collaterals in the distal part and the left carotid artery showing pre-occlusive narrowing up to the middle just after its origin.
Our patient met the criteria of American College of Rheumatology 1990 in terms of diagnosis. 5 Since CRP and ESR were within normal limits, it was determined that the disease was inactive. The current treatment was continued without any additional medical intervention, and the operation was planned.
Initially, the left common carotid artery and its bifurcation were checked with a neck incision, and the distal of the left subclavian artery was controlled with a subclavicular incision. Access to the ascending aorta was gained by opening the pericardium through median sternotomy. No pathologies such as thickening and plaque formation were not observed upon the examination of the ascending aorta. First, an 8-mm dacron graft was threaded through the mediastinum and anastomosed distally to the left common carotid artery, just beneath the bifurcation and proximally to the ascending aorta. Subsequently, another 8-mm dacron graft was introduced through the thoracic cavity at the level of the ascending aorta and the 2nd intercostal space, achieved by opening a window in the pericardium. The distal of the graft was then anastomosed to the distal portion of the subclavian artery, while the proximal end of the graft was anastomosed to the ascending aorta (Figure 2).

An 8-mm dacron graft was threaded through the mediastinum and anastomosed distally to the left common carotid artery. Subsequently, another 8-mm dacron graft was anastomosed to the distal portion of the subclavian artery and the proximal end of the graft was anastomosed to the ascending aorta.
There were no complications in the postoperative period, except for a mild headache. The preexisting ischemic complaints in the left hand improved dramatically, and all upper extremity pulses became palpable. The patient was discharged maintaining the same preoperative steroid and antiplatelet treatment. Subsequent clinical follow-ups over the course of 2 years revealed the absence of any complaints. Furthermore, the grafts remained patent, and the anastomoses showed no signs of obstruction in the follow-up CT angiography (Figures 3–5).
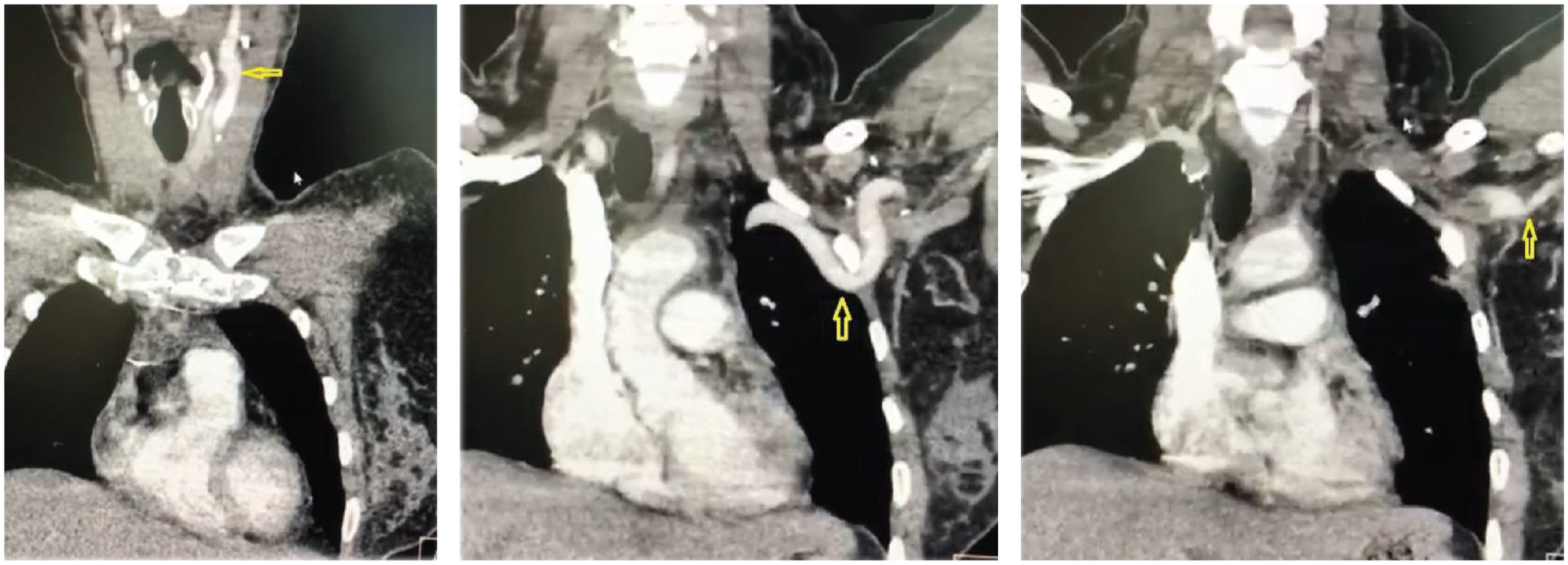
Coronal contract-enhanced thorax CT angiography images showed the patency of the graft and the proximal and distal anastomoses.
Discussion
TA is a rare chronic inflammatory disease that can result in organ and extremity ischemia. It progresses through panarteritis, involving the aorta and its main branches. While the aortic arch and the ascending aorta are less frequently affected by the disease, 6 the condition generally follows a chronic and recurrent course, leading to serious morbidity due to disease recurrences. In vascular pathology, segmental patchy granulomatous inflammatory lesions are observed across all three layers of the vessel wall in the aorta and its branches. Over time, these inflammatory processes lead to aneurysmal enlargement, stenosis, and thrombosis. 4
Early diagnosis and initiation of immunosuppressive therapy in TA can prevent the development of arterial stenosis and aneurysm, and the occurrence of clinical symptoms associated with them.7,8 Corticosteroids play an important role in medical treatment during both the active periods and the course of the disease. Additionally, methotrexate, cyclophosphamide, cyclosporine, and infliximab can be added to the treatment regimen or used as alternatives. However, the efficacy of antiplatelet agents, oral anticoagulants, and vasodilator drugs has not been fully established. 4
Although the primary treatment of TA is pharmacological, surgical and endovascular interventions may be required in addition to pharmacological treatment for organ and extremity ischemia, renovascular hypertension, and aneurysmal enlargement. 9
Revascularization techniques for TA encompass percutaneous transluminal angioplasty and stenting. In cases of short segment lesions, endarterectomy is employed. For complex lesions unsuitable for these interventions, widening with a patch or graft bypass is performed. 4
As observed in our patient’s vascular involvement, lesions affecting the supraaortic branches in TA tend to be longer, more diffuse, and exhibit greater thickness and fibrosis compared to those seen in atherosclerosis. 9 Experiences in angioplasty procedures are mostly with stenotic lesions and satisfactory results have been achieved through endovascular methods for short stenotic lesions without complete occlusion. Conversely, challenges may arise when dealing with total occlusions, and the risk of thromboembolism and vascular trauma is higher. It has been observed that the outcomes of endovascular interventions are not very encouraging, particularly in cases involving the origin of the subclavian artery. 6 Comparatively, endovascular interventions carry a higher risk of failure than surgical procedures do. Although they may exhibit favorable early success rates, there is a significant risk of future restenosis.4,6 Unlike lesions in atherosclerosis, lesions in TA tend to be longer and less amenable to endarterectomy. Additionally, it is noteworthy that symptoms in TA arise more from thrombosis rather than embolism. 9
Among the surgical procedures, patchplasty and endarterectomies exhibit lower patency rates.
Severe lesions affecting the subclavian and carotid arteries often necessitate supraaortic surgical reconstructions. These reconstructions aim to correct ischemic symptoms in the brain and upper extremities and mitigate the risk of stroke.
Surgical bypass is the standard treatment for symptomatic and irreversible supraaortic lesions, with supraaortic bypasses yielding favorable long-term outcomes. 6 These interventions enhance patients’ quality of life.
In our case, the total occlusion of the left subclavian artery from the aortic arch in the long segment and pre-occlusive narrowing of the left common carotid artery in the proximal long segment made us consider that direct bypass using a graft would be the most suitable approach. Severe ischemia threatening the extremity function in the left hand and arm was a definite indication. While neurological symptoms in atherosclerotic patients arise from cerebral infarctions caused by embolism, it is known that symptoms in TA patients result from global ischemia. 9 Our patient did not have any symptoms originating from the left main carotid lesion for the time being. However, the chronic progressive nature of the disease, the possibility of lesion development in the other carotid in the following years, and the long-segment severe stenosis in the left common carotid artery made us think that we could encounter global ischemic symptoms and stroke-like neurological problems in the future. However, since we devised a bypass route from the ascending aorta to the left subclavian artery, our estimation indicated the highest likelihood of patency extending from the ascending aorta to the distal portion of the left main carotid artery if performed in the same session. This approach was preferred due to the anticipated complexity and risks associated with any future attempt to bypass the long-segment pre-occlusive lesion of the left common carotid artery. Consequently, the decision was made to proceed with the planned graft bypass, as discussed.
In open surgical reconstructions, it is essential to avoid the affected segment to reduce the risk of restenosis. For this reason, distal bypasses were performed on the relatively intact and proximal regions of both affected vessels originating from the ascending aorta, where involvement is typically less frequent.
Compared to postoperative endovascular procedures, the rates of occlusion and neurological symptoms are significantly lower with bypass grafts. 9 However, surgical procedures are considerably complex and are accompanied with high perioperative complication rates. Moreover, the procedures themselves carry the potential for serious cardiac, pulmonary, and neurological morbidities.6,9
Aneurysm formation, infection, graft dehiscence, occlusion, and revision rates are higher compared to those who were operated on during the inactive period. 10 Consequently, whenever feasible, operations should be performed during the disease’s inactive phase, and it is advisable to maintain immunosuppressive treatment after the procedure. 9
Normal hemoglobin, ESR, and CRP values are the most commonly employed indicators to show the periods of disease inactivity. In suitable cases, 18F-FDG positron emission tomography can serve as a supportive diagnostic tool. Therefore, due to our patient’s urgent situation, we proceeded with the operation while the patient was undergoing her current steroid treatment, given that the ESR and CRP values we identified were within normal limits. Life-long medical follow-up by a multidisciplinary team, including rheumatology and cardiovascular surgery experts, is essential for these patients.
Conclusion
Despite the increased general operative risk factors associated with opening the left pleural cavity and pericardium−unlike extraanatomic bypasses− we opted to route the graft from the ascending aorta to the left subclavian artery.
This choice is rooted in our belief that it offers the most anatomically direct pathway for the graft and enhances the likelihood of sustained patency in the future.
Footnotes
Author contributions
The authors’ contributions to the article are as follows: C.A.: Conceived and designed the study, planned and performed the operation, and supervised and edited the article. Y.J.: Assisted with the operative procedure and contributed to data collection. R.H.: Collected data and drafted the article. All authors have participated in reviewing the results and have given their approval for the final version of the article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.